To examine the treatment of gender dysphoria described in Bell v Tavistock (UK 2020). Bell documents the treatment and sequelae of a 16-year-old adolescent referred to the Tavistock with gender dysphoria. Her case highlights contrasts between gender affirming care and comprehensive care.
Conclusions
Consistent with other western centres, in the 2010s, the Tavistock began treating patients with gender dysphoria under the ‘Dutch protocol’ for gender affirming care. Bell reveals concerning lapses of clinical governance influenced by activists and linked to patient harm. The recent suspension of a senior child psychiatrist from an Australian public hospital service after questioning the evidence base and ethical foundation of gender affirming care underlines the need to resolve these uncertainties to address the crisis in the treatment of gender dysphoria.
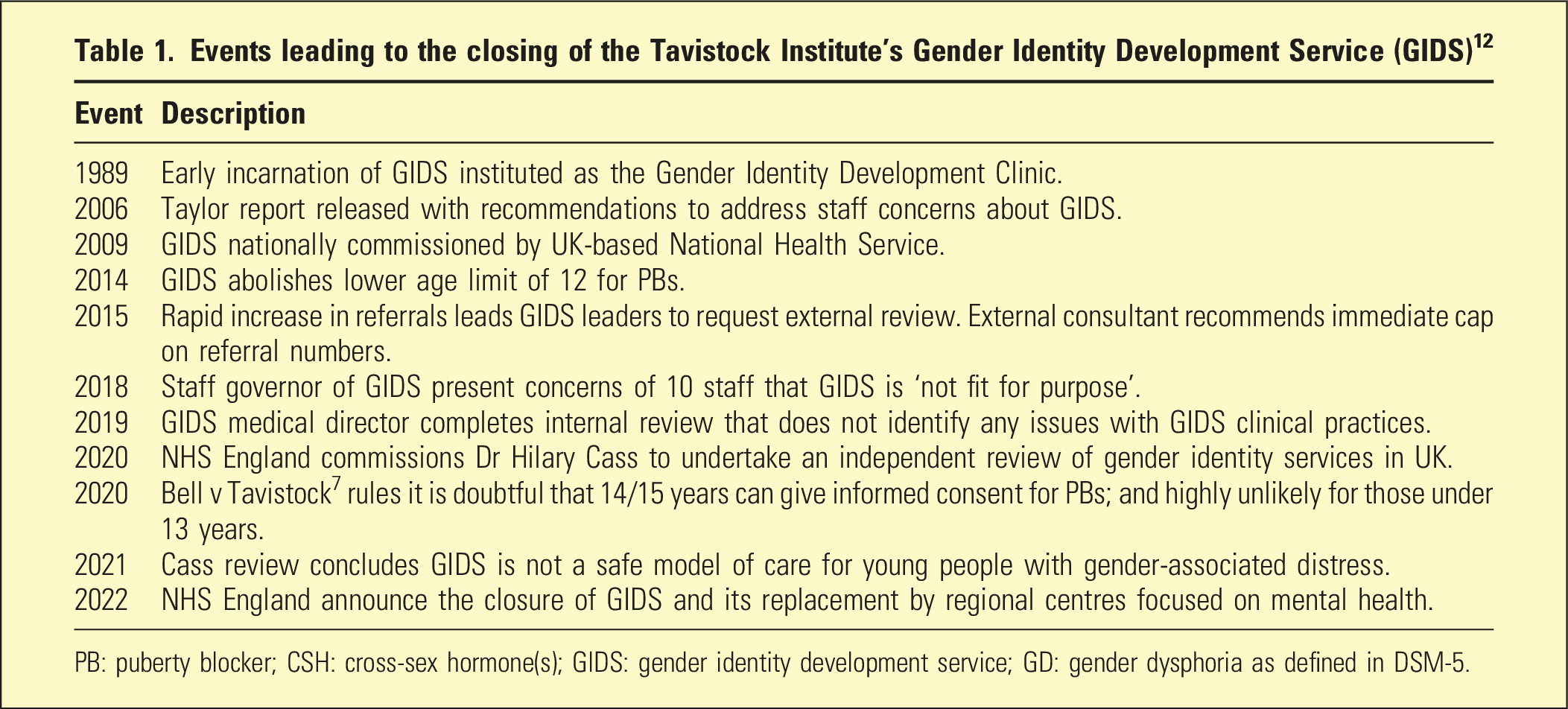
The clinical, social, and political understanding of sex and gender is vigorously contested. The closure of the Tavistock’s Gender Identity Development Service (GIDS), announced in 2022 after staff and an independent review questioned the safety of gender affirming care for gender dysphoria, highlight this (Table 1). Additionally, the DSM-5 (2013) and ICD-11 (2022) updated categories associated with gender phenomenology: DSM-5 replaced ‘gender identity disorder’ with ‘gender dysphoria’1; ICD-11 replaced the diagnoses ‘transsexualism’ and ‘gender identity disorder of children’ with the codes ‘gender incongruence of adolescence and adulthood’ and ‘childhood’.2,3 While the DSM-5 diagnosis is predicated on individual distress caused by gender experiences, the ICD-11 codes attribute distress or dysfunction associated with gender experiences to social stigma.4
