
Abstract
Objective
Trainees and Fellows of the Royal Australian and New Zealand College of Psychiatrists (RANZCP) work in complex interpersonal and organisational environments. Engagement in supervision can be a helpful way for trainees and Fellows to achieve interpersonal, professional, and organisational success. Supervision comes in many forms depending on the stage and state of one’s career. An awareness of different supervision models is relevant to trainees’ understanding of what is expected of them and their supervisors in their work and educational contexts. This paper explores the taxonomy of supervision models available to RANZCP trainees and Fellows in Australia and New Zealand.
Conclusion
Supervision is a heterogeneous concept with multiple aims, outcomes, and processes that change with ones’ stage of career.
Different types of supervision relevant to RANZCP trainees and Fellows, and key differentiating features and aims
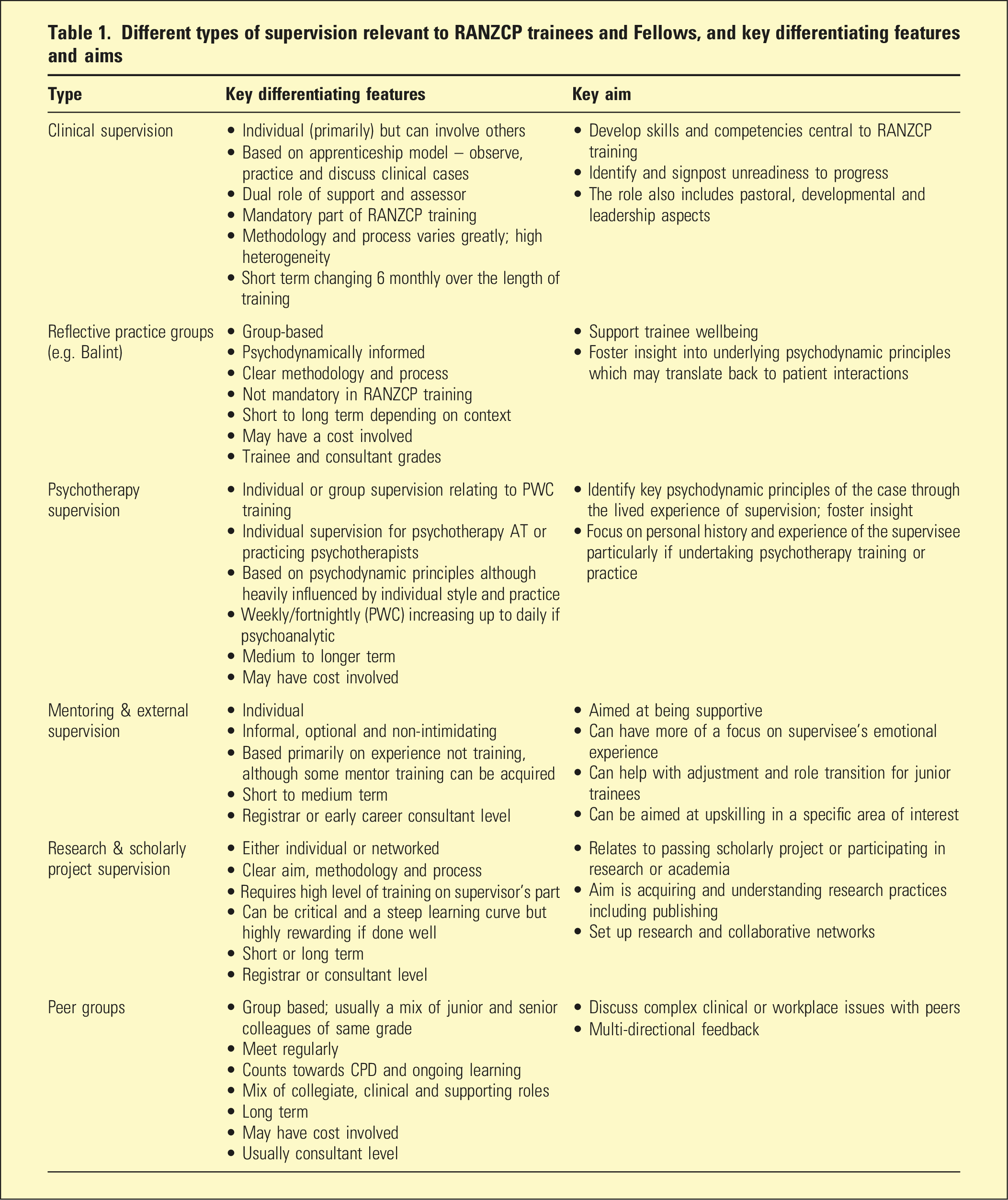
Clinical supervision
Duties of clinical supervisors (adapted from RANZCP Supervisor manual 2012) 1
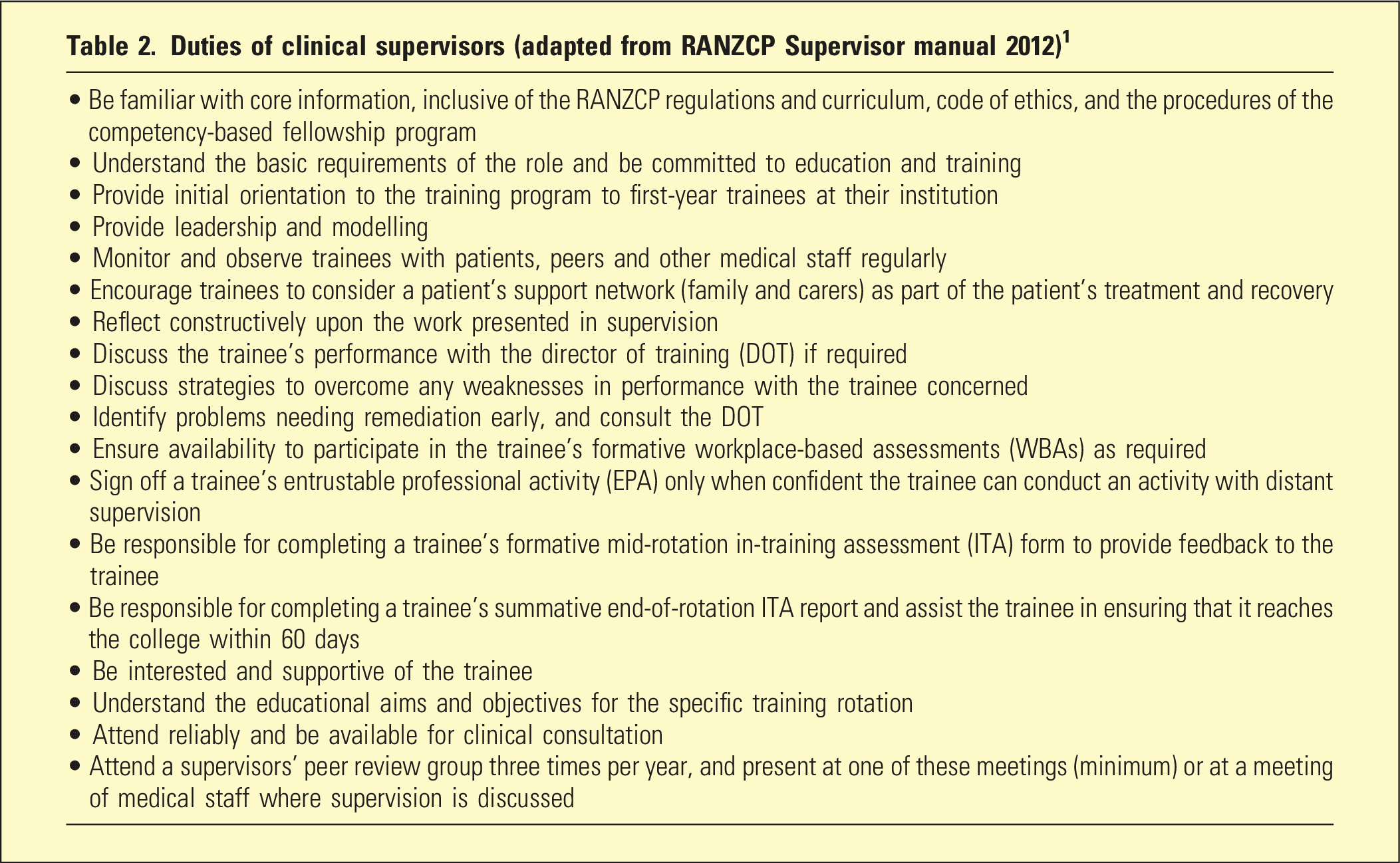
Good clinical supervision is said to be vital to protect trainee burnout, particularly early in training. 7 However, the practice of clinical supervision is highly variable, often with unclear goals based on limited evidence of effectiveness. 8 Clinical supervision is also poorly understood, particularly by trainees. 9 One survey found supervision objectives were not often clearly defined at the beginning of the rotation and that lack of structure, set times, flexibility, and frequent supervisor changes were barriers to a safe and supportive learning environment. 10 Another 2012 survey of trainees found that less than half thought their clinical supervisors were supportive of trainee’s medical student teaching role and did not discuss their teaching in supervision. 11
