
Abstract
Objective
A lack of access to psychiatric services for adult ADHD is a recognised issue in South Australia and nationally. This study aims to explore the practices of local psychiatrists and their attitudes towards adult ADHD, with a view to determining any barriers influencing accessibility to treatment.
Methods
We developed an online survey to examine the aims of the study. Free text boxes were included to obtain qualitative data. Quantitative data were tallied and presented as percentages. Qualitative data (free text responses) were analysed thematically.
Results
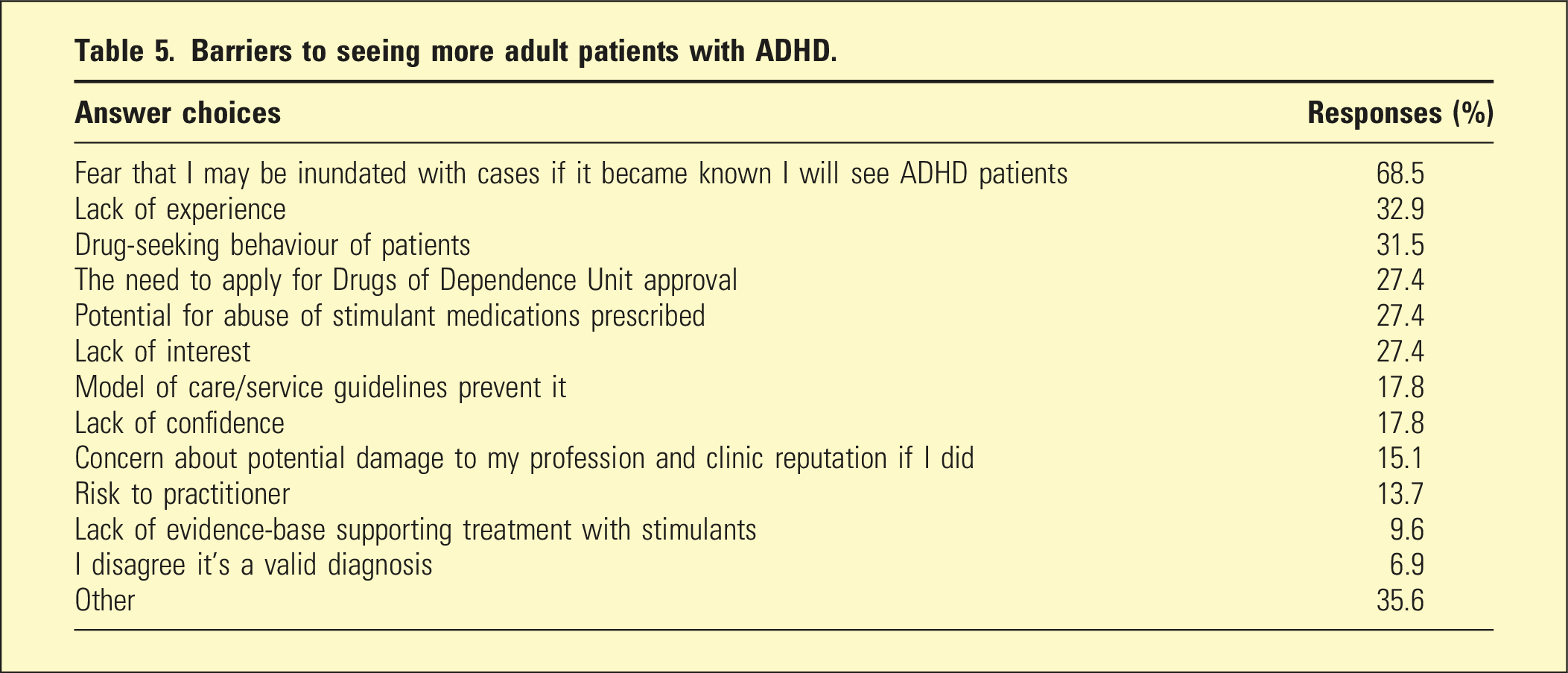
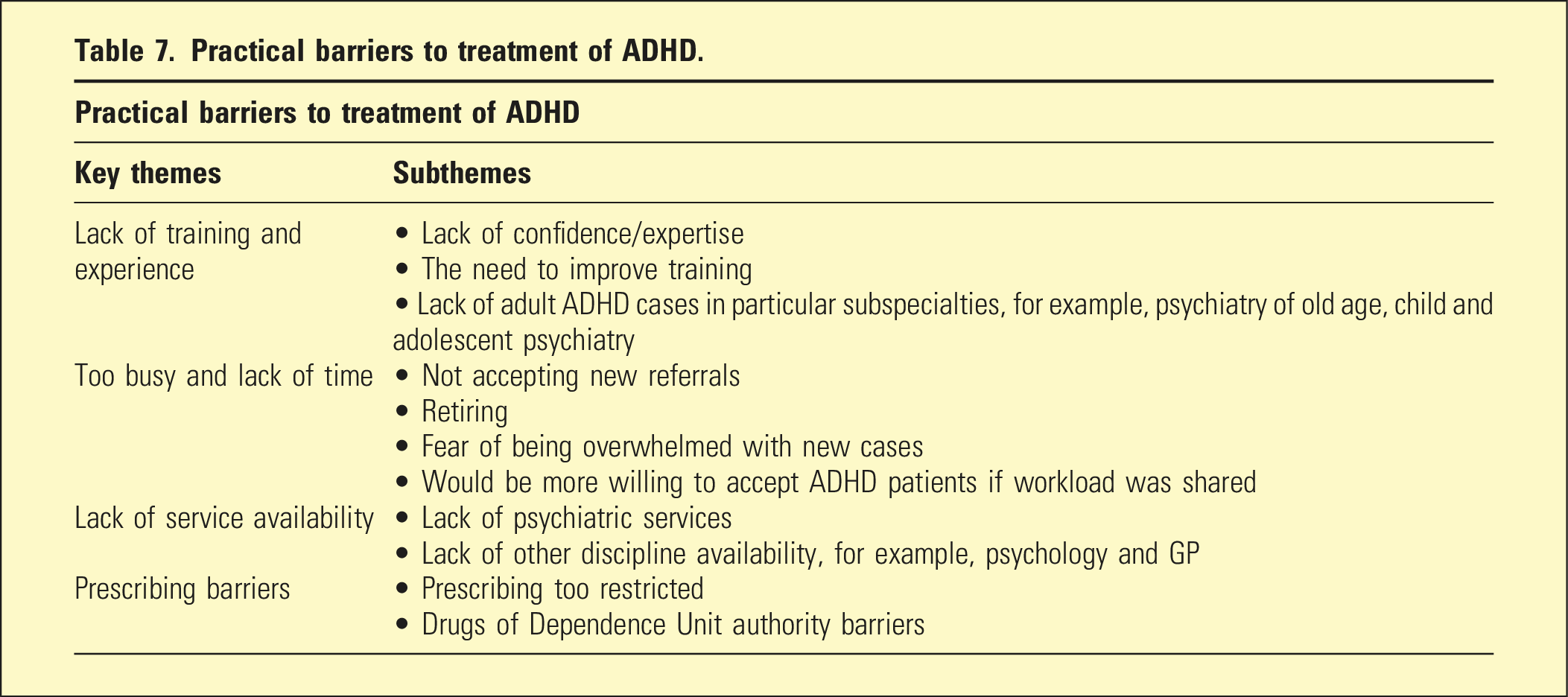
73 out of 322 psychiatrists responded (22.7%). The greatest barrier to seeing adult ADHD was the fear of being inundated with cases (68.5%), followed by lack of experience managing ADHD (32.9%), and potential drug-seeking behaviour of patients (31.5%). Two overarching qualitative themes were identified: practical barriers and attitudinal barriers.
Conclusion
ADHD service provision is complex and relates to many systemic factors such as public versus private, funding, and service organisation. More psychiatrists need to become involved in treating ADHD so that the work is more widely spread. Increased training in ADHD is also needed to increase confidence in managing the condition.
Attention Deficit Hyperactivity Disorder (ADHD) is a recognised and treatable neurodevelopmental disorder characterised by persistent patterns of inattention and/or hyperactivity-impulsivity that interfere with functioning or development. 1 Studies show ADHD prevalence rates of about 2%–7% in children 2 and adults. 3 The condition is associated with significant functional consequences, particularly if untreated. In childhood, this is evident through reduced academic performance and social rejection, 4 which may manifest in adulthood as higher probability of unemployment, 5 comorbid mood and substance use disorders, 5 and higher rates of criminal activity.5,6