Events leading to the closing of the Tavistock Institute’s Gender Identity Development Service (GIDS)12
Event
Description
1989
Early incarnation of GIDS instituted as the Gender Identity Development Clinic.
2006
Taylor report released with recommendations to address staff concerns about GIDS.
2009
GIDS nationally commissioned by UK-based National Health Service.
2014
GIDS abolishes lower age limit of 12 for PBs.
2015
Rapid increase in referrals leads GIDS leaders to request external review. External consultant recommends immediate cap on referral numbers.
2018
Staff governor of GIDS present concerns of 10 staff that GIDS is ‘not fit for purpose’.
2019
GIDS medical director completes internal review that does not identify any issues with GIDS clinical practices.
2020
NHS England commissions Dr Hilary Cass to undertake an independent review of gender identity services in UK.
2020
Bell v Tavistock7 rules it is doubtful that 14/15 years can give informed consent for PBs; and highly unlikely for those under 13 years.
2021
Cass review concludes GIDS is not a safe model of care for young people with gender-associated distress.
2022
NHS England announce the closure of GIDS and its replacement by regional centres focused on mental health.
PB: puberty blocker; CSH: cross-sex hormone(s); GIDS: gender identity development service; GD: gender dysphoria as defined in DSM-5.
In effect, the ICD approach removes the locus of disease from the individual and diagnoses a ‘diseased society’ where healthy individuals’ distress arises from pathological power relationships. This divergence is worthy of detailed examination as a prima facie example of the prioritisation of political over clinical goals. However, as our discussion concerns ethical, medico-legal, and iatrogenic issues in cases arising in the UK, we consider gender dysphoria alone.
