
Abstract
Objective
The Medicare Benefit Schedule (MBS) telehealth items were expanded in March 2020 during the COVID-19 pandemic. We measured the use of MBS telepsychiatry items compared to consultant physician telehealth items within the context of these item changes, to understand differences in telepsychiatry and physician telehealth utilisation.
Methods
Monthly counts of face-to-face and telehealth (videoconferencing and telephone) MBS items for psychiatrists and physicians from January 2017 to December 2022 were compiled from Services Australia MBS Item Reports. Usage levels were compared before and after telehealth item expansion. Usage trends for MBS telepsychiatry and physician telehealth items were compared in time-series plots.
Results
Telehealth item expansion resulted in a greater rise of telepsychiatry services from 3.8% beforehand to 43.8% of total services subsequently, compared with physician telehealth services (from 0.6% to 20.0%). More physician telehealth services were by telephone compared with telepsychiatry services. Time-series of both telehealth services displayed similar patterns until mid-2022, when physician telehealth services declined as telephone items were restricted. Telepsychiatry services consistently comprised a greater proportion of total services than physician telehealth services.
Conclusions
MBS psychiatrist services showed a more substantial and persistent shift to telehealth than physician services, suggesting a greater preference and use of telepsychiatry.
Introduction
The COVID-19 pandemic prompted heightened demand and use of telehealth globally, which helped to ensure continuity of care for patients with various medical conditions. 1 In the context of COVID-19-related stringency measures the Australian Medicare Benefits Schedule (MBS) telehealth items, for reimbursement of private medical consultations, were expanded from 13 March 2020 onward. 2 New temporary telehealth items were made available for various specialist services, including general practitioners (GPs), consultant physicians, psychiatrists, paediatricians, geriatricians, public health physicians, neurosurgeons, anaesthetists and allied healthcare providers. Complementary videoconferencing and telephone items were created for many existing face-to-face MBS items.3–5
In January 2022, another MBS policy change to the availability of telehealth items was implemented. Most MBS telehealth items by videoconferencing and some telephone items (One out of five consultant physician items and three out of 17 psychiatrist items) were made permanent. Other telephone items were retained temporarily but subsequently removed on 30 June 2022. 6
Telehealth items benefited many patients in accessing care, especially in the context of lockdowns and social distancing with a substantial growth in telehealth use as a substitute for face-to-face consultations.7–9 As the COVID-19 pandemic evolved, Australian movement restrictions eased and MBS telehealth item availability was revised downwards, particularly for telephone consultations, including GPs. 10 However, longer-term impacts, including for telepsychiatry, are currently unknown.
Telepsychiatry may be useful beyond the pandemic, especially in hybrid models of care that combine in-person and online consultations. 11 Consequently, many psychiatrists consider that most of their patients are suitable for hybrid care telepsychiatry. 12 Psychiatric treatments are often provided in a shared-care model with GPs who act as care coordinators and conduct physical check-ups and monitoring. 13 A greater and more sustained shift to telehealth might therefore be possible in psychiatry compared with other medical specialities that require regular physical interactions (examination and investigations), for which telehealth is unsuitable. Accordingly, another medical discipline (consultant physicians) that has experienced similar changes (telehealth item expansion in the context of COVID-related movement restrictions) may serve as a comparator for the study of telepsychiatry usage trend patterns. In considering the comparator group for our study, we thought it appropriate to view psychiatry as more analogous to the broad category of general internal medicine or the combined physician sub-specialities. 14 Therefore, we sought to compare telepsychiatry services with another type of non-mental health medical telehealth services catering to the general patient population. Consequently, we chose the MBS item group for consultant physicians as a comparator, instead of other healthcare professionals such as GPs, allied mental health professionals or surgeons.
In this study, we compared the use of consultant psychiatrist and physician MBS telehealth items (telephone and videoconferencing) from March 2017 to February 2023 to understand relative trends in the use of MBS telepsychiatry and physician telehealth services, since the expansion of MBS telehealth items in March 2020. These findings could potentially inform future resource allocation for MBS medical and psychiatric care in Australia and beyond.
Methods
Data source
National monthly service data for MBS items for outpatient psychiatric and consultant physician services were retrieved from the Services Australia website for MBS item reports (https://medicarestatistics.humanservices.gov.au/statistics/mbs_item.jsp). The study period was from March 2017 to February 2023, with two equal 36-month periods before March 2020 and from March 2020 onward. Both face-to-face and telehealth (video and telephone) MBS items for psychiatric consultations and consultant physician consultations were included (Supplemental Table 1).
Data analysis
Data analysis was performed in Microsoft Excel. Monthly MBS item reports were combined according to modalities (face-to-face or telehealth) for both psychiatric and consultant physician items. Descriptive statistics were generated. As these data were not normally distributed, medians and interquartile ranges (rounded to the closest integers) were used to describe the data before and after telehealth item expansion (Supplemental Table 2). The monthly percentages of telehealth services for both disciplines were calculated from the monthly total services for included items. Time series of telehealth service counts and percentages were plotted for comparison between telepsychiatry and consultant physician telehealth items. To avoid double counting, the numbers of services under the co-claim items for telehealth (Items 112, 288 and 294) were deducted from the face-to-face service total numbers (See Supplementary Material: Appendix).
