
Abstract
Objective
The Australian Institute of Health and Welfare publishes statistical indicator reports on the specialised mental health workforce. These include data for 2022–2023 on psychiatrists, mental health nurses, mental health occupational therapists, psychologists and mental health social workers. We provide a brief commentary on these reports, reflecting upon the implications of such changes for psychiatric practice and patient care.
Conclusions
Overall, there are fewer mental health workers with increasing distance from urban centres. There are insufficient rural psychiatrists with the NT and Queensland having higher rates per 100,000 in outer regional and remote areas. Psychologists and mental health nurses have the highest rates per 100,000 in rural areas. Though low in absolute rates per 100,000, mental health social workers are better distributed in rural compared to urban areas. Further data on public, private and non-governmental sector employment would be useful.
Keywords
The Australian Institute of Health and Welfare (AIHW) publishes statistical indicator reports on the specialised mental health workforce. These include data for 2022–2023 on psychiatrists, mental health nurses, mental health occupational therapists, psychologists and mental health social workers. 1 Based on previous research into the shortage of regional and remote workforce for psychiatrists, 2 we explore the current relative distribution of the range of specialised mental health workers in Australia, and comment upon the implications for service delivery, and patient access using the same dataset for all professions. 1 Previous research has shown that workforce levels are material considerations in the incidence of youth suicide hotspots, which were prevalent in rural and remote regions. 3
Although there seem to be no available corresponding data for general practitioners available from the AIHW, there are data on GPs from the Department of Health and Aged Care, albeit not specific to the mental health workforce. 4 These data reveal the following: ‘Under the baseline projections (where supply is assumed to meet demand in the 2023 base year) a shortfall of over 600 FTE in 2024, increasing to over 1900 FTE in 2028, and 6100 FTE by 2048. A shortfall in the number of GPs from the baseline projections of over 800 in 2024, increasing to over 2600 by 2028, and 8600 GPs by 2048’ 4 (p. 8).
