
Abstract
Objective
This study evaluated the acceptance, feasibility and safety of a short-term group program for adults (18 years and older) and youth (16 to 18 years) with borderline personality disorder (BPD) symptoms. Termed Road Maps, the content and development were informed by common treatment factors identified from evidence-based therapies for BPD.
Method
Two-hundred and eight people consented to participate in the research trial and completed baseline measures. Intervention participants rated the acceptability and subjective experience of the group. Attrition rates informed feasibility, and serious adverse events were tracked to identify potential harms.
Results
Participant post-group ratings of the group’s acceptability and subjective experience were above average across both adult and youth populations. Attrition rate after commencement of group was 38% for adults and 27% among youth. The incidence rate of emergency department presentations was reduced by 41% in the 6 months post-group, relative to 6 months pre-group.
Conclusions
The current study provides preliminary support for the acceptability and feasibility of a short-term group therapy program for people with a diagnosis of BPD. Road Maps may be a useful intermediate intervention in a broader model of stepped care. Australian New Zealand Clinical Trials Registry, https://www.anzctr.org.au/ACTRN12622000849796.aspx, (ACTRN12622000849796)
Historically, recommendations for the treatment of borderline personality disorder (BPD) have steered away from short interventions given the pervasive nature of the condition and core relational symptoms relating to mistrust and fear of abandonment. 1 However, recently studies have reported adaptations of shorter versions (3 months or less) of DBT 2 and MBT 3 with encouraging findings. Nevertheless, the extensive training required to deliver specialist therapies is likely to limit broader implementation. 4 It has been proposed that less resource-intensive treatments be developed through integration of the common factors of effective BPD therapies. 5 These include procedural factors (specifically, a clear therapeutic framework incorporating a theoretical formulation, peer consultation and defining the structure of therapy) and intervention-based factors (e.g. active therapist stance, encouragement of agency, exploratory and change-orientated interventions). 