Results
Descriptive statistics
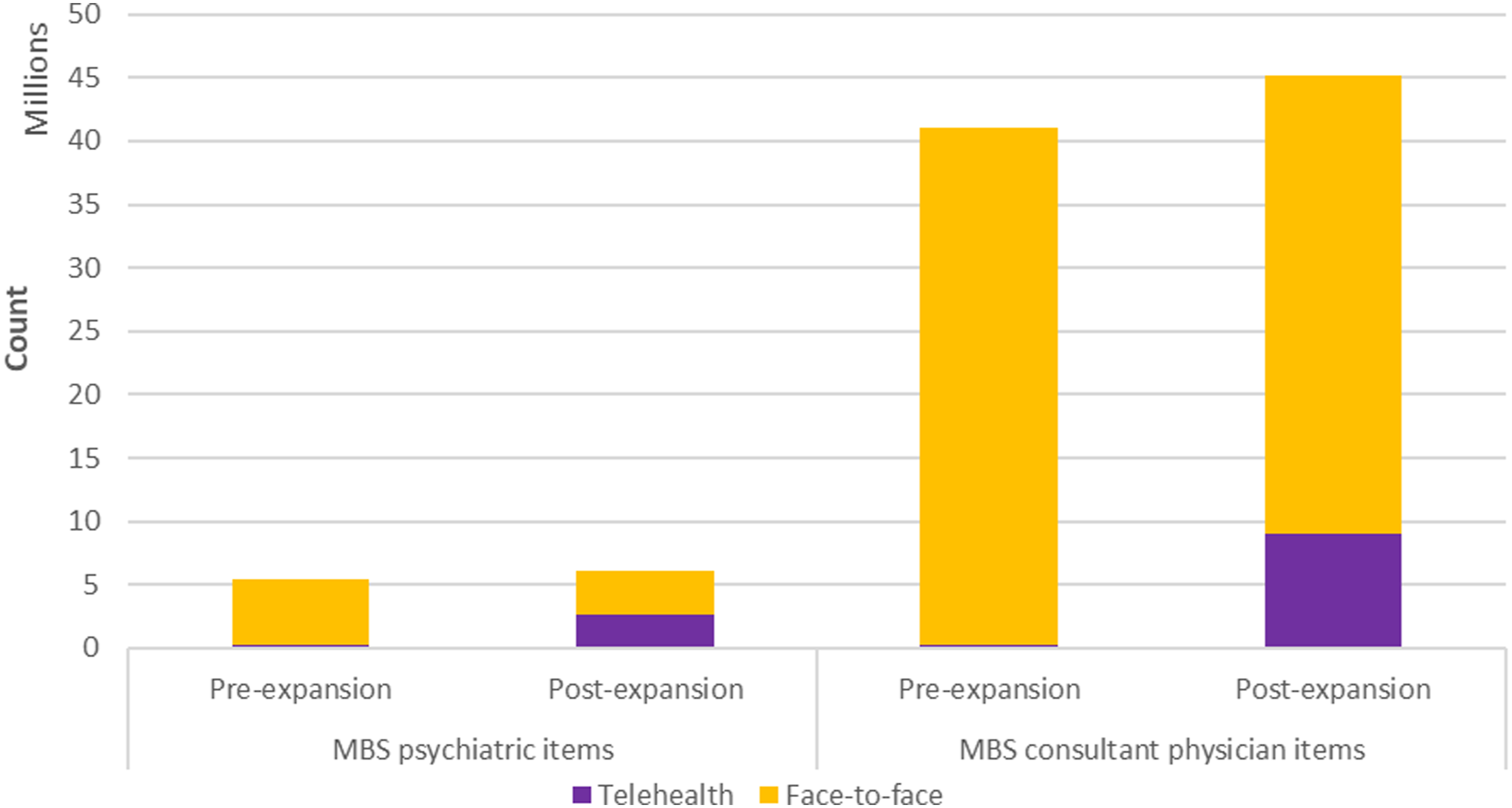
The distributions of monthly MBS consultant physician consultations and MBS psychiatric consultations before and after telehealth expansion are represented in Figure 1. The total number of services during the study period was 86,255,020 for MBS consultant physician items and 11,435,449 for psychiatrist items (Figure 2). Before the MBS item expansion, telehealth services formed a very small portion of the total services for consultations in both disciplines. After the expansion, there was a greater rise in the use of telepsychiatry services ex-ante from 3.8% of total services to 43.8% ex-post than in consultant physician telehealth services (from 0.6% to 20.0%). In the post-item-expansion period, telephone consultations constituted a higher portion of consultant physician telehealth services (74.0%) than telepsychiatry services (46.0%). Box plots for (A) Monthly MBS psychiatrist services and (B) Monthly MBS consultant physician services from January 2017 to December 2022. The box represents interquartile range and the centre line show the median. The whiskers indicate variability outside the upper and lower quartiles, and the points represent outliers. MBS psychiatrist and consultant physician items according to delivery modalities before and after telehealth item expansion (2017-2022).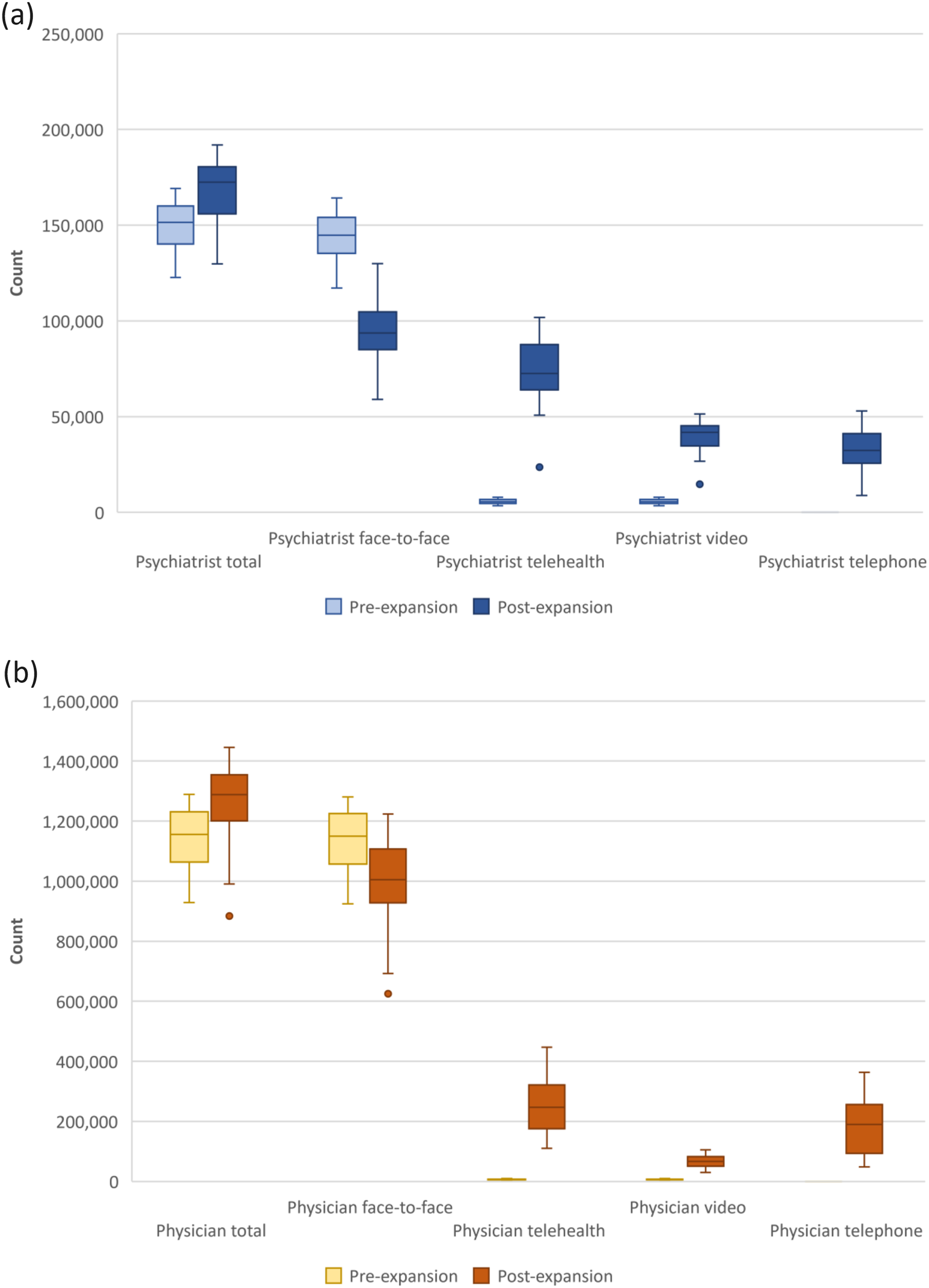
Trends of MBS psychiatrist items
