
Abstract
Objective
In this perspective, we investigate how the Royal Australian and New Zealand College of Psychiatrists’ (RANZCP) position statement on psychotherapy takes the potential for adverse effects into account.
Conclusions
Psychotherapy has two critical outcomes – efficacy and adverse effects. Evidence-based psychotherapy is significantly more effective than care-as-usual for about one in 10 psychotherapy patients. However, a similar proportion also reports adverse effects. Despite this, the RANZCP position statement on psychotherapy focuses on efficacy with minimal discussion of the adverse effects. This is an oversight because psychiatrists have legal and ethical obligations to consider the adverse effects as well as the benefits of any treatment. We therefore reflect on the RANZCP’s six recommendations in light of the adverse effects of psychotherapy.
‘Facing it, always facing it, that’s the way to get through. Face it.’ - Captain McWhirr, Typhoon, by Joseph Conrad
Psychotherapy is central to psychiatry. The most recent position statement on psychotherapy was released by the Royal Australian and New Zealand College of Psychiatrists (RANZCP) in 2021. 1 The question that led to this perspective was ‘How does this statement take into account the adverse effects of psychotherapy (hereinafter PAEs) when making recommendations on psychotherapy?’
We found that the RANZCP position statement focuses on the well-established benefits of psychotherapy with minimal comment on the potential adverse effects. However, ‘non nocere’ (do no harm) is one of the most important ethical rules in psychiatry. Psychotherapeutic conversations can and do have adverse effects. ‘For most patients, it can be burdensome to speak about insufficiencies of oneself, to be confronted with painful memories, to be exposed to threatening situations, or to be subject to treatment demands’. 2 Psychiatrists are obliged to inform patients about these potential harms when gaining consent for therapy. 2
We therefore provide a perspective that aims to advance the recognition of PAEs and their implications for RANZCP psychotherapy training, clinical practice, and research. Our perspective is structured to: (1) define PAEs, (2) summarise the qualitative and quantitative studies of PAEs, and (3) provide evidence-based reflections on the six RANZCP recommendations on psychotherapy in light of recent reviews of PAEs (Box 1).3–5
Defining the adverse effects of psychotherapy
The World Health Organization (WHO) defines the term ‘adverse effects’ as the subjectively unpleasant consequences of any treatment that were not the intended goal.6,7 Adverse effects vary in the degree of physical, psychological or social suffering, and associated impairment in functioning, and are measured on a continuum. 6 Harm is determined by the severity and duration of adverse effects and any resulting treatment implications. 6
We therefore used these concepts as reported by the patient or observed by close family members and/or the treating therapist to correctly applied evidence-based psychotherapy such as psychodynamic therapy or cognitive behavioural therapy (CBT). Since the outcomes of psychotherapy are inherently subjective (e.g. improved or worsened mood), patient reports of PAEs are the most important measure although close family members, friends, colleagues, and the therapist may be affected by changes in the patient. Other than the particular type of psychotherapy offered, PAEs are related to the therapeutic skills of the therapist, the quality of the two-person therapeutic relationship, and the patient’s presentation or personality. 8 PAE rates are probably higher in the real world than in clinical trials with manualised treatments and close supervision because of varying levels of therapist skills, training, and adherence to therapy principles.
Qualitative and quantitative studies of adverse effects
Patient lived experience informs descriptions of PAEs, given they have unique knowledge about their own life journey and what constitutes recovery.
9
Psychotherapy requires epistemic trust that the therapist’s knowledge is credible and applicable to the patient’s life. Consequently, negative experiences are associated with epistemic vigilance or mistrust of the therapist’s competence or benevolence.3,9 Qualitative studies indicate that patients often attribute negative experiences to therapist misbehaviour or poor treatment fit.
3
These, in turn, are associated with the following: • Increased problems after therapy • Fear of the therapy process • Loss of motivation or hope • Unpleasant feelings during therapy • Negative cognitions aroused in therapy.
3
Dynamic formulations of PAEs have a similar focus on the therapeutic relationship where a patient forms a dependent transference relationship with their therapist, thereby incurring a loss of agency and capacity to independently problem-solve and regulate their emotions, leading to worsening symptoms. 10 In some longer-term therapies, there is the potential for regression, greater self-absorption, and adoption of the sick role with the risk of further PAEs during the termination of treatment. 10 PAEs are considerably less likely when therapy is viewed as a shared endeavour with patients and therapists undertaking a collaborative journey that results in enhanced patient self-agency. 9
PAEs are one of the two critical outcomes in randomised controlled trials (RCTs) of psychotherapy.3,4 The first critical outcome is measuring whether therapy works (efficacy or effectiveness), and the second critical outcome is tolerability, that is, whether a patient can withstand any PAEs so therapy has a meaningful impact. 11 As with any psychiatric treatment, the benefits of psychotherapy should outweigh the adverse effects. Current RCT-level evidence demonstrates that evidence-based psychotherapy is effective for about one in 10 psychotherapy patients compared to care-as-usual controls, while RCT reports also indicate that a similar proportion experience PAEs in making these significant gains.4,12
All RCTs of psychotherapy should therefore measure clinically significant improvement and PAEs in the same detail in both intervention and control groups.4,5 In particular, comprehensive patient interviews with independent assessors provide more in-depth descriptions of PAEs. 7 To meet the independence criterion, PAE assessors should be unaffiliated with the clinical trial and not biased for or against the particular type of psychotherapy. 7
As with the adverse effects of medication, patients may experience unpleasant consequences of psychotherapy even if their overall clinical state improves.