Despite high estimated prevalence rates, lack of access to psychiatric services for the assessment and treatment of adult ADHD is a recognised local issue in South Australia. 7 The models of care of most public adult community mental health services specifically exclude offering services for ADHD, 8 and the numbers seeking treatment appear to far outweigh the available private psychiatrists. Lack of service availability not only creates frustration for those seeking treatment, but potentially contributes to societal illness burden due to the known functional consequences of untreated ADHD. 9 Research has estimated the impact of untreated ADHD to cost the Australian economy over $20 billion each year. 10
Difficulty accessing adult ADHD services is not limited to South Australia. The recently published ADHD Clinical Practice Guideline (AADPA) identified that existing services across Australia are difficult to access due to long waiting times and out-of-pocket costs, and that optimal care involving a multi-agency approach is rarely available. 11
Several overseas studies have surveyed healthcare providers to explore this matter12–20 but we were unable to find a mixed methods study that explored attitudes of psychiatrists towards adult ADHD with an open-ended approach. As far as we are aware, there is no published research on this topic from Australia.
Aim
The aim of this study was to explore the attitudes and practices of South Australian psychiatrists towards adult ADHD, with a view to determining any local contextual factors influencing accessibility to treatment. We aimed to explore any barriers that may influence psychiatrists’ decisions to provide adult ADHD services.