Noting a holistic assessment of the regional and remote specialised mental healthcare services should also encompass mapping of specialised mental health facilities, community care facilities, models of care, and patient outcomes 5 – we have focussed on the most recent workforce distribution to simplify discussion of a key issue. There are also identified barriers to accessing mental health care in regional and remote Australia. 6 In this context, the relative regional and remote distribution in the AIHW data provide a snapshot of the current workforce challenges, relevant to clinicians, patients and policymakers.
The data are depicted in Figures 1–5, derived from the AIHW Mental health Workforce Spotlight webpage: Mental health workers, numbers and rate (per 100,000 population) by geographical distribution.
1
The AIHW states the data sources for the report are the National Health Workforce Dataset, the National Mental Health Establishments Database and the Australian Association of Social Workers.
1
Rate of psychiatrists per 100,000 population by remoteness classification. Source: Australian Institute of Health and Welfare, Mapbox, OpenStreetMap. Rate of psychologists per 100,000 population by remoteness classification. Source: Australian Institute of Health and Welfare, Mapbox, OpenStreetMap. Rate of mental health occupational therapists per 100,000 population by remoteness classification. Source: Australian Institute of Health and Welfare, Mapbox, OpenStreetMap. Rate of mental health nurses per 100,000 population by remoteness classification. Source: Australian Institute of Health and Welfare, Mapbox, OpenStreetMap. Rate of mental health social workers per 100,000 population by remoteness classification. Source: Australian Institute of Health and Welfare, Mapbox, OpenStreetMap.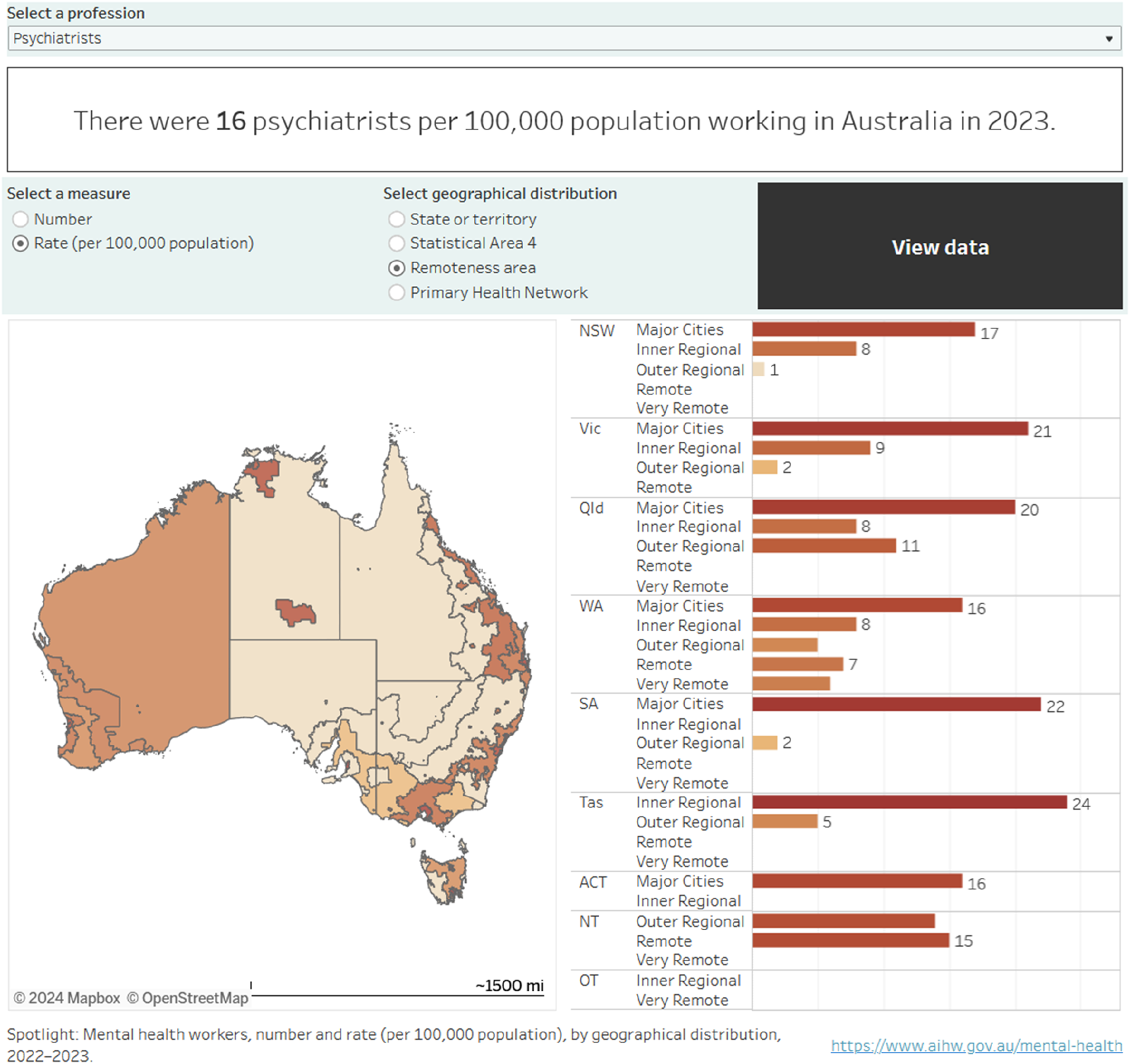
Psychiatrist geographical distribution per 100,000 (Figure 1)
With the exception of Tasmania, and the Northern Territory, which are classified as regional or remote for the majority of the most populous geographical areas, psychiatrists are located in major cities and inner regional areas. In the case of WA, psychiatrists are distributed across the whole range of metropolitan, regional and remote classifications.