Most psychiatrist services were conducted face-to-face before March 2020 (Figure 3). After that, face-to-face consultations dropped considerably with a corresponding rise in telehealth consultations. Telephone and video consultations began to diverge in January 2022. Total consultation counts showed a gradual upward trend. Monthly MBS psychiatrist services from January 2017 to December 2022.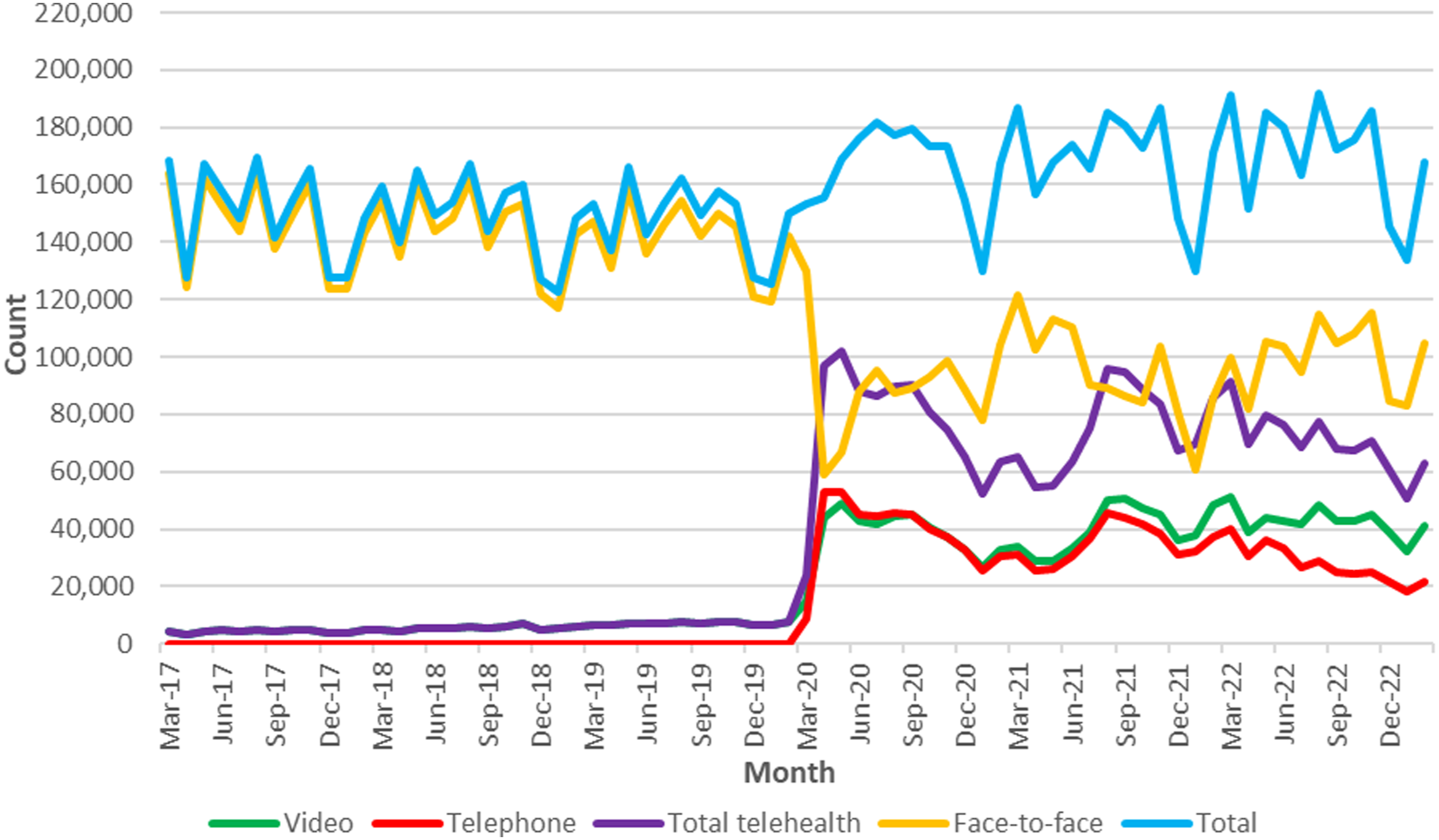
Trends of MBS consultant physician items
Most services were delivered face-to-face until March 2020 (Figure 4). Total services continued to rise per annum, but face-to-face services dipped, before returning to pre-pandemic levels by late 2022. Telehealth services increased sharply in March 2020, with subsequent large fluctuations and a gradual downward trend. Monthly MBS consultant physician services from January 2017 to December 2022.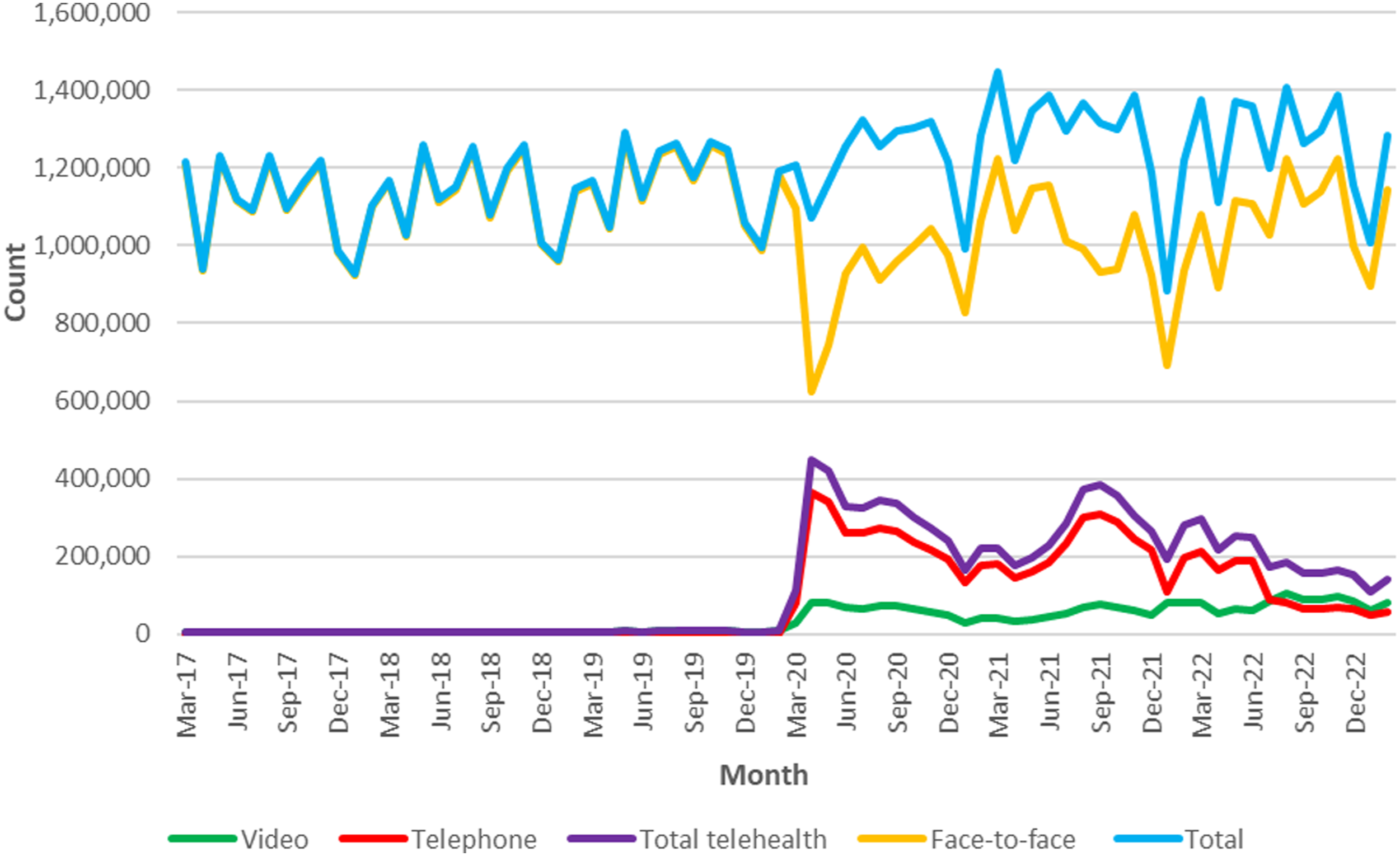
Comparison with the trend of MBS telepsychiatry items
Consultant physician telehealth services and telepsychiatry services were roughly equal in numbers before March 2020 (Figure 5(a)) but as a component of total consultations, consultant physician telehealth services formed a much smaller proportion than telepsychiatry services (Consultant physicians: 0.6% vs Psychiatrists 3.8%). From March 2020 onward, consultant physician telehealth services greatly exceeded telepsychiatry services but remained a smaller proportion of total