
Abstract
Objective
To explore the concept of, ethics surrounding, and arguments for and against cosmetic psychiatry.
Conclusions
Cosmetic psychiatry may be defined as the science and practice of interventions that subjectively enhance the mental states of healthy people. Cosmetic medicine (including surgery) is a professionally and socially accepted part of contemporary medical practice; cosmetic psychiatry is not. Like cosmetic medicine, there are significant risks associated with cosmetic psychiatry. There is an urgent need for a broader conversation about this emerging clinical reality.
Keywords
‘I’m sorry, but all this ADHD doesn’t add up’, wrote British journalist Dominic Lawson. 1 Lawson had probed the seemingly communicable spread of attention deficit hyperactivity disorder (ADHD) amongst celebrities and interrogated the validity of this phenomenon. Through a disease-centred lens, Lawson was arguably right to be sceptical. Through a cosmetic-centred lens, however, perhaps less so.
So-called aesthetic medicine is loosely defined as ‘all medical procedures aimed at improving the physical appearance and satisfaction of the patient’. 2 Most are more familiar with the analogous term ‘cosmetic medicine’, which includes cosmetic surgery. In cosmetic medicine, a diagnosis is not required for an intervention to be provided; pathophysiology nonessential; but patient satisfaction is paramount. Cosmetic interventions may include nutrition, drugs, blades, lasers, vacuums, needles and syringes. 2 There is an expanding array of such cosmetic interventions on offer, legally available and readily accessible, all intended to subjectively enhance the human physical condition. But what about subjective enhancement of the human mental condition?
Examples of prominent individuals who have described subjective enhancement of the mental state from psychotropic substance use. Terence McKenna controversially proposed that human evolution from Homo erectus to Homo sapiens (with development of human consciousness, cognition and culture) was driven by consumption of psilocybin-containing mushrooms - the so-called ‘stoned ape theory’. 6 More recently, and perhaps more plausibly, some anthropologists have hypothesised that humans may have evolved to ‘counter-exploit’ plant neurotoxins. 7 Modern history provides several examples of the ‘counter-exploitation’ of neurotoxins in prominent, professionally successful people (see below). It is important to note that professional success or prowess does not necessarily equate to health or mental health; the degree to which several of the following individuals were, in fact, ‘mentally healthy’ remains debatable

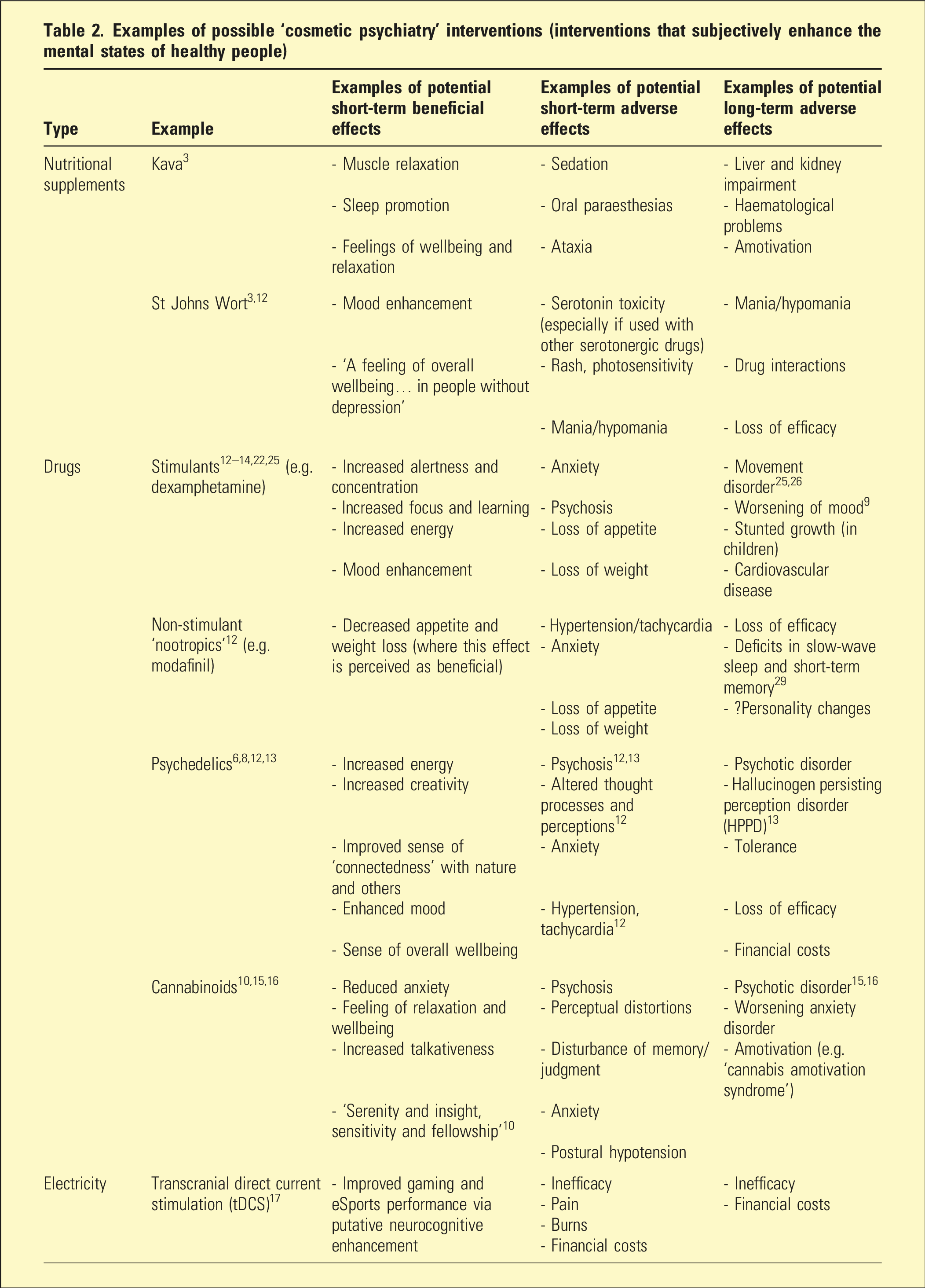
Examples of possible ‘cosmetic psychiatry’ interventions (interventions that subjectively enhance the mental states of healthy people)
The case for
The first argument is Descartian – why should there be cosmetic surgery but not cosmetic psychiatry? Why is it accepted that doctors may subjectively enhance the face of a healthy person, but not their mental state? Giannini argued psychiatry should rise above the disease-centred goal of ‘objective cure’ 3 to assist individuals attain the cosmetic-centred goal of ‘subjective perfection’. 3 Ethicist Arthur Caplan argued ‘brain enhancement’ 14 through cosmetic psychopharmacology is an individual human right that, where appropriately informed, is a choice that should be free from the gatekeeping of doctors and governments. 14 Caplan argued for people’s rights to ‘the best brains possible’, even opining that, ‘religious and secular cultures alike reward those who seek betterment’. 14 On the grounds of so-called cognitive liberty, advocacy for legal access to cognitive-enhancing drugs is increasingly prevalent. 15