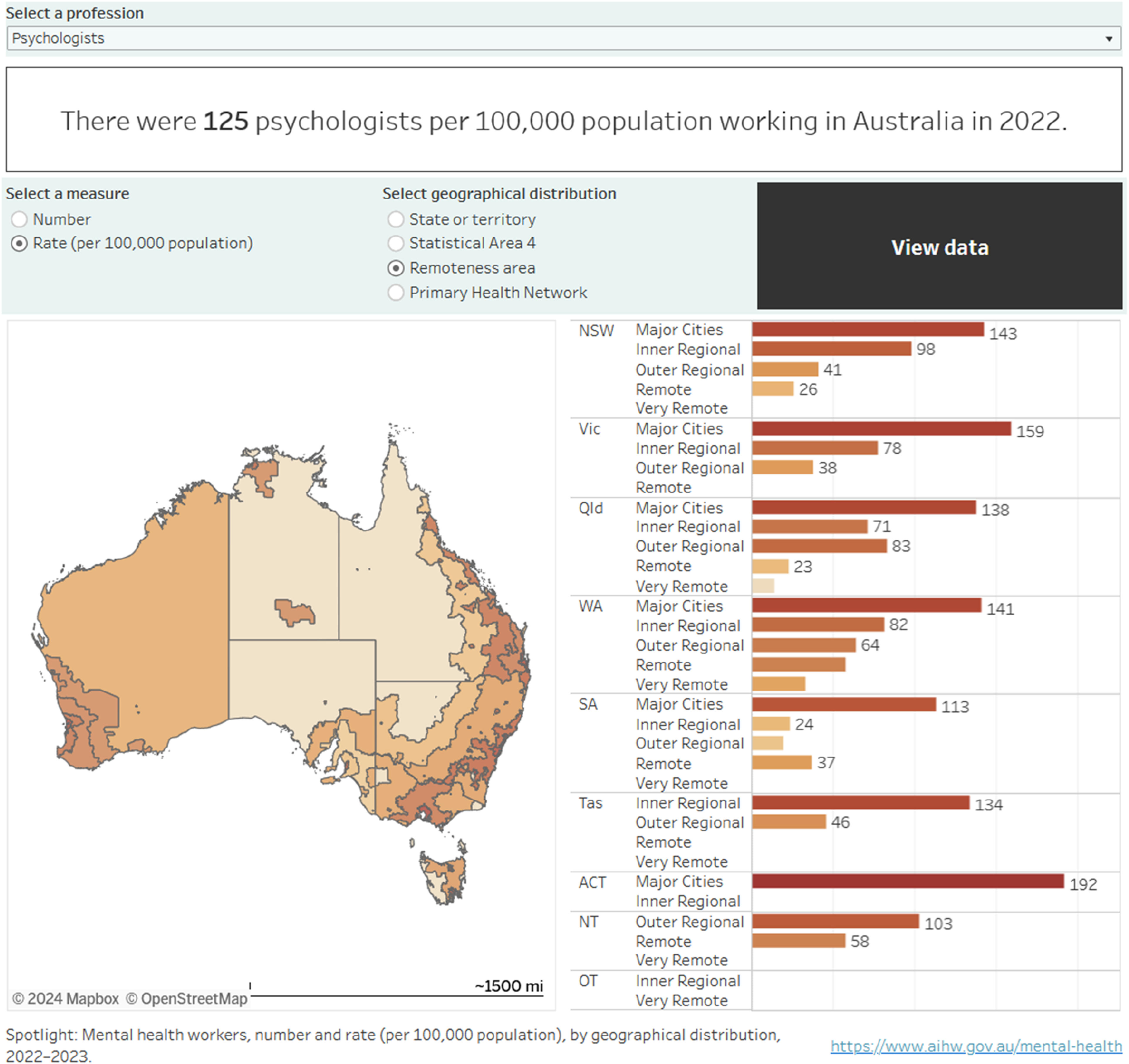
Psychologist geographical distribution per 100,000 (Figure 2)
Psychologist national numbers of 125 per 100,000, dwarf the distribution of psychiatrists at 16 per 100,000, and are higher than mental health nurses (96 per 100,000). Interestingly, the very highest rate of psychologists, 192 per 100,000 is found in the ACT. Relative to psychiatrists, there are substantial numbers of psychologists in inner and outer regional areas in all states, except the ACT, which is classified as a major city. However, the regional and remote distributions are somewhat lower in South Australia in particular.