6 However, there has been limited research into the practical application and effectiveness of such approaches, including in youth populations. This is concerning as there is strong evidence supporting early identification and intervention for young people with borderline symptoms. 7
The current paper describes the development of a short-term group intervention for youth with borderline symptoms and adults with a diagnosis of BPD. We report preliminary findings relating to treatment feasibility (i.e. attrition), safety (i.e. serious adverse events) and acceptability (i.e. post-group feedback).
Method
Procedure
Summary of inclusion and exclusion criteria.
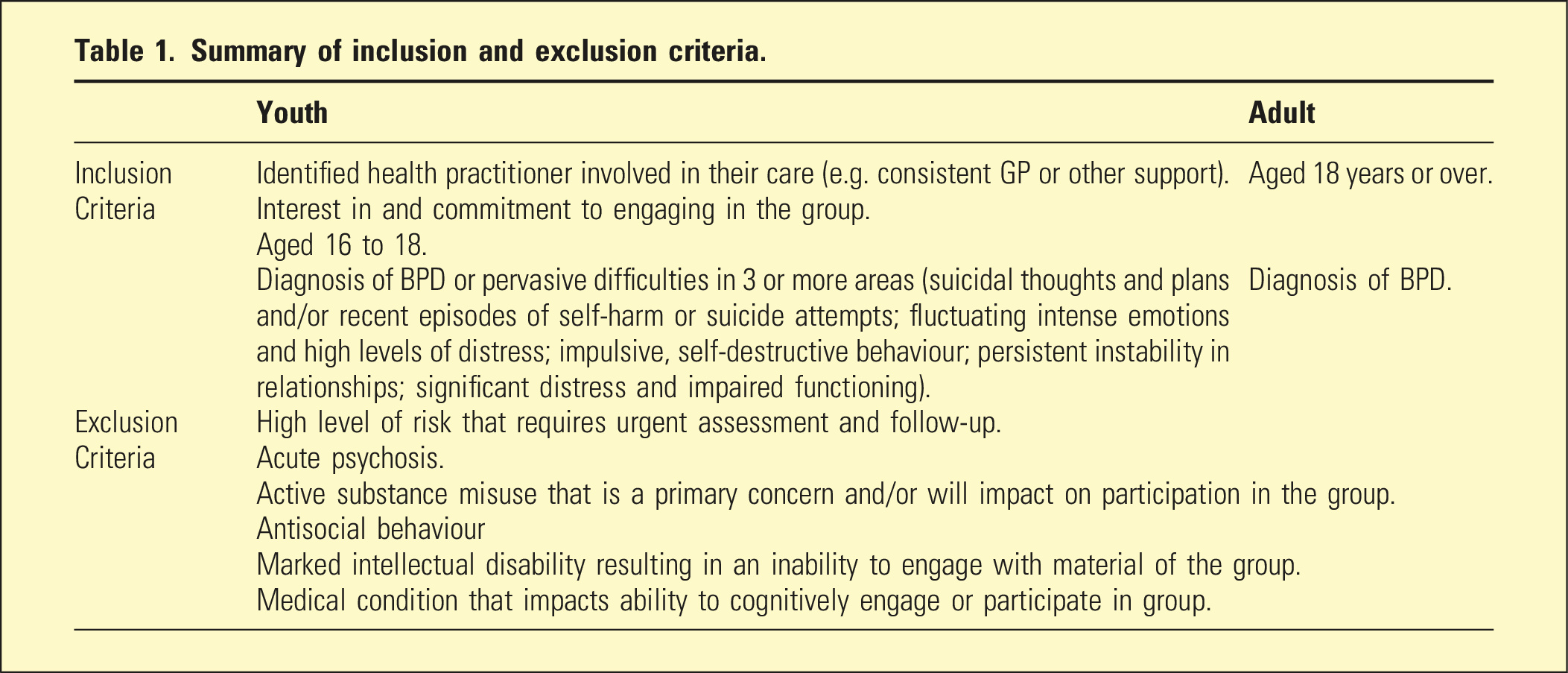
Intervention
Outline of Adult Road Maps intervention sessions/content.
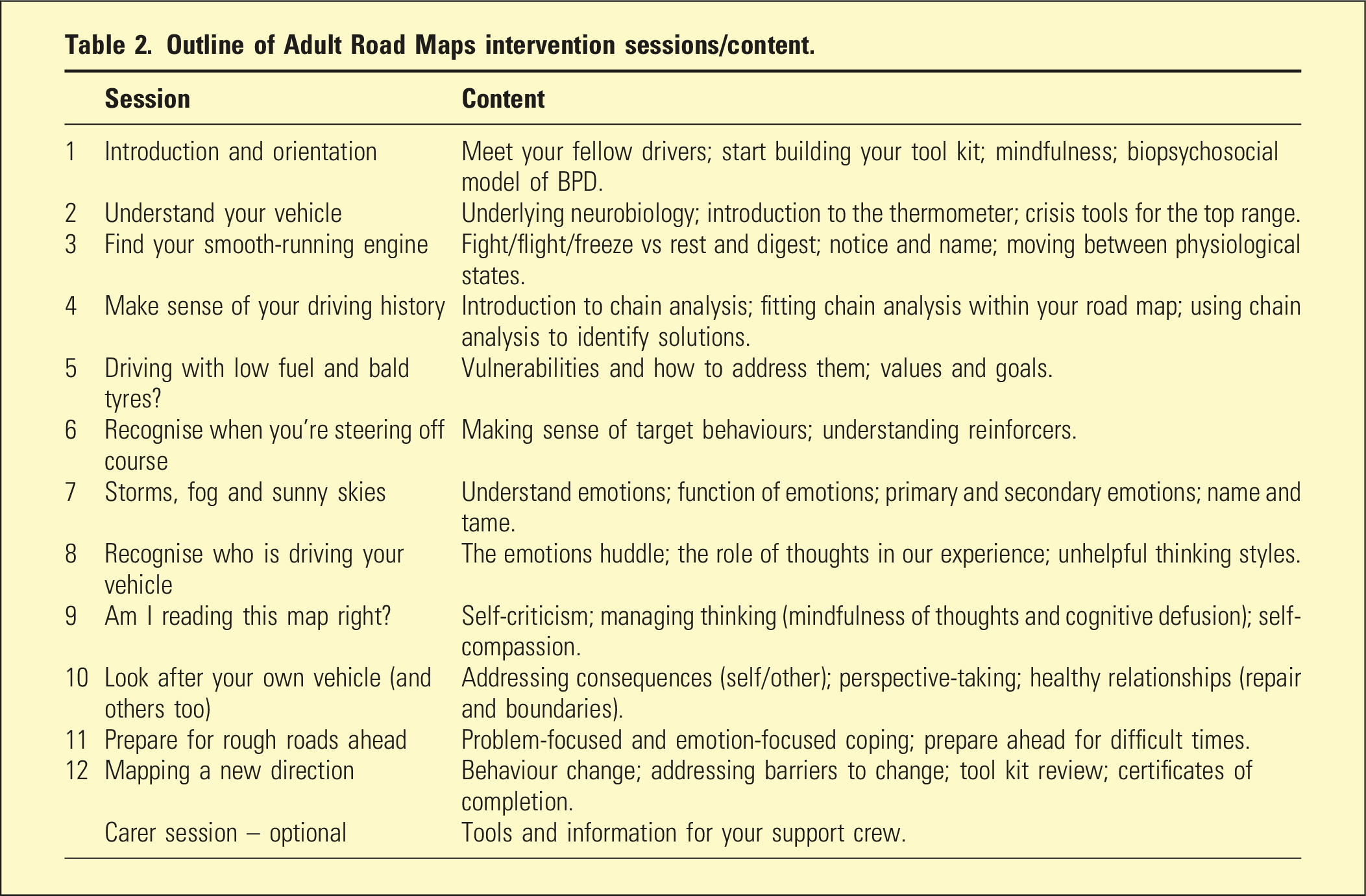
A key feature was the road map metaphor to demonstrate and increase comprehension of fundamental concepts and group content. Additionally, the group incorporated a fictional gender-neutral character to facilitate discussion around key concepts without reliance on participant self-disclosure. The group introduced a skill/technique each week and reviewed participant’s between-session application of skills to support generalisation. An optional carer information session was offered to increase familiarity and understanding of core concepts across participants’ support networks.
The adult group was offered weekly over a period of 12 weeks. Each session ran for 2.5 h including a 15-min break equating to approximately 30 h of contact. Adaptations to Road Maps for the youth group included reducing content, adding experiential exercises to sessions and shortening the length to 10 weeks to fit within an Australian school term. During the pandemic the adult and youth group moved online, as required. Group participants were offered a post-group assessment to review their clinical progress and where indicated discuss options for referral to a more intensive step-of-care (e.g. individual or group therapy and care coordination).
Measures