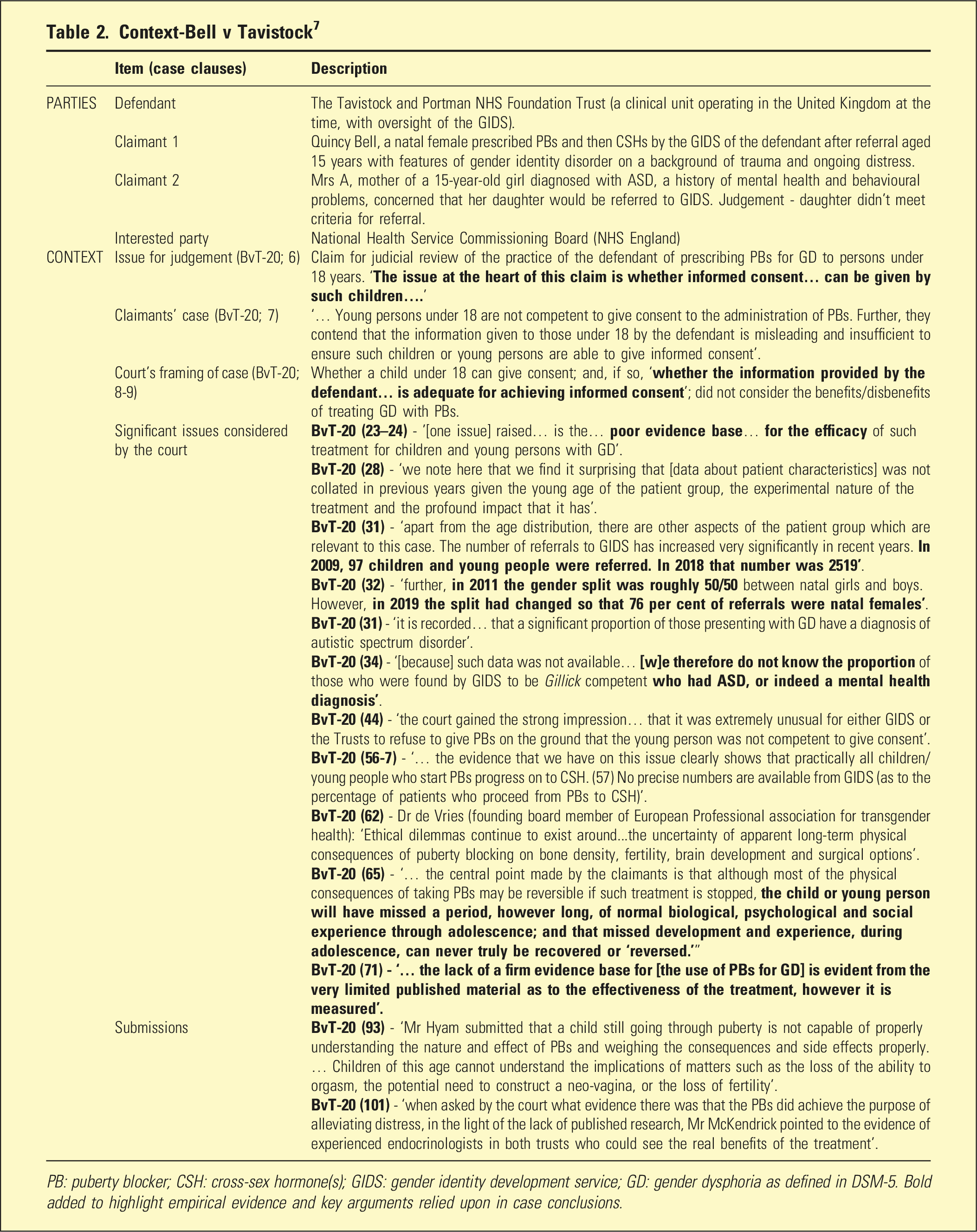
These nosological changes paralleled rapid changes in gender associated presentations in the UK and elsewhere, albeit the epidemiological evidence base is limited. The best available international evidence suggests an overall increase in presentations with gender dysphoria under 18 years old, with a disproportionate increase in natal female presentations.5,6Table 2, which summarises the legal case discussed below, confirms both increased referrals and increased proportion of natal females at GIDS 2009–2019.7 The available evidence cannot explain increased presentations/female predominance,6 but proposed causes include the influence of movements promoting individual rights,8 and/or decreased stigma with increased service availability.4
The Tavistock and Portman NHS Foundation Trust (a clinical unit operating in the United Kingdom at the time, with oversight of the GIDS).
Claimant 1
Quincy Bell, a natal female prescribed PBs and then CSHs by the GIDS of the defendant after referral aged 15 years with features of gender identity disorder on a background of trauma and ongoing distress.
Claimant 2
Mrs A, mother of a 15-year-old girl diagnosed with ASD, a history of mental health and behavioural problems, concerned that her daughter would be referred to GIDS. Judgement - daughter didn’t meet criteria for referral.