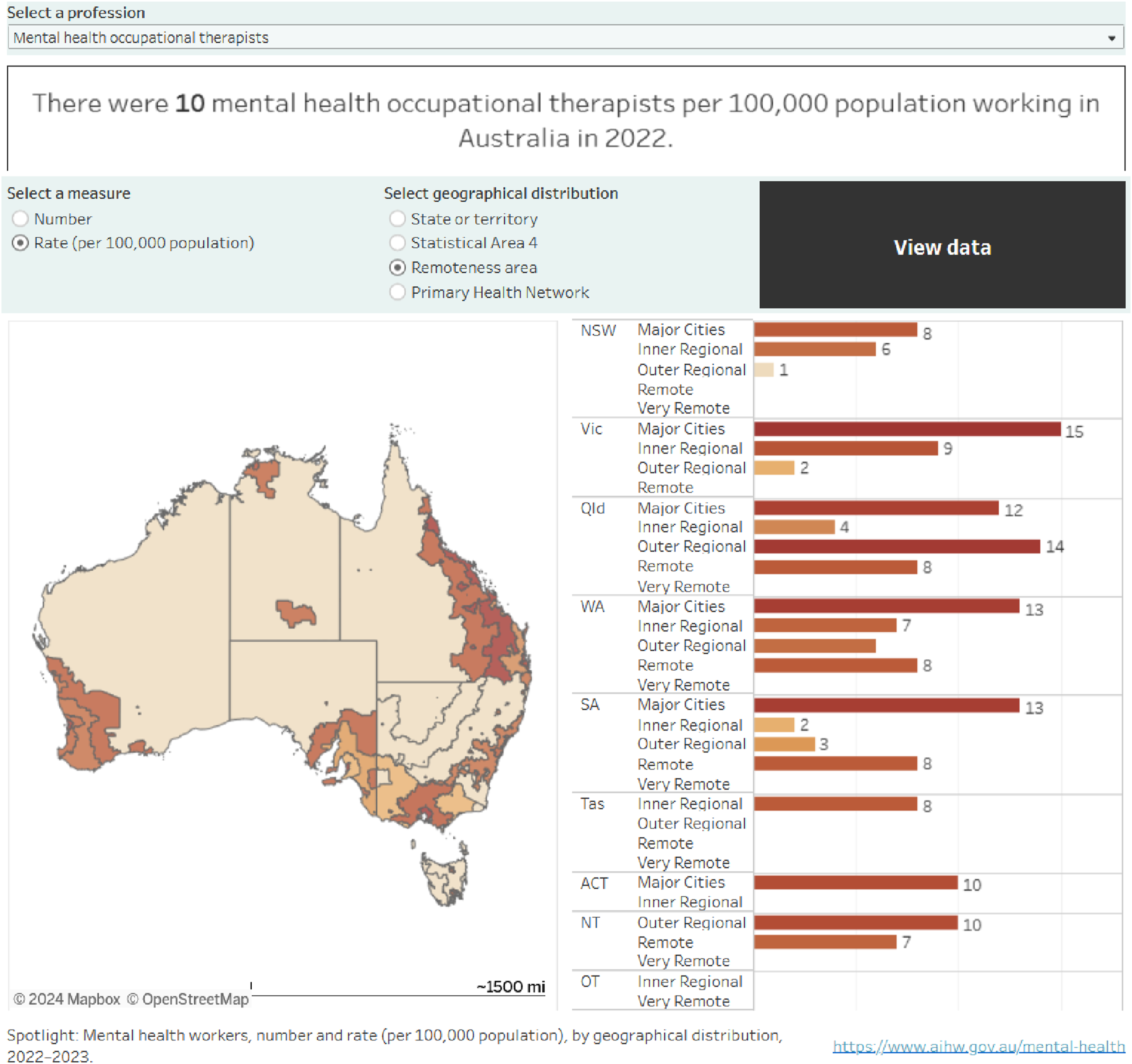
Mental health occupational therapist geographical distribution per 100,000 (Figure 3)
Similar to psychologists, occupational therapists (OT) are fairly uniformly distributed including regional and remote areas, especially South Australia.