Method
Survey development
We developed an online survey to explore the objectives of the project. The questions were based on the attitudes and barriers identified from our literature review and from our conversation with staff from the South Australian branch of the RANZCP (June 2019). The survey was organised into the following areas: four demographic questions about the participants’ practice; 10 questions about caseload, referral patterns and approaches to treatment; 16 questions on attitudes and opinions about ADHD and its treatment, presented as statements followed by a five-point Likert scale; multiple answer checkbox questions identifying barriers to seeing adult patients with ADHD (the specific options included were chosen from responses in overseas studies,14–16 as well as anecdotally from RANZCP staff). Free text boxes were also included after each question where the participant could add their own comments about the statement proposed. This was included to obtain qualitative information to add a richer nuanced understanding, in addition to the quantitative information obtained from the Likert scales. Finally, there were two free text responses seeking additional comments and suggestions for change.
Ethics
Ethics approval was granted via the University of Adelaide Human Research Ethics Committee (HREC). Approval number H-2020-124.
Participants and recruitment
Permission was obtained from the RANZCP to use their email distribution list for South Australian psychiatrists. The first recruitment email was sent to all actively practising Fellows in South Australia on 30th July 2020, followed by a reminder email on 17th August 2020. Written consent was obtained online at the start of the survey.
All South Australian psychiatrists who were actively practising were eligible to participate. Participation in the survey was voluntary with no direct communication between researchers and participants. No identifying details were collected from participants. Completion of free text response boxes was voluntary; however, all other questions required a response before proceeding.
Data analysis
Quantitative data were descriptively analysed using percentages. The free text responses were analysed by separating these into themes. As many of the free text responses extended more broadly than the specific question asked, we chose to combine all the free text responses and analyse them together, rather than analysing the qualitative data for each question independently. The qualitative analysis of free text responses was informed by the six-stage process described by Braun and Clark, 21 a widely used approach in qualitative research. In our study, investigators independently reviewed all the free text responses and organised them into codes and themes. Investigators then met to compare their individual analyses and through an iterative process reached a final consensus on the key themes and subthemes. The free text responses were reviewed again to ensure all responses were covered by one of the subthemes.
Results
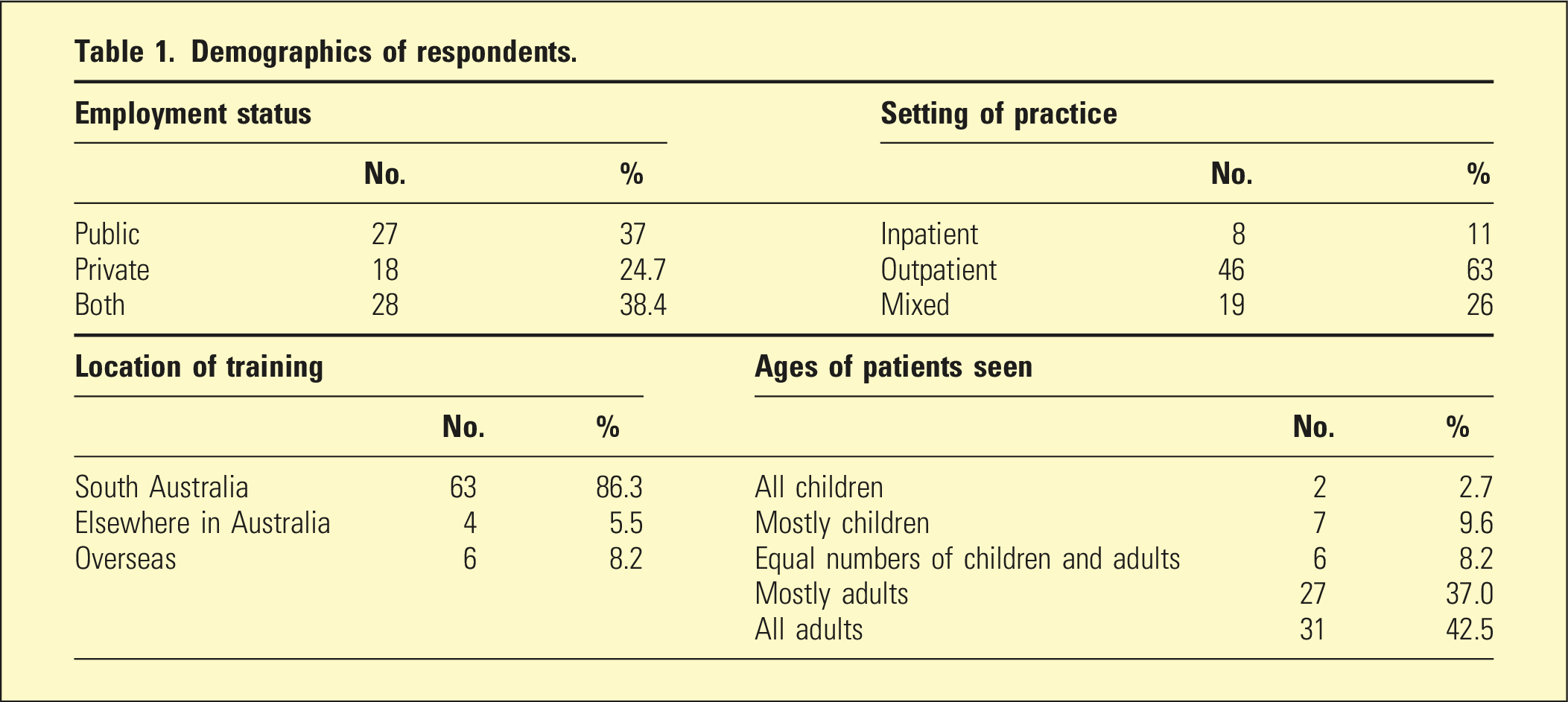
Demographics of respondents.