It has been argued that the professionally guided, supervised use of psychotropics is safer and more effective than self-prescribed or recreational use. 3 Indeed, the call for regulation of all psychotropic substances, as opposed to prohibition, is an old and arguably rational one. Given their medical training and psychopharmacological expertise, some psychiatrists may be optimally placed to mediate such regulation. Regarding non-pharmacological interventions, passing electricity into the brain is best professionally regulated; self-administered electroconvulsive therapy (ECT) has resulted in burns and skin grafting, without therapeuticity. 16 Transcranial direct current stimulation (tDCS) is an increasingly popular performance-enhancing tool for gaming and eSports; 17 unregulated use exposes consumers to risks of inefficacy and harms (e.g. burns) but also financial exploitation.
The benefits of cosmetic psychotropic use in those who serve society are well documented. Stimulants have long been used by sleep deprived soldiers, pilots and sailors, and have played an important role in several wars. 18 Some military doctors have opined that, ‘the healthy human has vast untapped potential’ and that it would even be, ‘remiss if we did not seek to improve performance in sleep-restricted environments’. 19 Former US president, Barack Obama, was suspected to use modafinil 20 and, under his administration, White House staffers reportedly used modafinil and z-drugs to optimise performance and sleep/wake cycles whilst working ‘around the clock on high-stakes issues’. 21 Unsurprisingly, it has been asked if similar benefits may be derived from psychotropic use in sleep deprived doctors (e.g. improved attention and alertness leading to reduced errors, etc.). 22 The ethics therein remain underexplored.
Finally, clarifying psychotropic use as cosmetic-centred rather than disease-centred may improve precision of mental health statistics and epidemiology which may optimise health policy and funding allocation. For example, many psychotropics currently require a specific diagnosis to be legally prescribed. Where a drug is cosmetically prescribed, but a diagnosis erroneously given so as to legally provide it (e.g. stimulant for subjective neurocognitive and energy enhancement, but diagnosis of ADHD provided), the prevalence of the putative disorder is falsely inflated. Indeed, recent data suggests that by year four of their course, up to 61.8% of US college students were offered prescription stimulants for non-medical use, and up to 41.5% had used them. 23 This issue may be partly responsible for ‘all this ADHD’ 1 and consequent calls for the National Disability Insurance Scheme (NDIS) to cover it. Thus, rather than perpetuating an ‘epidemic’ of a previously relatively uncommon adulthood disorder, acceptance of cosmetic psychiatry may generate a wealth of useful data regarding psychotropic use in otherwise healthy people.