All participants were asked to complete a screening instrument for BPD (MSI-BPD) 8 to identify symptoms in line with a DSM-5 diagnosis. Borderline symptom severity and impulsive/self-destructive behaviour were also assessed using the borderline symptom list (BSL-23) and supplement (BSL-supp).9,10 These measures demonstrated adequate reliability, in this study, across adult (α = 0.96; α = 0.75) and youth groups (α = 0.91; α = 0.77). The results from these self-report tools provided the clinician with a profile of borderline symptoms which were verified during clinical interview.
Post-group attitudes about the intervention were collected using an adapted feedback form previously used for another short-term group trialed with people with borderline symptoms 11 with specific items regarding acceptability and appropriateness included. 12 Feedback items rated 3.5 or above were considered above average. In the current study, the reliability of this scale was good for both the adult (α = 0.91) and youth (α = 0.94) groups.
Treatment dropout was coded if a person attended at least one group session but less than 60% of all group sessions. Reasons for attrition, where available, were audited from clinical records. The clinical team followed the organizations’ requirements for reporting and responding to serious adverse events (SAEs). The research team tracked SAEs relating to death of a consumer. Further, mental health-related emergency department (ED) presentations, inpatient admissions and bed days were collated and compared 6 months before and after the Road Maps group across all research participants.
Statistical analysis
The dataset was screened for data entry errors and missing cases. Participant demographics, attrition rates and attitudes are reported descriptively. Mixed-effects negative binomial regression was used to analyse service utilisation given overdispersion and zero-inflation in the data distribution. A fixed-effect was specified for time (pre- vs post-group) and a random-effect for participant was included to account for repeated measures within individuals. The effect of time (pre- vs post-group) on the outcome was expressed as an incident rate ratio (IRR).
Results
Participant demographics and baseline clinical characteristics
Participant (N = 208) demographics and baseline clinical characteristics split by cohort.