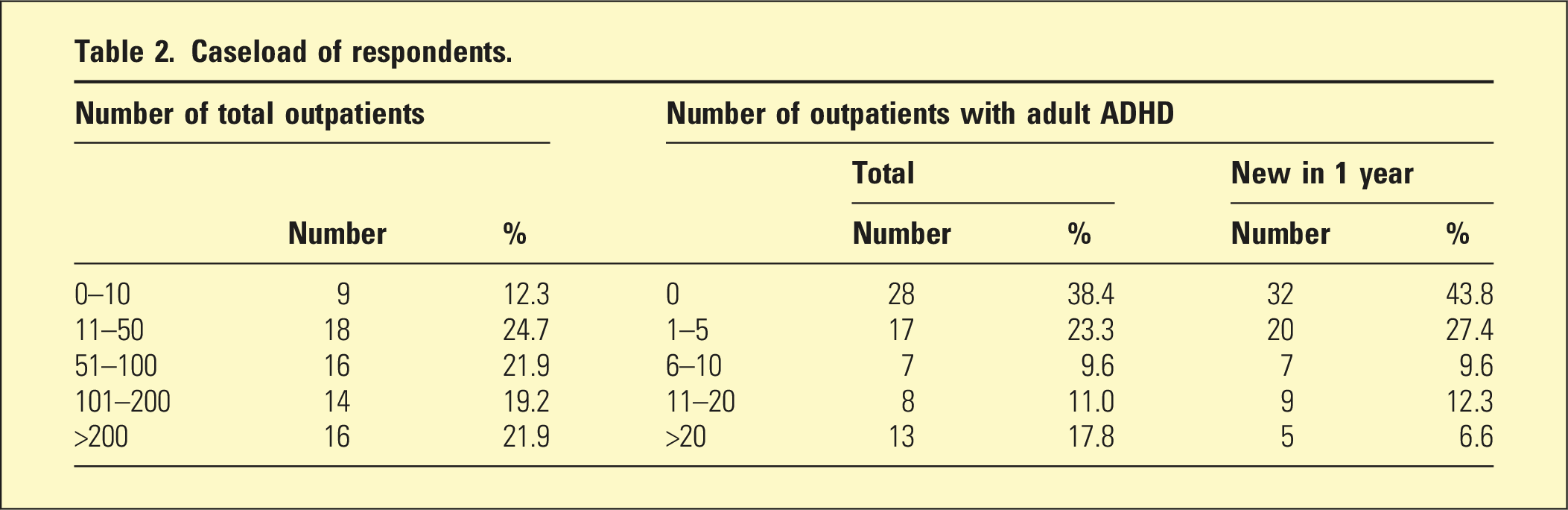
Caseload of respondents.
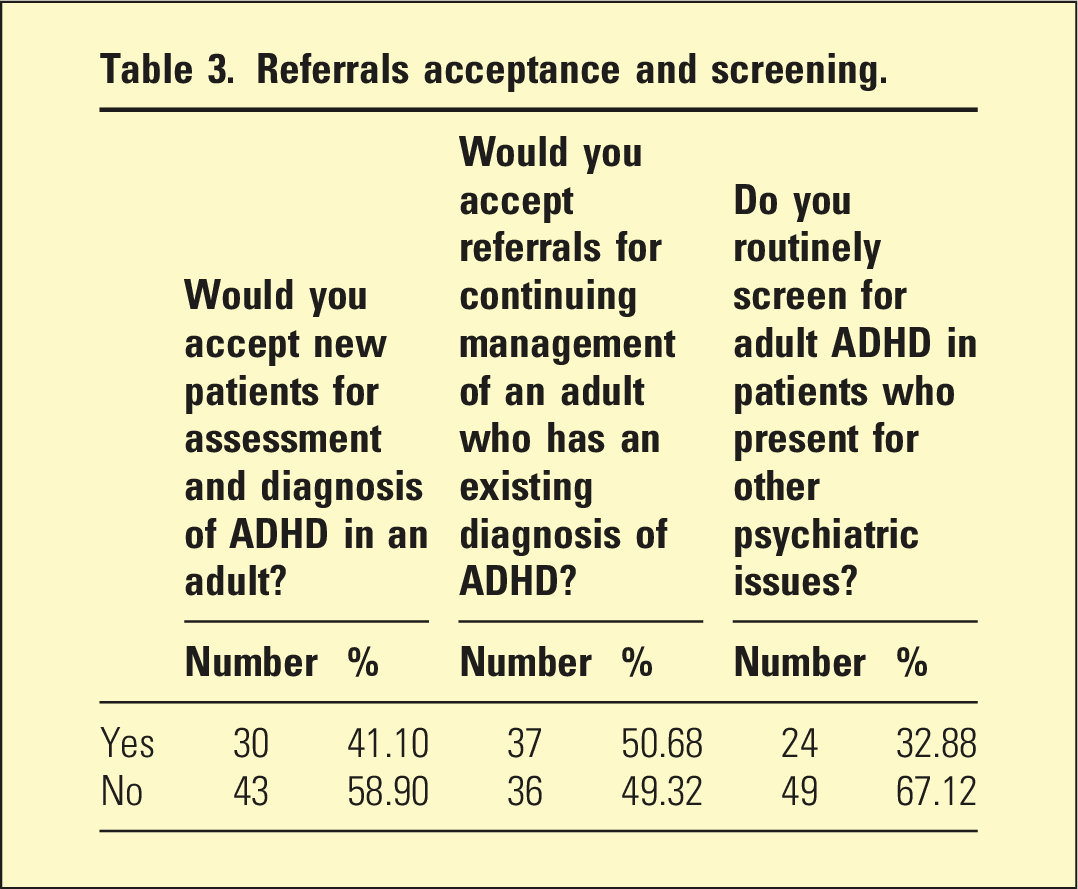
Referrals acceptance and screening.