The change in the RANZCP’s assessment model in 2012 further shifted the focus of supervision to assessment over supportive or mentoring elements. 12 Proposed changes to the assessment model from 2024 are likely to continue this trend, as they replace high-stakes exams with workplace-based assessments as the basis of decisions about training progression. 13 This will present clinical supervisors with an even more complex set of competing responsibilities. These include professional development aspects such as fostering resilience, wellbeing, and an understanding of professional boundaries, to facilitating an understanding of therapeutic relationships and psychodynamic aspects of the work, whilst ensuring safe and effective clinical teaching and training, alongside additional assessment and pastoral, developmental, and leadership roles. 6 A potential workaround to this dilemma can be found in the Royal College of Psychiatrists (RCPsych) training in the United Kingdom (UK), where an Educational Supervisor (ES) is appointed separate from the clinical supervisor in order to externalise the monitoring of a trainee’s educational progress. 14
Reflective practice groups
Reflective practice groups, the most common of which are called Balint groups, refer to groups where practitioners participate in non-judgemental, clinical reflective practice facilitated by a trained supervisor. 12 Weekly Balint groups are a mandatory part of RCPsych training in the UK, but not the RANZCP training program. However, many local RANZCP training branches offer them, and they can also be privately arranged as ongoing CPD for psychiatrists. 15 Groups meet between weekly and monthly and usually have around five to ten people. Balint groups typically centre around a participant presenting an account of a perplexing or troubling patient encounter, which elicited a strong emotional reaction in the practitioner. 3 The other group participants then consider the emotional experience of both doctor and patient without referring to technical explanations or giving advice. The aim of this process is for participants to explore dynamics which might be involved in the interaction, and which may also play out in the group, such as parallel processes, transference and countertransference reactions, and various levels of identification and projective identification.15,16 Balint groups are intended to help practitioners understand their own and patient experiences, as well as deepen the understanding of complex psychodynamic aspects of cases, and may help assist with practitioner emotional well-being and preventing burnout.12,15
Peer groups
Another type of group supervision is a peer group. These usually meet between weekly or monthly, and consist of 5–10 psychiatrists of differing career stages, sometimes including senior trainees. As well as contributing to CPD, a peer group offers perspective sharing between professional equals in exploring complex cases, management decisions, and current trends in research or practice. These groups also provide a supportive and encouraging environment from others who understand the complexities and vicissitudes of the role. Peer groups can also focus on a theme to provide a forum for advice and reflection for psychiatrists working in a specific area of interest (such as clinical supervisors, private practice, or veterans’ mental health).