The case against
The first counterargument is Descartian – the body is not the mind. Surgically altering one’s face is merely renovating the shopfront, whereas chemically altering one’s mental state may appear to alter the very essence of one’s being (e.g. perhaps Kramer was physically listening to his patients, but hearing Prozac). Substance-related personality changes can occur in context of substance use disorders, especially when longstanding. 24 Numerous websites report substance-related personality changes, including with so-called smart drugs. Theoretically, such changes could be biologically mediated but substance-influenced role changes, distorted temperaments, changed interpersonal styles and altered psychosocial functioning could all hypothetically contribute.
Regarding access, the libertarian argument for free informed choices requires that people are sufficiently informed. Consider a thought experiment: the ‘cosmetic psychiatry clinic’. Even if a psychiatrist set up a ‘cosmetic psychiatric clinic’ with appropriate training, stringent safeguards, regulatory oversight and comprehensive capacity assessments for consent to mental-state-enhancing interventions in healthy people (e.g. stimulants), it would still require that individuals could provide sufficiently informed consent. Short-term effects of most commonly used psychotropics are well-known, long-term effects less so. Given the current paucity of knowledge regarding long-term adverse effects, sufficiently informed consent may therefore be impossible to provide. Some evidence suggests many short-term benefits of psychotropics are lost long-term; 25 other evidence suggests more serious potential harms. Long-term stimulant use (recreational or prescribed) has been associated with permanent movement disorders;25,26 ketamine use associated with irreversible bladder damage; 27 SSRI use with permanent sexual dysfunction; 28 psychedelics and cannabinoids with chronic psychotic disorders. 13 Though lacking firm data, some experts hypothesise long-term modafinil use is associated with deficits in slow-wave sleep and memory 29 and even cancer. 30 Such long-term associations are rarely discussed. Advocates for wider access to tryptamines and methylenedioxymethamphetamine (MDMA) hastily cite drug harms ranking studies 31 to promote the safety of these substances. Ironically, according to these same studies, psychedelics and MDMA sit adjacent antipsychotics, 31 molecules with tremendous potential for harms, especially long-term. There simply is no such thing as a neurochemical free lunch.
The specific area of psychotropic neurocognitive enhancement, so-called ‘neuroenhancement’, 19 has been heavily debated. Chatterjee examined four key areas of concern including (a) impacts on character and individuality, (b) safety, (c) distributive justice (e.g. only the wealthy having access) and (d) coercion. 22 The latter deserves further attention. In a neoliberal capitalist society, productivity and performance are crucial and anything that enhances these parameters, indispensable. If neuroenhancing drugs were made legally available and readily accessible, it is possible that employers or corporations may implicitly or even explicitly mandate them. In a market-driven culture where everyone uses neuroenhancement, those who do not may fall behind and potentially lose their employment removing any need for explicit mandates. Exploring this conundrum, Appell argued for both unencumbered legal access to psychotropic neuroenhancement, but also legal protections to ensure it remained uncoerced. 32 However, even if appropriate regulatory safeguards were implemented, it is doubtful they would ensure complete protection – as evidenced by illegal breaches of regulations in finance, elite sports and gambling, etc. Similar concerns apply to university, research and other important areas such as schools and scholarships where psychotropic neuroenhancement may offer a putative advantage. In this context, cosmetic psychiatry emerges as a form of naive unfettered consumerism, a manifestation of a materialist society where the pursuit of more or better outweighs all other considerations.
Finally, one crucial counterargument is that cosmetic psychiatry is simply not psychiatry. Strictly interpreted, the RANZCP definition of psychiatrist suggests no role outside of ‘diagnosing and treating people with mental illness’. 33 The stay-in-your-lane argument is that psychiatrists are in the business of healing the sick, not bettering the well. This argument demands there be other, non-psychiatric, professionals who provide, guide and supervise mental-state-enhancing interventions in otherwise healthy people. If one accepts this argument, it dictates there be another term to describe the practice (e.g. ‘psychocosmesis’ or ‘mind-enhancing medicine') as cosmetic psychiatry is a contradiction in terms.
Conclusion
This paper is not about extolling the benefits of supplements, psychotropics, electricity or other potentially mental-state-enhancing interventions. Nor is it an advocacy piece for legalisation of use or access to them. It is about considering the ethics and reality of interventions, substance or otherwise, that subjectively enhance the mental states of healthy people and whether psychiatrists have any role in providing, guiding and supervising these. There are arguments either way.
Unlike cosmetic medicine, cosmetic psychiatry is yet to be socially and professionally accepted. Meanwhile, the pursuit of (both lay and professional) interventions that subjectively enhance the mental states of otherwise healthy individuals continues unabated. Cosmetic psychiatry is a conversation that urgently needs to be had.