consultations (Consultant physicians: 20.0% vs Psychiatrists: 43.8%). (a) Monthly MBS consultant physician telehealth and telepsychiatry services; (b) Monthly MBS consultant physician telehealth and telepsychiatry services plotted on separate y-axes.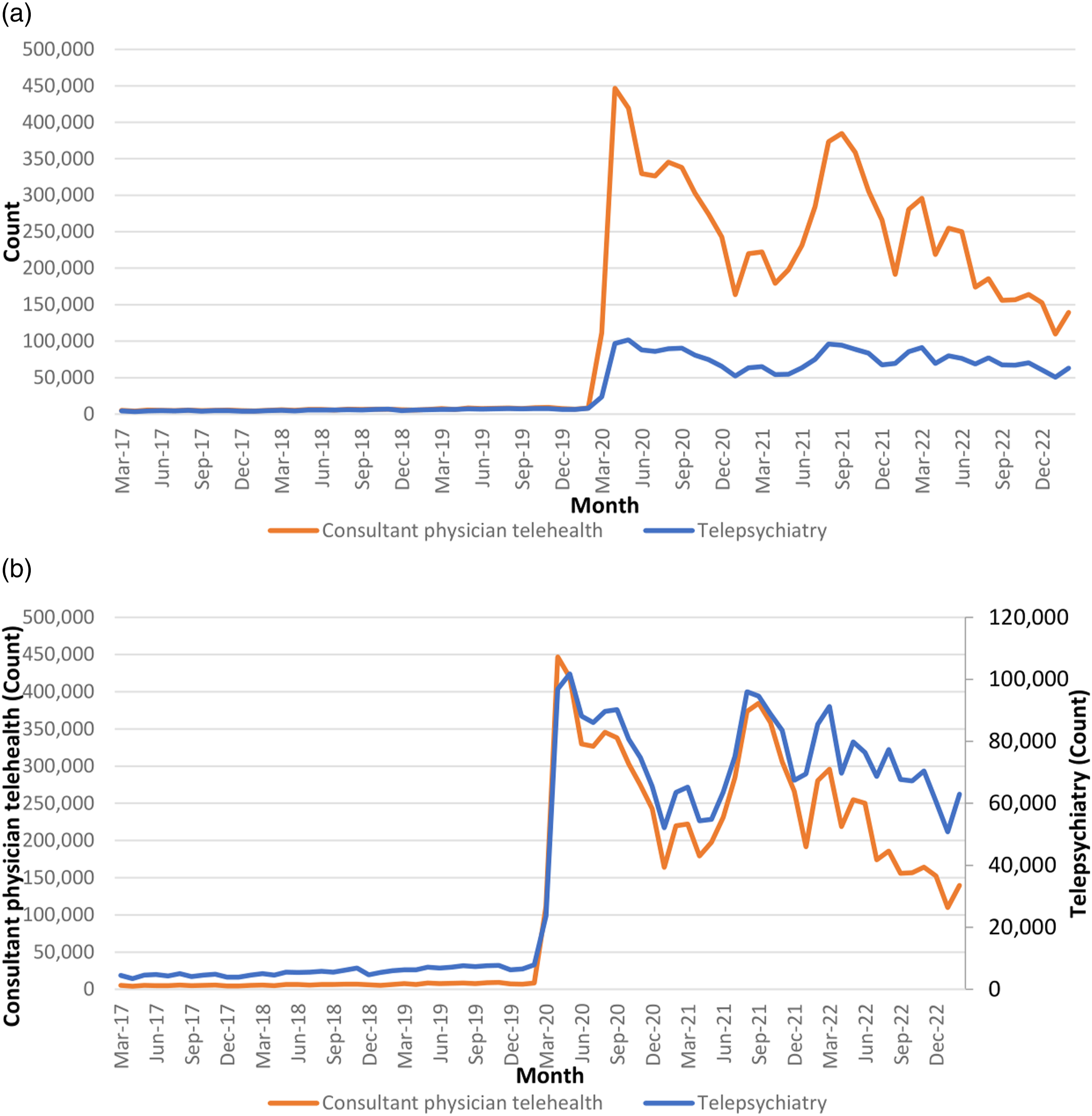
However, when plotted using appropriately adjusted scales with separate y-axes for physicians and psychiatrists, the time-series temporal trend patterns are similar until the first half of 2022, when they start to diverge (Figure 5(b)). From this point, there was a clearer downward trend in consultant physician telehealth consultations than in telepsychiatry consultations. This coincided with the announcement and subsequent full implementation of reduced availability of telephone items.
Regarding the proportion of total face-to-face and telehealth (telephone and videoconferencing) services, telepsychiatry services were slightly higher than consultant physician telehealth services throughout the pre-pandemic period (Figure 6(a)). Both categories showed rapid upward surges in March 2020, but the increase was more marked for telepsychiatry. Subsequently, telepsychiatry services consistently formed a higher percentage of total (face-to-face and telehealth) services compared with consultant physician services. Telepsychiatry services did not show as much decline from early 2022 onward as consultant physician telehealth services. (a) Monthly percentage of MBS consultant physician telehealth and telepsychiatry services; (b) Difference in telehealth as a percentage of monthly total services (Telepsychiatry minus consultant physician telehealth).