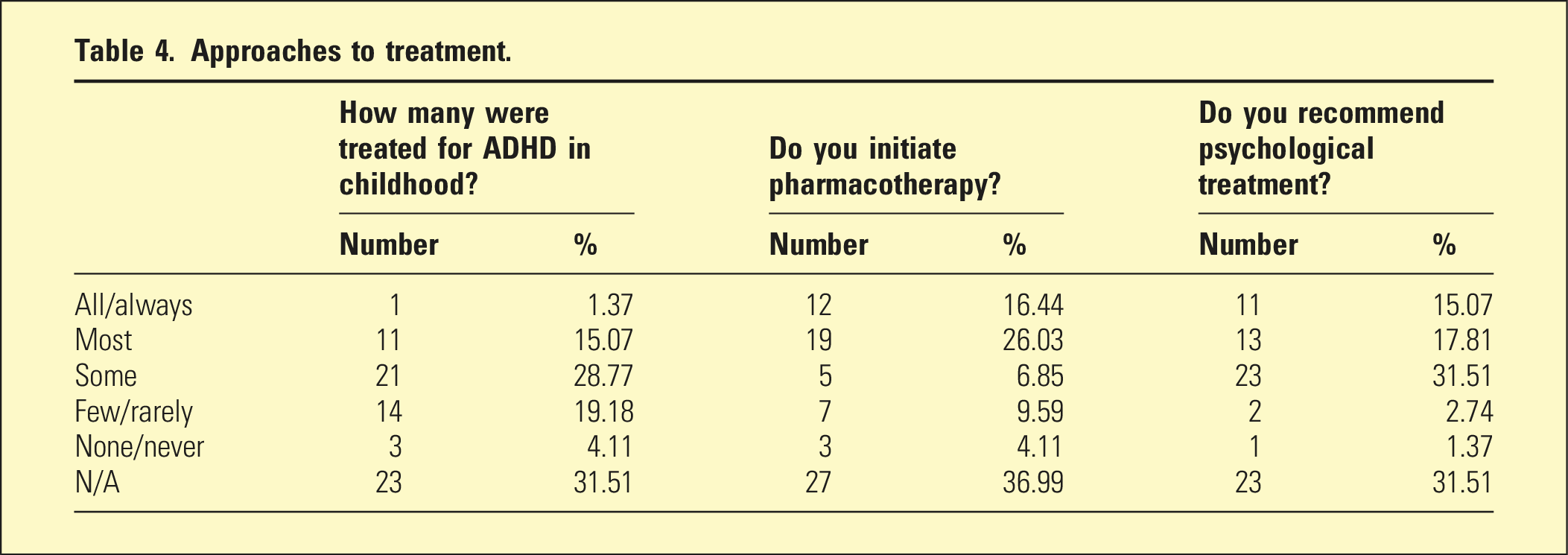
Approaches to treatment.
Barriers to seeing more adult patients with ADHD.
Likert scale questions.