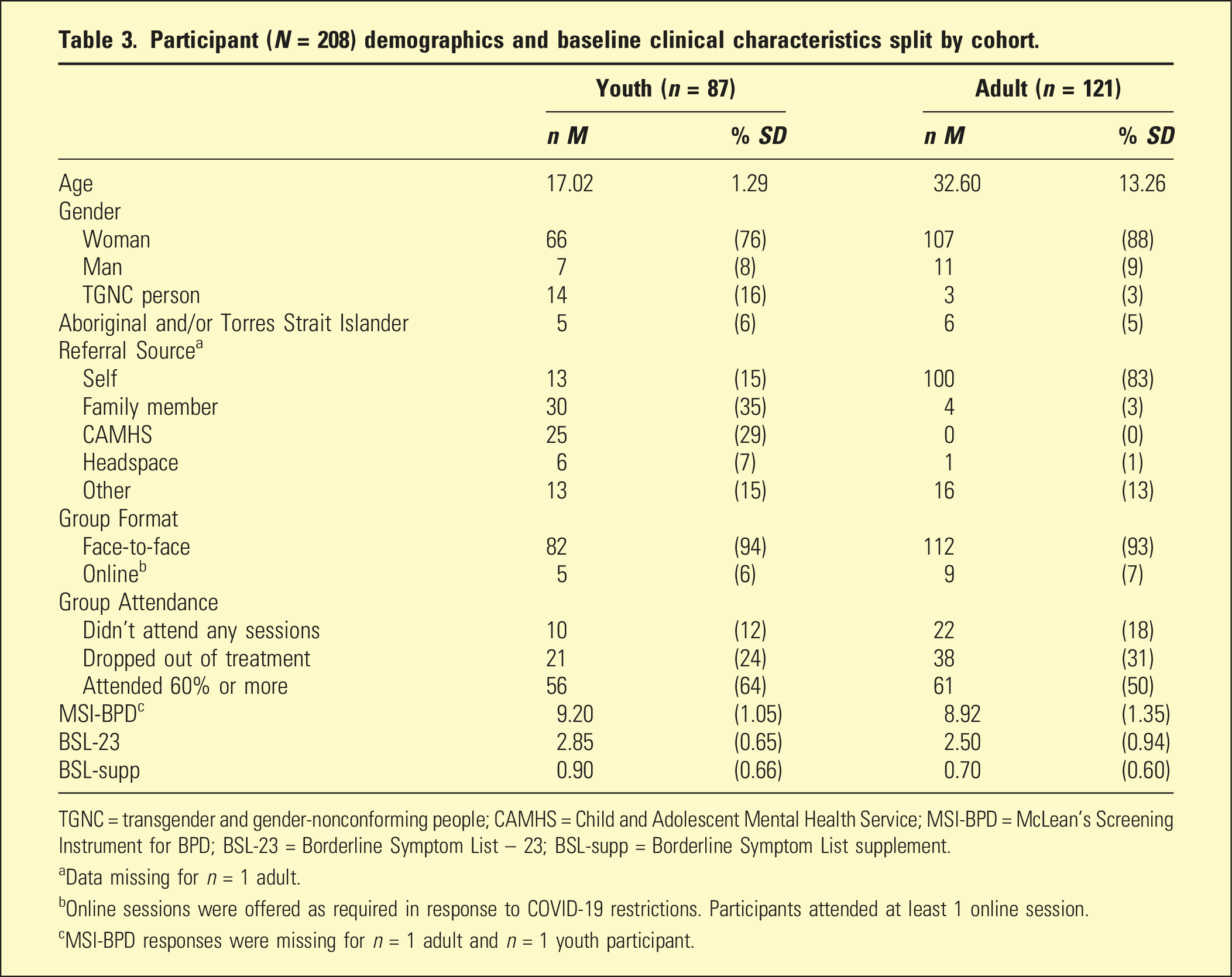
TGNC = transgender and gender-nonconforming people; CAMHS = Child and Adolescent Mental Health Service; MSI-BPD = McLean’s Screening Instrument for BPD; BSL-23 = Borderline Symptom List – 23; BSL-supp = Borderline Symptom List supplement.
aData missing for n = 1 adult.
bOnline sessions were offered as required in response to COVID-19 restrictions. Participants attended at least 1 online session.
cMSI-BPD responses were missing for n = 1 adult and n = 1 youth participant.