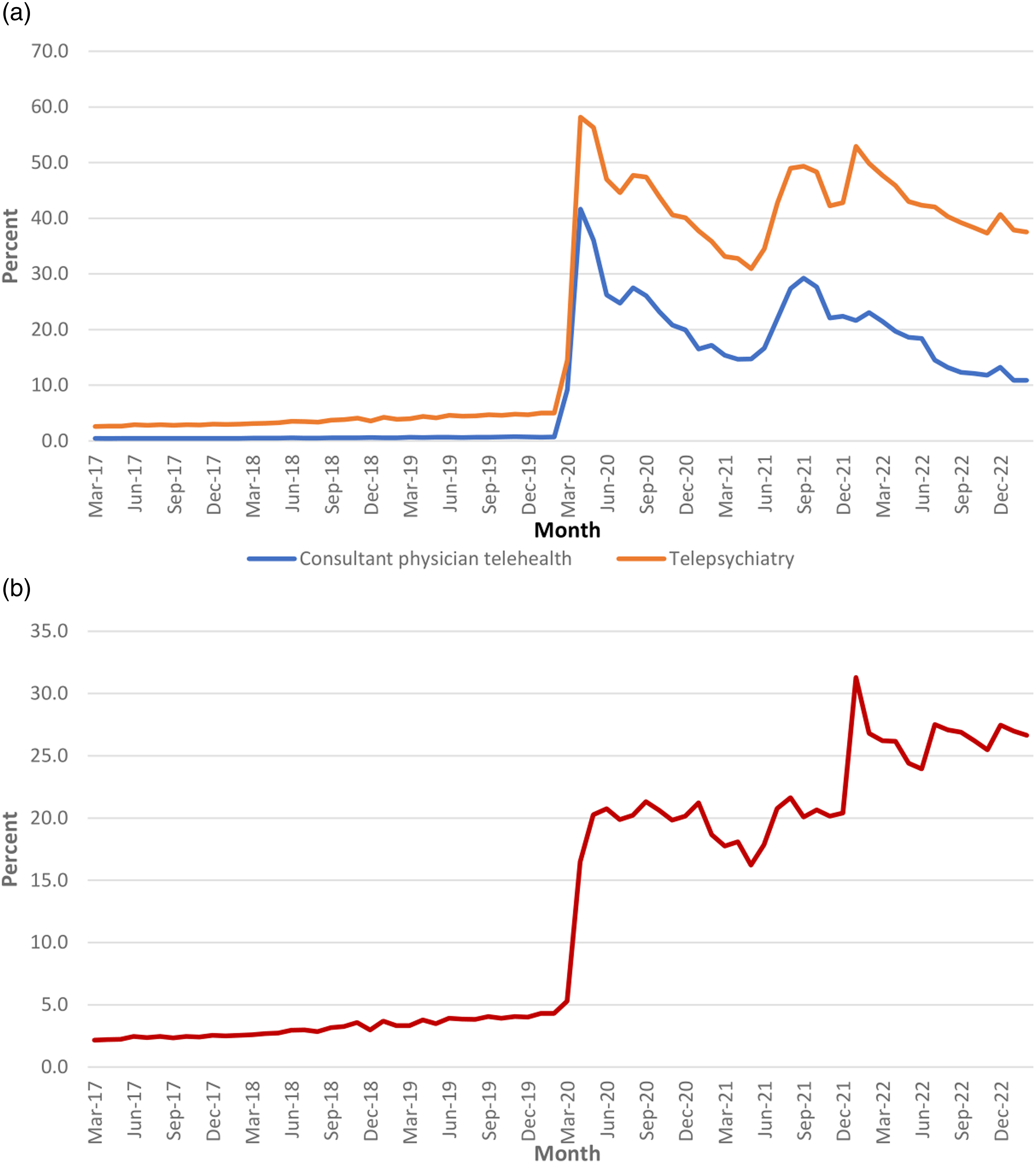
Moreover, the relative growth of telepsychiatry services as a proportion of its service category outpaced consultant physician telehealth services as a proportion of consultant physician services, as the differences in percentages of telepsychiatry services and consultant physician telehealth services steadily widened throughout the period (Figure 6(b)).
Discussion
We compared the use of consultant psychiatrist and physician telehealth items before and after the MBS expansion. Telehealth services in both specialities rose considerably with the policy change in March 2020. Total service counts for consultant physician items were much higher than for psychiatrist items, likely as a result of a greater potential pool of consultants and trainees (approximately 30,000 physicians and trainees vs 3,679 psychiatrists and trainees).15,16 While telepsychiatry services were dwarfed by consultant physician telehealth services in absolute numbers, the temporal usage patterns for these services were very similar for most of the study period. This suggests that the usage of these services varied similarly within the context of Medicare policy changes implemented in the context of COVID-19-related stringency measures, allowing for a valid comparison.