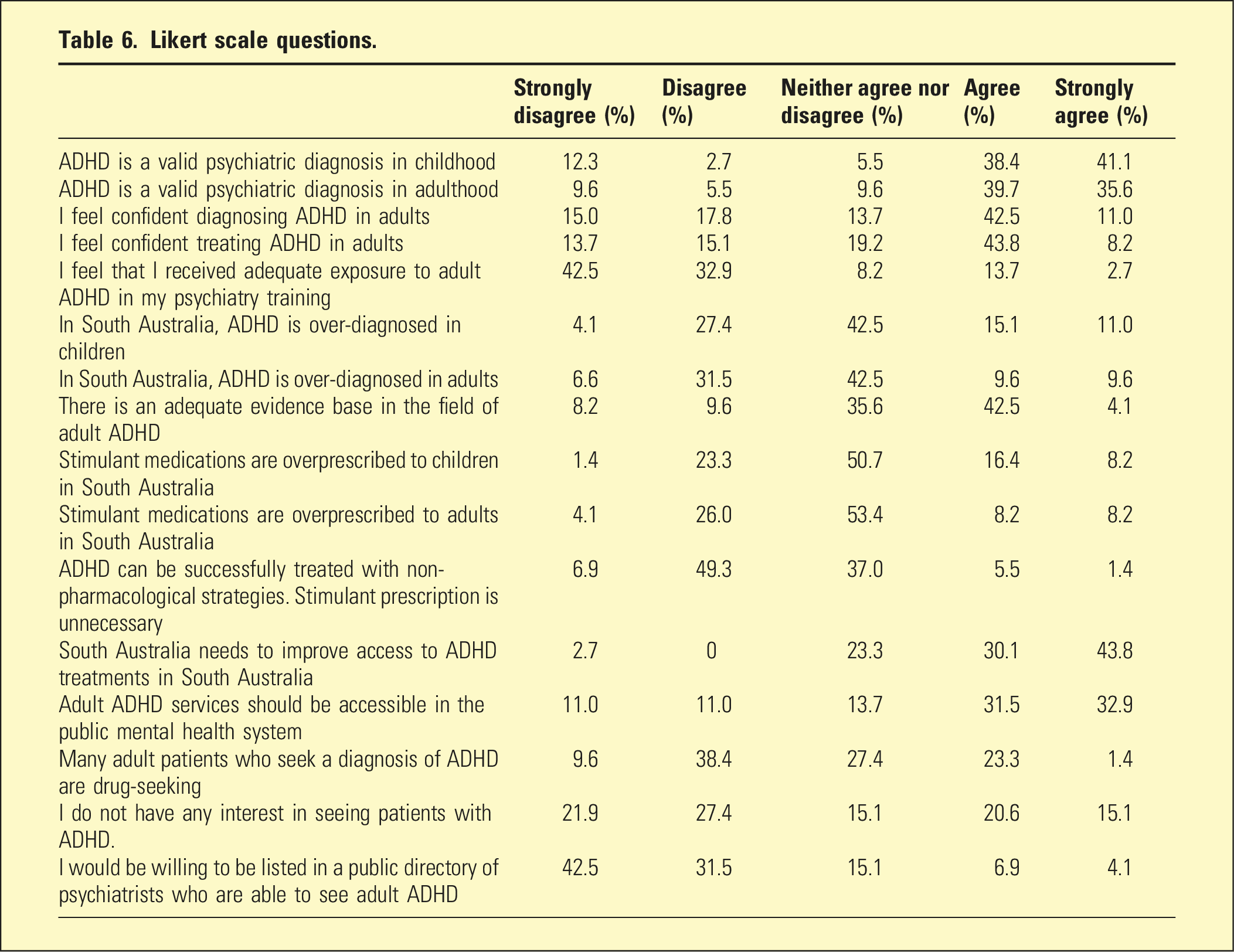
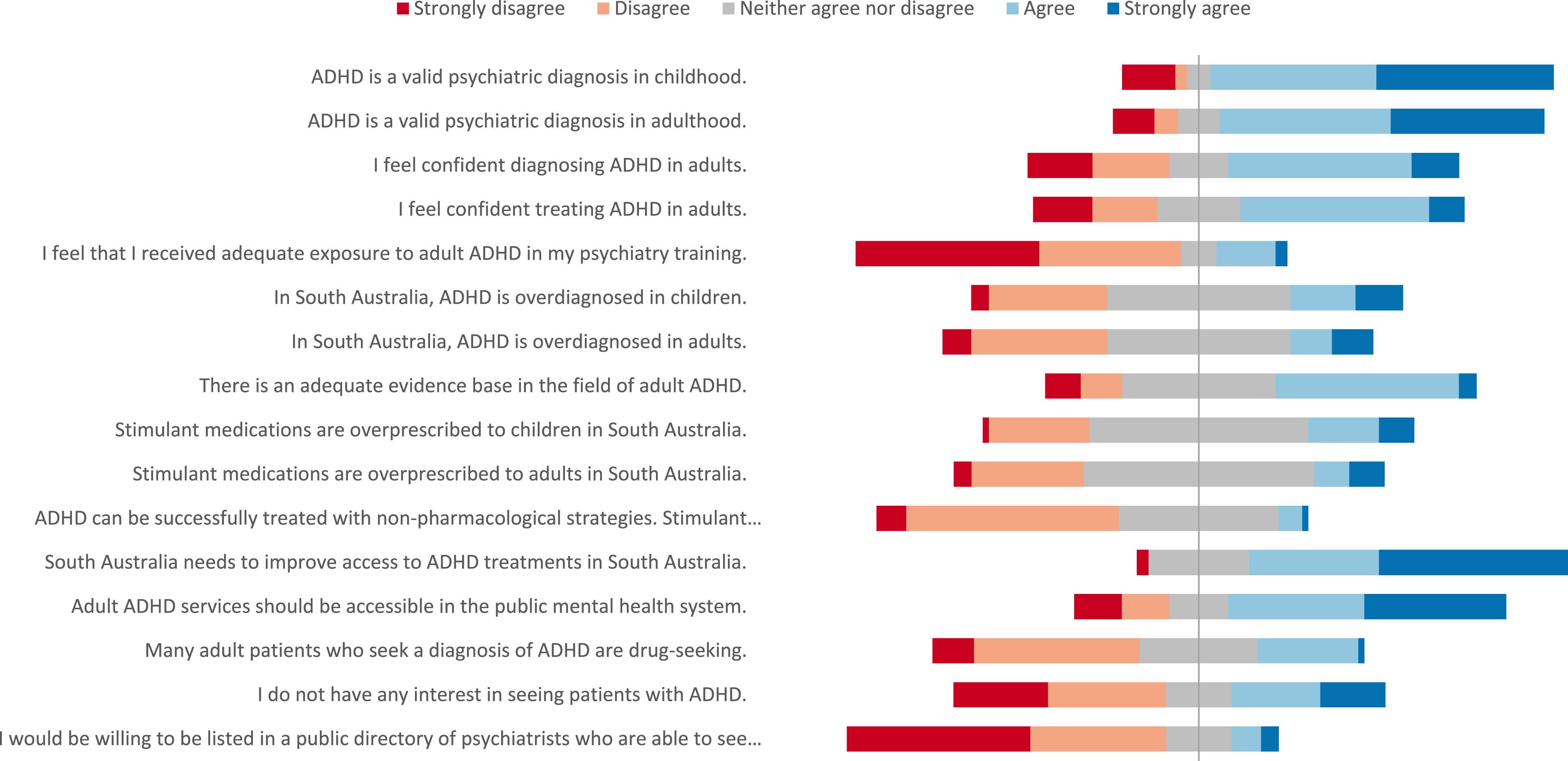
Likert scale questions.