Acceptability and subjective use
Subjective evaluation of the group among adult and youth Road Maps participants who completed the post-group assessment (n = 99).
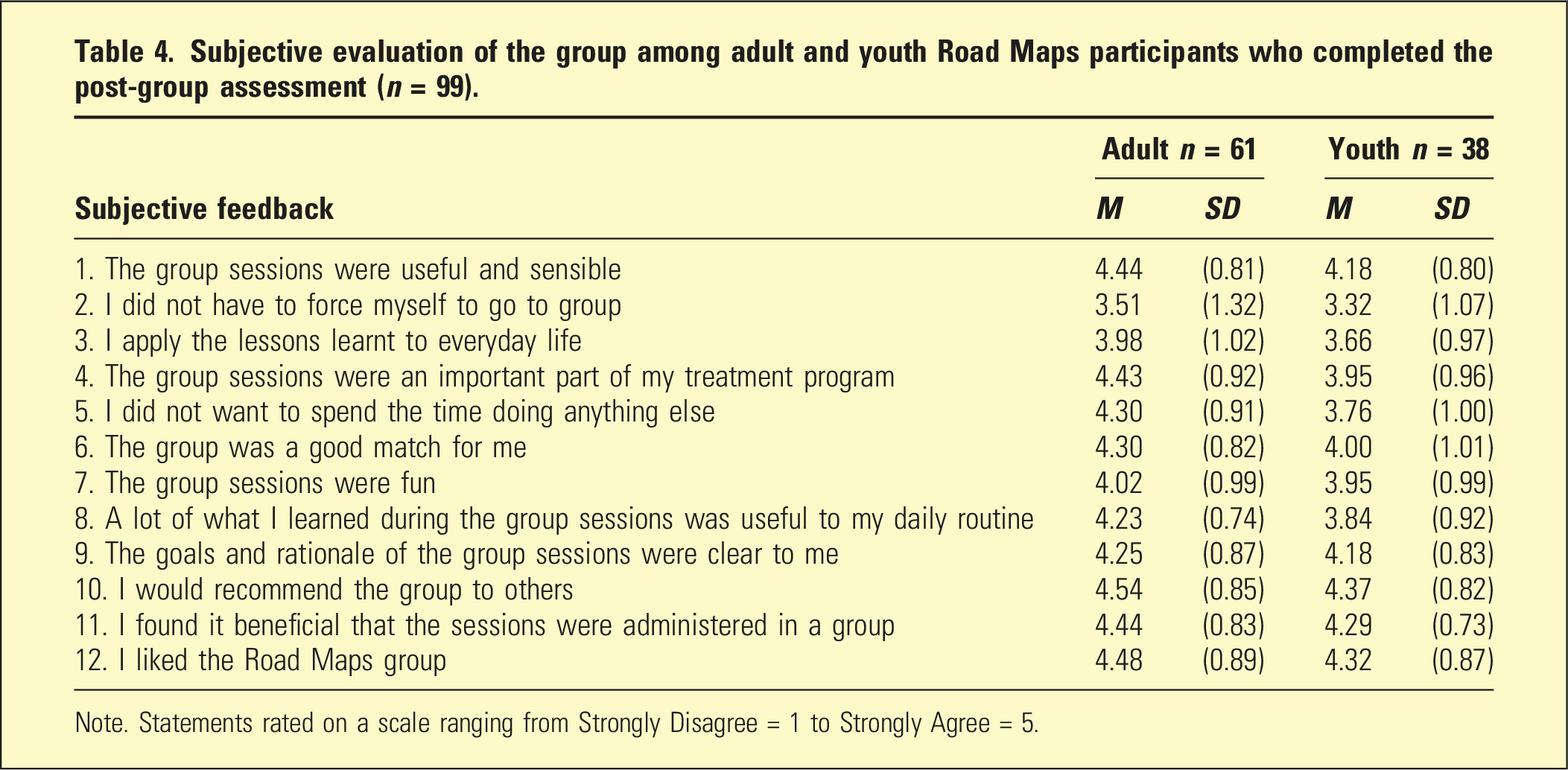
Note. Statements rated on a scale ranging from Strongly Disagree = 1 to Strongly Agree = 5.