Despite these similarities, there are three major differences in the usage trends. First, after telehealth item expansion, three-quarters of consultant physician telehealth services were by telephone, whereas over half of telepsychiatry services were by videoconferencing. Second, and in this context, the decline in total telepsychiatry services was less conspicuous compared with consultant physician telehealth services when telephone item availability was reduced in June 2022. Lastly, there was a bigger initial increase and consistently higher proportions of telepsychiatry services, and these differences with consultant physician telehealth widened over time. There was a more pronounced and sustained shift to telehealth for outpatient psychiatric services compared with consultant physician services. Additionally, greater proportions of patients continued to access telepsychiatry compared with consultant physician telehealth in 2022, when COVID-19-related stringency measures and telephone telehealth item availability were reduced. Given the high levels of telepsychiatry usage, more in-depth analyses to understand why this occurred and its impact are needed. Future research in this area may include evaluating clinicians’ and patients’ perspectives on the routine use of telepsychiatry, developing models to better explain the uptake of telepsychiatry that could account for the effects of the pandemic, analyses of telepsychiatry at regional levels, as well as assessments of telepsychiatry’s impact on access to psychiatric care and access equity.
The number of total telepsychiatry services was less affected by the Medicare policy change on telephone items than consultant physician telehealth services because telephone consultations formed a smaller portion of telepsychiatry services. The proportion of video consultations is also higher for psychiatrists compared with other specialists and GPs.7,17 There is no empirical data to explain this difference. In a separate cost-analysis paper on MBS telepsychiatry services, we found that telephone consultations incur the lowest out-of-pocket costs, followed by face-to-face and video consultations having successively higher out-of-pocket costs. 18 A lower proportion of the video consultations were bulk billed than for the other consultation types. Accordingly, cost considerations should prompt telephone use, instead of videoconferencing, but clinical factors might have encouraged the choice of consultation by videoconferencing. While telephone consultation is less technically demanding and more convenient for patients, 19 there are diagnostic challenges and potential difficulty in establishing a therapeutic alliance due to the lack of visual cues. 20 Videoconferencing, while not always the first choice, is probably still preferred by many patients for psychiatric consultations.