Practical barriers to treatment of ADHD.
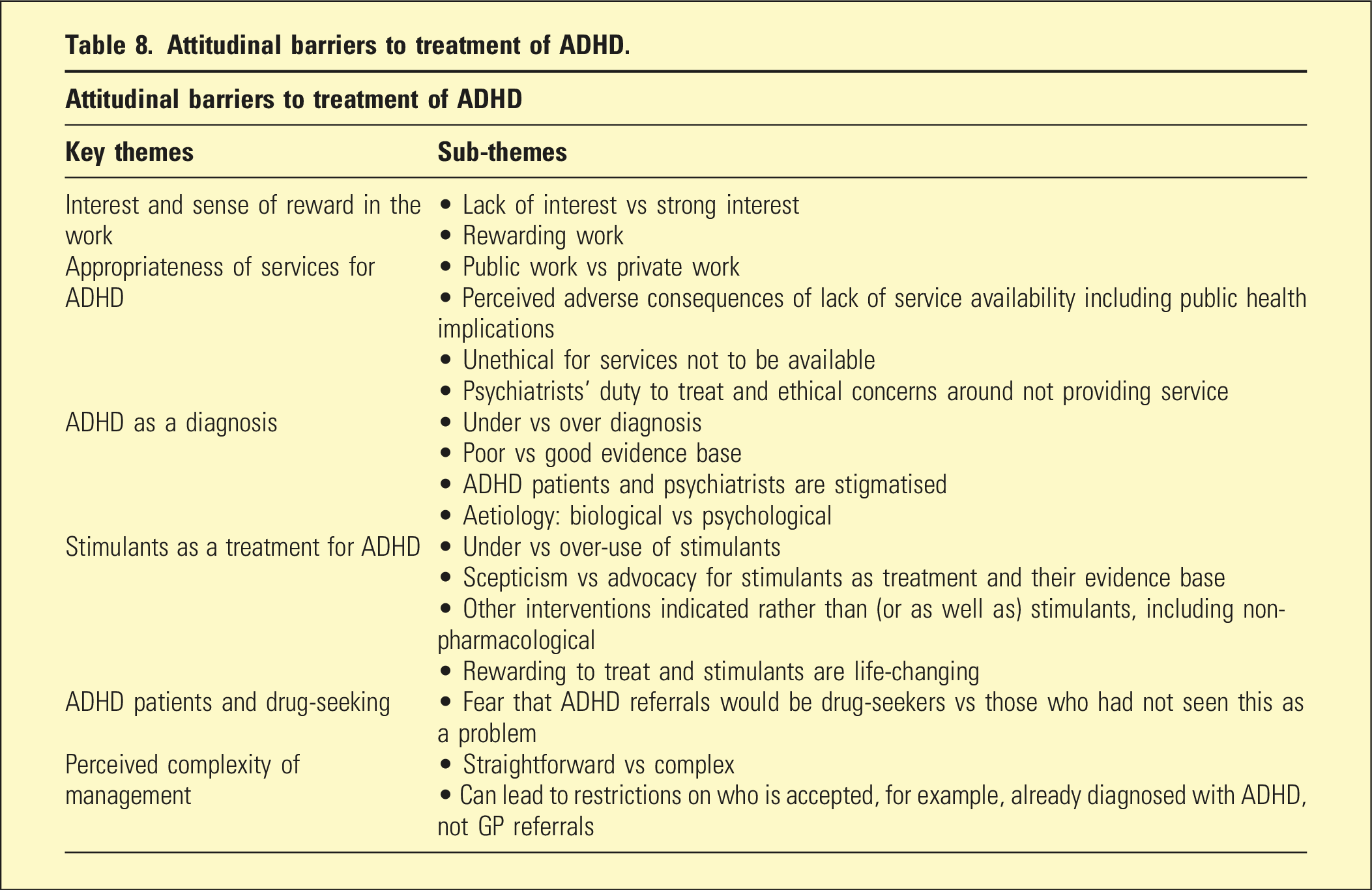
Attitudinal barriers to treatment of ADHD.