2
PAE rating scales measure patient and observer reported harm.
13
Over 1 in 10 patients or therapists have reported PAEs in the following domains: • Increased problem complexity • Therapy dependency • Therapy burdensome • Symptom deterioration • New symptoms • Stigmatisation.
14
Evidence-based reflections on the six RANZCP recommendations
Recommendation 1. Psychotherapy must be embedded in training for all psychiatrists
We reflect on the RANZCP’s recommendations on psychotherapy, in light of recent reviews of qualitative and quantitative evidence on PAEs.3–5 The first recommendation is that ‘Psychotherapy, as a key component of every psychiatric treatment, must be embedded in training for all psychiatrists’ (Box 1). 1
RANZCP recommendations on psychotherapy
RANZCP. Psychotherapy conducted by psychiatrists. Position statement #54. Melbourne, Australia: Royal Australian and New Zealand College of Psychiatrists, 2021.
Recommendation 2. Further study in psychotherapy should be supported
Indicators of possible psychotherapy adverse effects
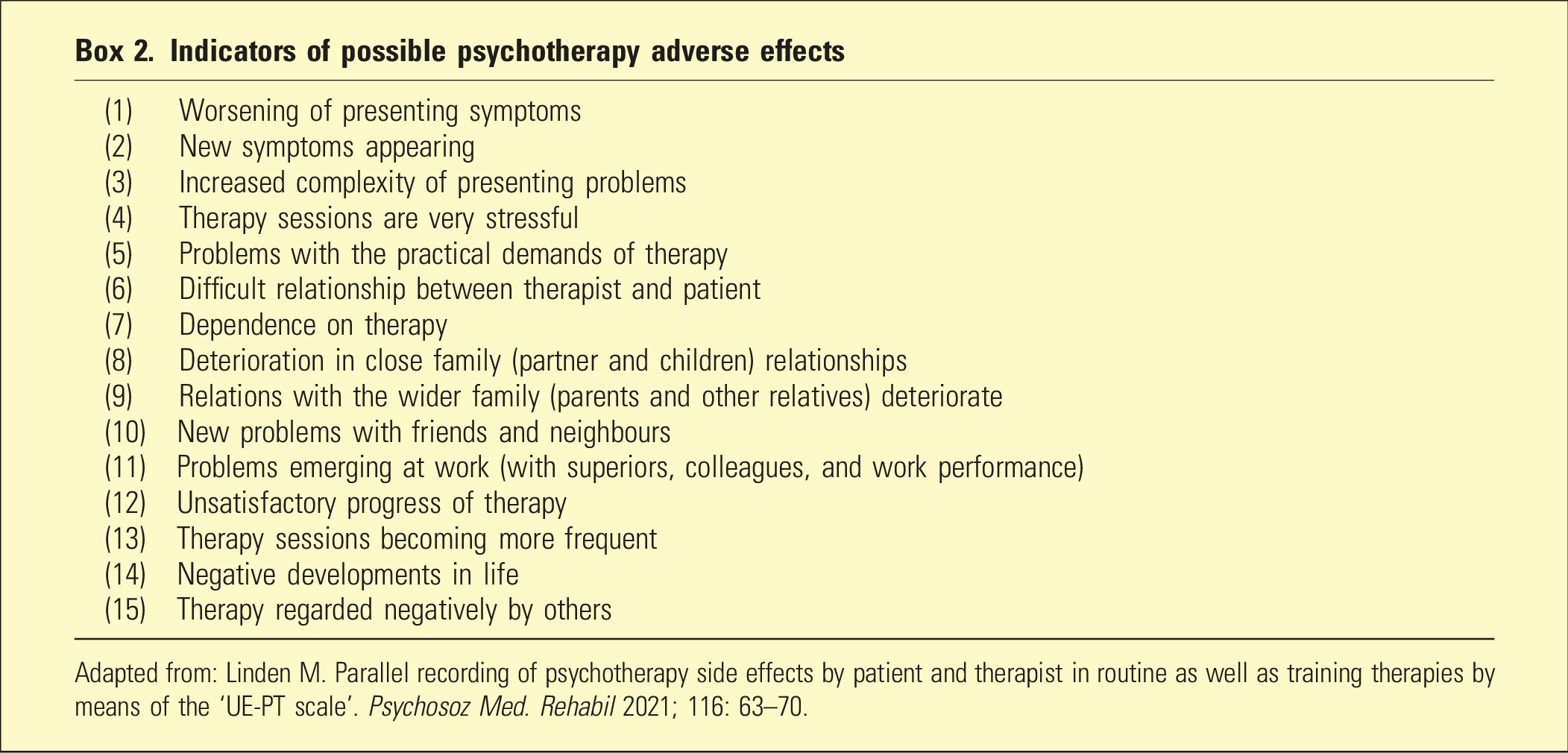
Adapted from: Linden M. Parallel recording of psychotherapy side effects by patient and therapist in routine as well as training therapies by means of the ‘UE-PT scale’. Psychosoz Med. Rehabil 2021; 116: 63–70.