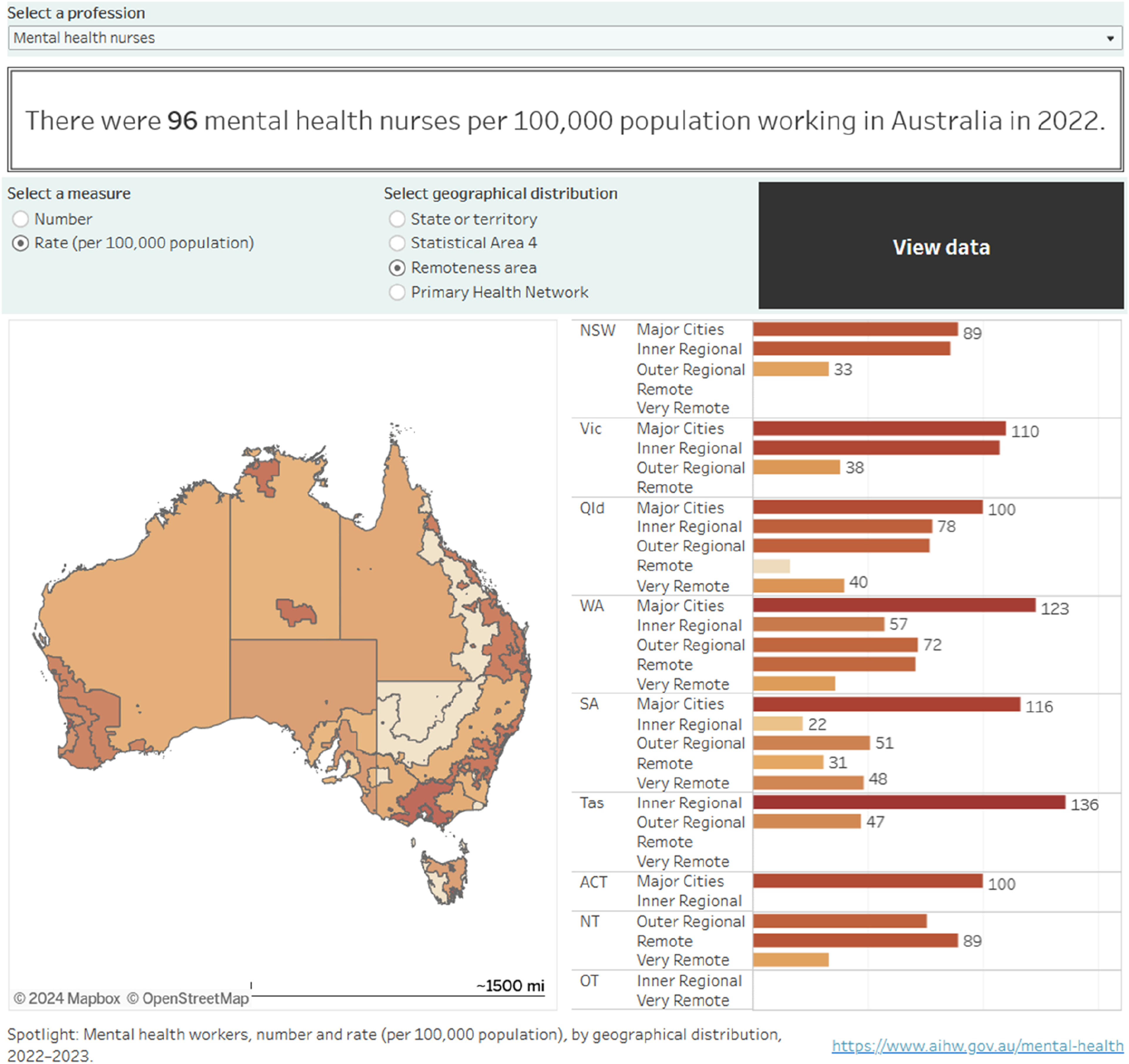
Mental health nurse geographical distribution per 100,000 (Figure 4)
Mental health nurses are possibly the most widely distributed to regional and remote areas in all States and Territories, except the ACT which is classified as a major city.