Discussion
Despite the pivotal role psychiatrists play in managing ADHD, less than half of psychiatrists stated they would accept new referrals for ADHD patients and only 11% were willing to be listed in a public directory advertising this. Patients with adult ADHD will therefore find it challenging to access a psychiatrist to assess and manage their illness, which also raises ethical issues regarding psychiatrists’ duty of care and lack of access to a much-needed service. 64.5% felt that treatment should be provided by public mental health services as the associated complexities require a multidisciplinary approach.
The reluctance to join a public directory aligns with the biggest barrier to seeing more adult ADHD, namely, a fear of being inundated with new referrals. This then becomes a self-perpetuating problem as the lesser the psychiatrists there are available to treat ADHD, the more inundated the few who do make this known will be, perpetuating fear of work overload and maintaining access difficulties. This cycle can only be broken by a sufficient number of psychiatrists making it known that they will treat ADHD so the workload is redistributed.
Lack of training, experience, and confidence are key issues. This is concerning with ADHD being one of the disorders in which adult psychiatrists are expected (by the public and regulatory authorities) to have expertise. A concerning three-quarters of psychiatrists stated they did not receive adequate exposure to ADHD during their psychiatry training and may be reflected in the fact that only 32.88% of psychiatrists routinely screen for ADHD. One reason for this, in South Australia at least, is that almost all management of ADHD occurs in private practice, but almost all Fellowship training occurs in public practice, thus not allowing trainees any exposure. Most psychiatrists believed there should be more ADHD treatment available in the public system and this would help address the training shortfall. Also, developing more training opportunities in private practice could address this deficiency.
Challenges in accurately diagnosing ADHD and the complexities of management were also barriers. Certainly, this would be amplified by training gaps, which prevent these skills from being developed. However, these opinions were balanced by others who felt treatment is straightforward and rewarding. One explanation for these varying attitudes could be that ADHD cases encountered in the public system are comorbid and complex, thus giving public psychiatrists a skewed perception of the complexity.
The perceived inadequacy of evidence may reflect the wide heterogeneity of opinions regarding aetiology and diagnostic clarity, including whether ADHD is in fact a psychiatric issue. One-fifth did not feel that ADHD was a valid diagnosis in adulthood, increasing to one-quarter for childhood ADHD. There was consensus that as a neurodevelopmental disorder, ADHD does not arise de novo in adulthood and the symptoms should be present in childhood, even if not formally diagnosed.
A minority of psychiatrists believed ADHD was over-diagnosed, which was mirrored in attitudes to stimulant prescribing. Despite the evidence for stimulant treatment of ADHD being as robust as pharmacological treatment of most other common disorders in adults,22,23 less than half felt there was an adequate evidence base. One explanation could be the gap in training. If trainees are not taught this evidence and have little incentive to study it, then they may conclude that the evidence does not exist.
Fears about drug-seeking by ADHD patients was a barrier for a minority of respondents, despite this being a common anecdotal concern. These fears and beliefs may be unfounded, as the comments made by other psychiatrists were that drug-seeking is not a common problem.
Limitations
The cross-sectional nature of the survey, conducted in 2020, does not account for changes in opinion over the past few years as a result of increased advocacy and awareness on this topic. The response rate of 22.7% is also quite low and the opt-in nature of the survey is subject to self-selection bias.
Conclusion and recommendations
There is a recognised lack of services for adults with ADHD in South Australia. 7 Given the significant impact of untreated ADHD,4–6 there is an imperative to increase access to appropriate assessment and management. Our study has examined the attitudes and practices of local psychiatrists to determine factors that may be contributing to the current situation. The most consistent themes were those of practical barriers to care. Attitudinal barriers, while heterogeneous, were surprisingly less prominent and perhaps stem from lack of experience working with this patient group.
More psychiatrists need to become involved in treating this cohort of patients, so that the fear of being inundated with ADHD referrals is eased by spreading the workload more widely. This study supports the contention that increased training in ADHD is an important strategy to allow more psychiatrists to feel comfortable managing this disorder. One recommendation is to provide access to more ADHD-focused professional development opportunities to upskill psychiatrists who would be willing to take a caseload of ADHD patients. Another recommendation is to increase training opportunities for registrars. A potential solution is to include public ADHD teaching clinics within established adult community mental health services, which would require services to embrace treatment of this patient population more than they do at present. Another option would be to create more training opportunities within private practice, especially with those psychiatrists who do already manage adults with ADHD.
Our findings also show that adult ADHD service provision is complex and relates to many systemic factors in terms of the segregation of public versus private sectors of care, health care funding and mental health service organisation. Further research to better understand the interplay of systemic factors may yield more solutions.
Footnotes
Acknowledgements
The authors would like to thank Ms Trudy Lisk (Branch Coordinator, RANZCP South Australian Branch) for her assistance in this project.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.