Feasibility
After initial assessment, research consent and group acceptance, 10 youth (12%) and 22 adults (18%) did not attend any group sessions. Subsequently, 77 youth and 99 adults attended at least one group session, with 27% and 38% of participants in these cohorts attending less than 60% of sessions (i.e. treatment dropout). Reasons for treatment dropout, where available, predominantly reflected non-group related factors such as difficulty managing attendance with external life demands (i.e. employment/study, relocation and family stressors) or physical illness. Group-related factors for attrition were interpersonal (not feeling comfortable sharing in a group or not feeling connected to other participants) or in fewer instances related to content (e.g. not liking or understanding material).
Serious adverse events
There were no participant deaths reported during the study period. Service utilisation records (n = 202) indicated that 6 months before the group, 77 (38%) research participants had one or more mental health-related ED presentation/s, and 46 (23%) had one or more inpatient admission/s. In the 6-month period post-group, 42 (21%) participants presented to an ED and 29 (14%) had one or more inpatient admission/s. Examining data for research participants admitted as an inpatient post-group, revealed that seven participants hadn’t attended any group sessions, seven dropped out of treatment and fifteen attended 60% or more of the group. Mixed-effects negative binomial regression analyses demonstrated that the incidence rate of ED presentations in the 6 months following Road Maps was 41% lower relative to the 6 months before Road Maps (IRR 0.59, 95% CI [0.43, 0.82]; p = .002). Overall, there were no statistically significant changes in the incidence rate of inpatient admissions (IRR 0.70, 95% CI [0.46, 1.05]; p = .081) or bed days (IRR 1.39, 95% CI [0.73, 2.62]; p = .314) in the 6 months after the intervention relative to the 6 months beforehand.
Discussion
Participants across both group cohorts reported that they found the sessions useful and sensible, and they liked the group and would recommend it to others. Participants noted the sessions were important to their treatment plan and the group was a good match for them. The feasibility of the group was informed by attrition rates. A recent meta-analysis of treatment dropout across therapy for people with a diagnosis of BPD ranged between 22 and 30%. 13 In the current study, treatment drop out for youth (27%) was within this range while the adult group attrition was higher (38%). Of note, the evaluation occurred during the global pandemic, necessitating unanticipated changes to modality and strict enforcement of social distancing measures which may have exacerbated attrition. To reduce attrition, after-hours and online groups have since been offered to people who struggle to attend in-person or during standard working hours.
Serious adverse events were tracked during the study period, and there were no participant deaths reported. The incidence of ED presentations in the 6-month period post-group was 41% lower relative to 6 months before group. Among participants who commenced the group, 13% had an inpatient admission in the 6-month period after the group finished. Overall, the incidence rate of inpatient admissions and bed days did not significantly change. The potential benefits of a short group may outweigh the harms. Further research is required to identify pre-treatment indicators that can guide clinical decisions regarding the appropriateness of referral to an intermediate step-in-care versus escalation to more intensive interventions.
Overall, the findings of this study demonstrate promise for interventions developed based on both the procedural and intervention-based common factors identified in the literature. There were several limitations to this study. First, we describe preliminary data regarding the acceptance and feasibility of the intervention, it does not speak to the effectiveness of the program, nor how it fits within a broader model of stepped care or whether it can be scaled up within a health system. The clinical trial which will test the effectiveness of the intervention in reducing symptom severity and improving psychosocial functioning, as well as 6-month follow-up interviews exploring pathways of care post-group, is in progress and will address some of these limitations.
Footnotes
Acknowledgements
The authors would like to acknowledge the BPD Co clinical team and experts by lived experience who were involved in aspects of the Road Maps group development, recruitment, data collection and facilitation. We would also like to acknowledge Dr Martha Kent, Judy O’Sullivan and Cathy McLeod-Everitt for their roles in service development and implementation. Finally, many thanks to the participants willing to provide feedback on their treatment experiences.
Disclosure
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors undertook this research as part of their paid employment at the Borderline Personality Disorder Collaborative.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Trial registration number/date
Australian New Zealand Clinical Trials Registry ACTRN12622000849796/retrospectively registered on 16th June 2022.
Data Availability Statement
The data that supports the findings of this study are available on request from the corresponding author. Data are not publicly available due to privacy or ethical restrictions.