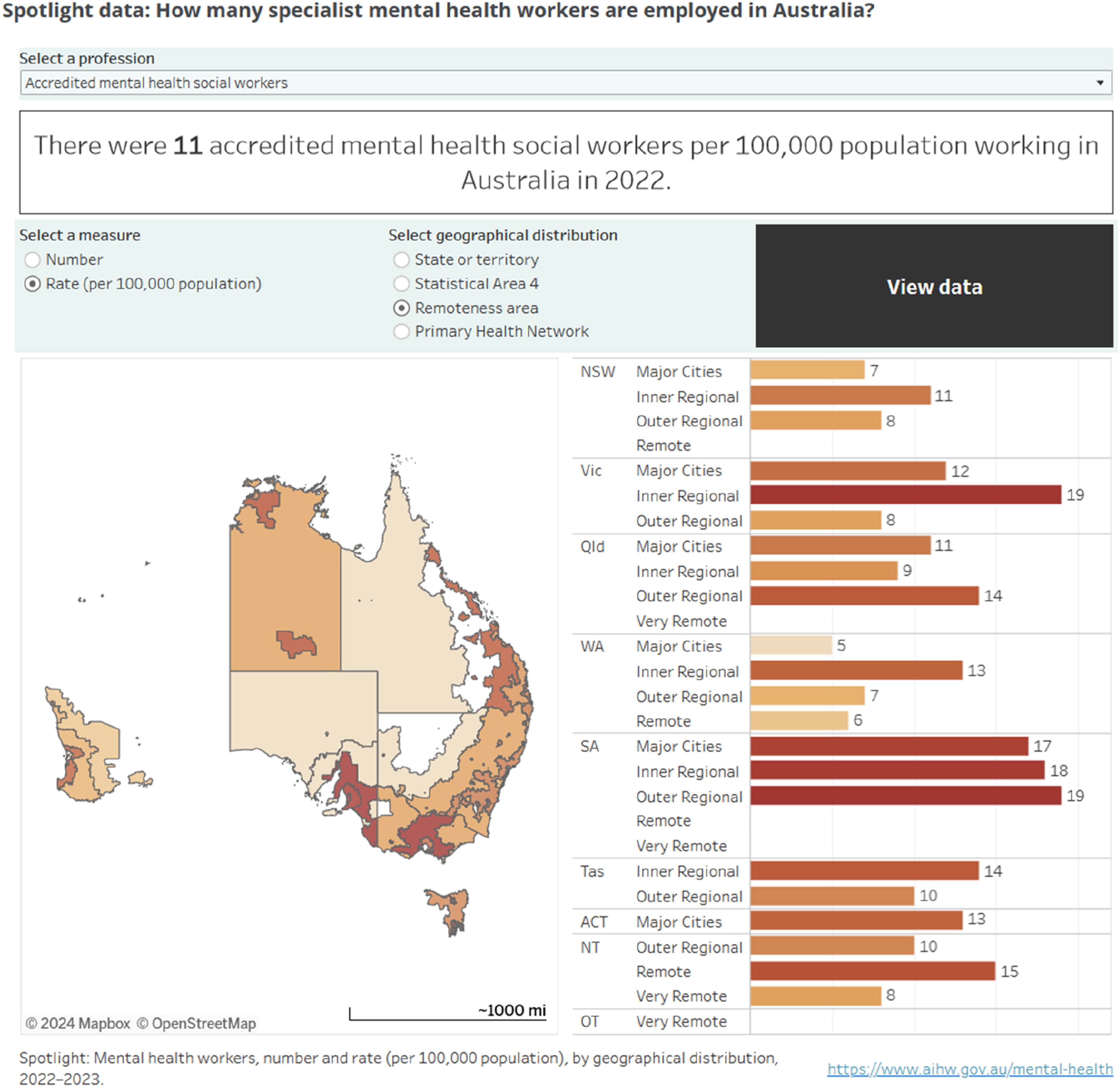
Mental health social worker geographical distribution per 100,000 (Figure 5)
More than any other mental health profession in the AIHW data, social workers are actually at higher levels in regional and remote settings compared to major cities, again with the exception of the ACT. These data are remarkable indeed, indicating that social work positions are available and are filled in regional and remote area.
Discussion
These data reveal that there is, overall, a varied and unevenly distributed specialised mental health workforce with fewer workers with increasing distance from urban centres. Psychologists and mental health nurses have the highest rates of workers per 100,000 in rural and remote areas. Mental health social workers are relatively well represented in regional and remote areas compared to urban areas. There are few rural psychiatrists with the NT and Queensland having higher rates per 100,000 in Outer Regional and Remote areas.