Mentoring & external supervision
Mentors and external supervisors both offer individual supervision. Mentors are generally referred to as teachers, advisors, or career coaches who are good at listening and talking in confidence with a mentee. 17 Usually, mentors and mentees meet fortnightly to monthly, sometimes when more professional guidance is needed, and at other times less frequently. 18 Common subjects are training, managing work-life balance, issues with supervision, career goals and plans, and suggestions about professional development opportunities. 18 Affirming the mentee’s strengths and interests and providing encouragement are also helpful. There is limited research evidence on the effectiveness of mentoring but it may help with burnout, and is thought to be particularly effective for senior trainees planning for the transition to Fellowship.19,17
Barriers to effective mentoring include the mentor being too critical, trying to solve mentees’ problems for them, interference with the psychodynamics of rotation supervision through processes such as splitting, and the blurring of boundaries between the professional, social, and other relationships of mentors and mentees. 18 Boundaries can be particularly challenging to negotiate in regional and rural practice. Mentoring may be individually or systemically organised – the RANZCP offers a mentoring program that gives both mentees and mentor participants programmed guidance for effective mentoring, as well as access to mentors from an area separate to their local organisation. 20
External supervision refers to a trainee or psychiatrist regularly seeing a senior colleague outside of their workplace for support and guidance with complex clinical, organisational, or workplace issues 21 or upskilling in a specific area. Given the seniority difference, the role includes a mentoring and supportive aspect, and may focus more on the supervisee’s emotional experience of their role, alongside facilitating career choices and direction.
Personal psychotherapy & psychotherapy supervision
As a RANZCP trainee, the psychotherapy written case (PWC) forms a significant aspect of assessment. 4 Supervision is most commonly conducted on an individual basis, but can also occur in groups of up to five trainees with three co-supervisors. Group supervision is more common in regional locations and has been deemed effective by trainees. 22 Psychotherapy skills training in psychiatry has also traditionally followed an apprenticeship model, whereby trainees develop competency by practicing and discussing the practice of psychotherapy with a supervisor, with minimal direct observation. 23 Many training sites cannot consistently provide access to accredited psychotherapy supervisors from within the workplace setting which leads to trainees seeking external supervisors. 23
Trainees undertaking advanced training in psychotherapy require ongoing psychotherapy supervision, the frequency and length of which is dependent on the modality of psychotherapy training undertaken, and involves discussing and formulating aspects of the case based on the psychotherapeutic principles being taught. 24 The RANZCP does not mandate private personal psychotherapy at any career grade but some professionals who choose to do this may find it beneficial, and requires another ongoing time and cost commitment. 25
Research and scholarly project supervision
Most research supervisors for the scholarly project are likely to be the trainee’s primary clinical supervisor. 26 However, seeking primary or secondary supervision from a university department of psychiatry can achieve greater networking and career development benefits. A trainee should actively seek out a supervisor who meets their research interests, including compatibility between both personality and professional approaches. 26 At the early career and trainee stage, academic supervision usually falls into role of a mentoring relationship. 26 Academic supervision can involve discussing mutual aims and goals of the research, including a timeframe and expected outcomes and publications, and assistance with learning research skills such as formulating research questions, choosing methodological approaches, ethics applications, data collection and analysis, and giving and receiving feedback on the write-up. 27 It may be helpful to put together a written supervisory agreement and to discuss potential boundary issues from the outset of supervision. 26
Other types of supervision
There are several other additional types of supervision that may be encountered, which are summarised in Table 3 in the supplementary material for completeness.
Conclusion
Though psychiatric supervision has continuously evolved, its roots are still principally grounded in the apprenticeship model. There are now more than six main types of supervision modalities relevant to RANZCP trainees and Fellows, with the clinical supervisor role remaining central but having competing aims. Changes to the RANZCP examination process are expected to significantly impact the clinical supervisor role, and may require supportive elements to be delivered through other modalities, such as mandated Balint groups or mentors, or considering splitting the role in a similar way to the ES position in the RCPsych program. Clinical supervisors may also benefit from additional specific training to help them maintain workforce needs and supportive working relationships whilst ensuring adequate assessment standards and critical rigour across different regions. This paper has summarised the aims and features of the current mix of supervision modalities available to RANZCP trainees and Fellows, offering an overview that may help make the process easier to understand and navigate.
Supplemental Material
Supplemental Material - Defining the passage of wisdom: A taxonomy of supervision for RANZCP trainees and Fellows
Supplemental Material for Defining the passage of wisdom: A taxonomy of supervision for RANZCP trainees and Fellows by Edward Miller, Michael James Weightman, Andrew Amos, and Stephen Parker in Australasian Psychiatry.
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.