The sustained use of video consultations can be seen as the manifestation of telepsychiatry as an ‘experience good’ from the economic perspective.21,22 In contrast to a ‘search good’, whose qualities can be determined by the consumer before purchase through an information search, an ‘experience good’ is one whose qualities cannot be determined before purchase but require actual experience after purchase. 23 Lack of access and reimbursement are fundamental barriers to telehealth services. 24 After the MBS telehealth expansion, many patients had the opportunity to use this type of service for the first time. This might be especially true for metropolitan patients, who were not eligible for Medicare reimbursement under the former telepsychiatry scheme reserved only for patients in rural and remote areas. 25 Similar to many other healthcare services, as an ‘experience good’, telepsychiatry can only be accurately evaluated and compared to its alternative (i.e. face-to-face consultations) after the service has been bought and experienced. 26 As shown in several Australian studies, patients and caregivers indicated a high level of acceptance and satisfaction after trying telepsychiatry, with patients reporting perceived benefits and willingness to use it again.11,27 If this is true, there will be a likely ongoing demand for telepsychiatry via videoconferencing. While the widened access to telehealth for metropolitan patients is a positive development, we note that the MBS telehealth item restructuring also involved the abolishment of the 50% fee-loading telehealth co-claim item 288 since January 2022, which particularly impacted access equity for rural patients. The later-introduced co-claim item 294 makes bulk-billing a requirement and might not be as appealing to psychiatrists as the former item 288, which instead provided an additional bulk-billing incentive payment. The 294 policy change reduces more affordable telehealth for patients in rural and remote areas and may further exacerbate health inequity experienced by this disadvantaged population as they face increased competing metropolitan demand for telehealth resources. 28
Consultant physician telehealth services consisted mostly of telephone consultations. Consequently, there was a more obvious decline in overall services compared to telepsychiatry after the specific telephone item policy change. This suggests that the substitution of videoconferencing for telephone consultation was not preferred by patients. A possible explanation is that resource constraints and limited technological aptitude are major determinants of patients’ choice of telehealth. 24 and are related to socioeconomic status.29,30 In a study of GP MBS telehealth services in Victoria, the proportion of telephone consultations was higher in the less socioeconomically advantaged areas compared to more socioeconomically advantaged areas. 31 Thus, reduced telephone item availability may reduce equitable access to healthcare. 32 It is also possible that the greater proportion of telephone consultations for physician telehealth consultations was due to physicians’ preference for the telephone over videoconference rather than any patient factors. This preference might be related to the comparatively less emphasis on non-verbal cues than on the content of verbal history for physician consultations compared with psychiatric consultations. Empirical research on clinicians’ preferences for telehealth options would be needed to clarify this point.
Several study limitations should be mentioned. As this study focused on Medicare-reimbursed private medical outpatient services, public-sector telehealth services and services funded by the Department of Veterans Affairs were not included. Since some medical sub-specialities may be more able to provide services through telehealth formats than others, ideally, we should have compared psychiatric consultations with physician consultations by sub-specialities. However, we were unable to do so as the same set of MBS item numbers were assigned to all sub-specialities of physician consultations. For psychiatric consultations, we did not include analysis by categories of MBS items, for instance, comparing once-off assessment items and follow-up items. Whether telehealth contributes to the growth of lucrative private practice business models, which focus on once-off diagnostic assessments, is a valid concern with considerable ethical implications and requires further scrutiny. Moreover, the MBS usage figures were based on Medicare claim data. Thus, monthly figures were determined by the date the service was processed, with a lag period from the date the service was provided and might vary due to the different number of processing days in a month. Only the number of services provided was available, not the actual number of patients receiving the services. Socioeconomic information (e.g. income levels) and clinical information (e.g. diagnostic profiles) were unavailable. Finally, we did not do a gender and age analysis to see if these factors predicted differences seen in MBS telehealth usage patterns.
The increased use of telepsychiatry services was larger and more sustained compared with consultant physician telehealth services. Telepsychiatry services might be less affected by the reduced availability of telephone items from June 2022 compared with consultant physician telehealth services. Psychiatric consultations are likely more amenable to telehealth compared to other medical consultations, and more research is needed on their long-term role in providing private psychiatric care.
Supplemental Material
Supplemental Material - Comparing the trends of MBS telepsychiatry and consultant physician telehealth services from 2017 to 2022: A retrospective study
Supplemental Material for Comparing the trends of MBS telepsychiatry and consultant physician telehealth services from 2017 to 2022: A retrospective study by Luke S-C Woon, Stephen Allison, Tarun Bastiampillai, Steve Kisely, Paul Maguire, William Pring, Rebecca Reay and Jeffrey CL Looi in Australasian Psychiatry
Supplemental Material
Supplemental Material - Comparing the trends of MBS telepsychiatry and consultant physician telehealth services from 2017 to 2022: A retrospective study
Supplemental Material for Comparing the trends of MBS telepsychiatry and consultant physician telehealth services from 2017 to 2022: A retrospective study by Luke S-C Woon, Stephen Allison, Tarun Bastiampillai, Steve Kisely, Paul Maguire, William Pring, Rebecca Reay and Jeffrey CL Looi in Australasian Psychiatry
Supplemental Material
Supplemental Material - Comparing the trends of MBS telepsychiatry and consultant physician telehealth services from 2017 to 2022: A retrospective study
Supplemental Material for Comparing the trends of MBS telepsychiatry and consultant physician telehealth services from 2017 to 2022: A retrospective study by Luke S-C Woon, Stephen Allison, Tarun Bastiampillai, Steve Kisely, Paul Maguire, William Pring, Rebecca Reay and Jeffrey CL Looi in Australasian Psychiatry
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
All primary data included in the study are publicly available from Services Australia.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.