Recommendation 3. Psychotherapy should be widely available to the population
Although the RANZCP recommends that psychotherapy should be widely available in public and private practice for patients with a variety of mental conditions, this may have negative as well as positive effects. For instance, a large survey of psychotherapy patients found one in 20 reported persistent PAEs, while another reported that 14% of patients experienced persistent PAEs after psychotherapy for depression or anxiety.15,16
Programmes to expand access to psychotherapy should therefore take these risks into account. This might include measuring and publishing patient and therapist ratings of PAEs and whether clinical deterioration is attributed to psychotherapy or other factors. Patients need information about their chances of improving or deteriorating after psychotherapy, based on these data.
Recommendation 4. Psychiatrists providing a balance of psychotherapy and medication
The RANZCP highlights that psychiatrists are trained in the use of psychotherapy and pharmacotherapy, which ensures that their patients are provided with the right balance of treatment. Adding psychotherapy to medication may improve treatment outcomes for patients with severe psychiatric conditions.1,12 For example, combined psychotherapy and antidepressants are recommended as the treatment for severe depression, based on clinical and cost-effectiveness. 17
In addition to maximising the benefits of combined treatment for severe depression, psychiatrists are also able to minimise the combined adverse effects of psychotherapy and antidepressants. The biological adverse effects of antidepressants include weight gain, sedation, and effects on sexual function, while PAEs include increased problem complexity and symptom aggravation due to psychotherapy.3,4,17 Patients receiving combination treatment for severe depression can experience various interactive combinations of these adverse effects, for example, increased problem complexity and sexual dysfunction. Psychiatrists should detect these psychotherapy and pharmacotherapy adverse effects and adjust treatment to alleviate them.
Recommendation 5. Psychotherapy providing unique benefits
The RANZCP notes that psychotherapy provides benefits that other treatment modalities cannot. For example, the treatment of choice for severe personality disorder is psychotherapy, because pharmacotherapy is not effective for the core features. 18 There is a signal that psychotherapy reduces the risks of self-harm and suicide-related behaviour associated with severe personality disorder. 18 However, research into PAEs has been neglected in this population, and future trials should therefore compare intervention groups with care-as-usual controls on relevant measures such as difficulties in the therapeutic relationship and reawakened traumatic memories. The expectation is that psychotherapy would be superior to care-as-usual on PAEs, but this benefit needs to be quantified.
Recommendation 6. The need for continuing research into psychotherapy
Finally, the RANZCP recommends further empirical research into the efficacy, cost-effectiveness, and PAEs of specific types of psychotherapy for different conditions. Given the gaps in the evidence that we have identified on the PAEs associated with popular psychotherapies such as psychodynamic therapy and CBT, clinical trials of these psychotherapies should systematically measure PAEs as well as efficacy and cost-effectiveness. 5 Further empirical research is also needed on optimising the process of informed consent and shared decision-making by discussing PAEs. 19
Strengths and limitations
The major weakness of this Perspective is the limited available information on PAEs on which to base our conclusions. However, a strength is that it also provides the first preliminary discussion of the RANZCP recommendations on psychotherapy in light of the available qualitative and quantitative evidence on PAEs.3–5 Psychiatrists have legal and ethical obligations to consider the adverse effects of any treatment and inform their patients accordingly. 2 Greater recognition of the potential for PAEs could therefore contribute to RANZCP psychotherapy training, clinical practice and research. Minimising PAEs though early recognition is a possible means of improving patient outcomes from psychotherapy above the current ceiling for treatment efficacy. 12 It is also foundational to the ethical practice of psychotherapy. 2
Footnotes
Authorship
All authors have satisfied: Substantial contributions to the conception or design of the work; the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that SA, JCLL, SK, and TB are editorial team members for this journal – they were not involved in the independent editorial or peer review processes. TB has received Honoraria from CSL Sequirus for a lecture.