At the national level, it is remarkable that the largest workforce, psychologists, at 125 per 100,000 exceed the numbers of nurses at 96 per 100,000 of population. Potentially, psychologists, nurses, and all specialised mental health workers work across private and public sectors. The AIHW data do not indicate the relative proportions of public, private and non-governmental sector employment, and we recommend that further research using the National Health Workforce Dataset may be useful to determine these specific sectoral employment distributions.
It is also notable that the majority of the professions, psychologists, mental health nurses, mental health occupational therapists, and especially mental health social workers are to some degree present in regional and remote areas. However, more detailed analysis at the more granular local governmental area levels in 2018 revealed there was significant spatial inequality of regional and remote mental health nurse staffing. 7 Consequently, further research might explore, for each specialised mental health profession the granular distribution of professionals available in the National Health Workforce Dataset, as was conducted for mental health nurses in relation to classified local governmental areas, in 2018. 7 This would reveal if there are specific shortages within smaller areas, across the states and territories. There are also regionally based psychiatrists in the majority of states, though less in very remote areas, with the exception of South Australia and the ACT (which is classified as a major city). A recent report regarding rural mental health services in South Australia highlighted the psychiatrist, nursing and allied health workforce deficits, and commented further on structural challenges with staffing. 8
Also worth exploring are longer term trends in workforce, such as that recently conducted for psychiatrists, which found that overseas trained psychiatrists comprised the majority of the meagre workforce in regional and remote areas. 2
Though there are data on the distribution of specialised mental health workers, there is unfortunately a lack of estimates of the required levels of regional and remote staff. It would also be relevant to compare if mental health workforce maldistribution is comparable with broader health workforce distribution.
There are also the recent expansions of models of telehealth for mental healthcare, and which in psychiatry greatly expanded from a relative low base prior to the COVID-19 pandemic, for psychiatrist 9 and allied health mental health consultations. 10
The National Mental Health Workforce Strategy released in 2022 has identified as part of Strategic Pillar 2 to ‘Address workforce supply in rural and remote areas, and, Address workforce distribution across settings and between public, private and not-for-profit sectors’. 11 The strategic approach to increase regional and remote placements, provide supervision, ensure local training pathways and encourage locals to stay and train, and enhance retention are all reasonable, 11 but depend upon the existing workforce which may be challenging, 12 due to long lead-in times for specialised mental health worker training. There have been initiatives by the RANZCP to expand psychiatrist training in rural mental health, 13 which have been implemented in Western Australia in 2022, since the National Mental Health Workforce Strategy. 14 With the current distribution of specialised mental health workers, such as psychiatrists’ and psychologists’ supervision and training may need to be provided remotely via telehealth, at least in part, as historically the pioneering use of telehealth in Australia was in rural and remote regions. 9 To date, there has been positive feedback and outcomes from rural telepsychiatry referrers suggest it is convenient and enhances communication, with some reservations that rural workers may be de-skilled. 9 More will need to be known about what can be done to enhance retention, as there is evidence of increased workload and stress due to lower worker numbers, and less known particularly of retention factors including professional, personal or community reasons. 15 A recent systematic review of strategic approaches to general health and social care workforce planning found that, unfortunately there are very limited data on allied health professionals in general (one reference on average), whilst the majority of research was on the medical and nursing workforce. 16
While we have comparative maps of specialised mental health worker distribution in regional and remote Australia, there are limits to interpretation without estimated workforce numbers for the majority of professions, excepting psychiatric 2 and mental health nursing 7 workforce data, which show demonstrable shortages in more granular data analyses. This granular data, and trends over time, together with infrastructure (hospital and community mental health facilities) and outcomes are needed to gain a more comprehensive picture of specialised remote and regional mental healthcare, and the role of workforce levels for each of the professions.
Footnotes
Author contributions
All authors have satisfied: Substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work; AND Drafting the work or revising it critically for important intellectual content; AND Final approval of the version to be published; AND Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JCLL, SA, TB, and SK are on the editorial team of the journal and were not involved in the editorial handling of the paper. This paper is independently peer-reviewed. This paper reflects the views of the authors, not the journal.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.