Interested party
National Health Service Commissioning Board (NHS England)
CONTEXT
Issue for judgement (BvT-20; 6)
Claim for judicial review of the practice of the defendant of prescribing PBs for GD to persons under 18 years. ‘The issue at the heart of this claim is whether informed consent… can be given by such children….’
Claimants’ case (BvT-20; 7)
‘… Young persons under 18 are not competent to give consent to the administration of PBs. Further, they contend that the information given to those under 18 by the defendant is misleading and insufficient to ensure such children or young persons are able to give informed consent’.
Court’s framing of case (BvT-20; 8-9)
Whether a child under 18 can give consent; and, if so, ‘whether the information provided by the defendant… is adequate for achieving informed consent’; did not consider the benefits/disbenefits of treating GD with PBs.
Significant issues considered by the court
BvT-20 (23–24) - ’[one issue] raised… is the… poor evidence base… for the efficacy of such treatment for children and young persons with GD’. BvT-20 (28) - ‘we note here that we find it surprising that [data about patient characteristics] was not collated in previous years given the young age of the patient group, the experimental nature of the treatment and the profound impact that it has’. BvT-20 (31) - ‘apart from the age distribution, there are other aspects of the patient group which are relevant to this case. The number of referrals to GIDS has increased very significantly in recent years. In 2009, 97 children and young people were referred. In 2018 that number was 2519’. BvT-20 (32) - ‘further, in 2011 the gender split was roughly 50/50 between natal girls and boys. However, in 2019 the split had changed so that 76 per cent of referrals were natal females’. BvT-20 (31) - ‘it is recorded… that a significant proportion of those presenting with GD have a diagnosis of autistic spectrum disorder’. BvT-20 (34) - ‘[because] such data was not available… [w]e therefore do not know the proportion of those who were found by GIDS to be Gillick competent who had ASD, or indeed a mental health diagnosis’. BvT-20 (44) - ‘the court gained the strong impression… that it was extremely unusual for either GIDS or the Trusts to refuse to give PBs on the ground that the young person was not competent to give consent’. BvT-20 (56-7) - ‘… the evidence that we have on this issue clearly shows that practically all children/young people who start PBs progress on to CSH. (57) No precise numbers are available from GIDS (as to the percentage of patients who proceed from PBs to CSH)’. BvT-20 (62) - Dr de Vries (founding board member of European Professional association for transgender health): ‘Ethical dilemmas continue to exist around...the uncertainty of apparent long-term physical consequences of puberty blocking on bone density, fertility, brain development and surgical options’. BvT-20 (65) - ‘… the central point made by the claimants is that although most of the physical consequences of taking PBs may be reversible if such treatment is stopped, the child or young person will have missed a period, however long, of normal biological, psychological and social experience through adolescence; and that missed development and experience, during adolescence, can never truly be recovered or ‘reversed.’” BvT-20 (71) - ‘… the lack of a firm evidence base for [the use of PBs for GD] is evident from the very limited published material as to the effectiveness of the treatment, however it is measured’.
Submissions
BvT-20 (93) - ‘Mr Hyam submitted that a child still going through puberty is not capable of properly understanding the nature and effect of PBs and weighing the consequences and side effects properly. … Children of this age cannot understand the implications of matters such as the loss of the ability to orgasm, the potential need to construct a neo-vagina, or the loss of fertility’.
BvT-20 (101) - ‘when asked by the court what evidence there was that the PBs did achieve the purpose of alleviating distress, in the light of the lack of published research, Mr McKendrick pointed to the evidence of experienced endocrinologists in both trusts who could see the real benefits of the treatment’.
PB: puberty blocker; CSH: cross-sex hormone(s); GIDS: gender identity development service; GD: gender dysphoria as defined in DSM-5. Bold added to highlight empirical evidence and key arguments relied upon in case conclusions.
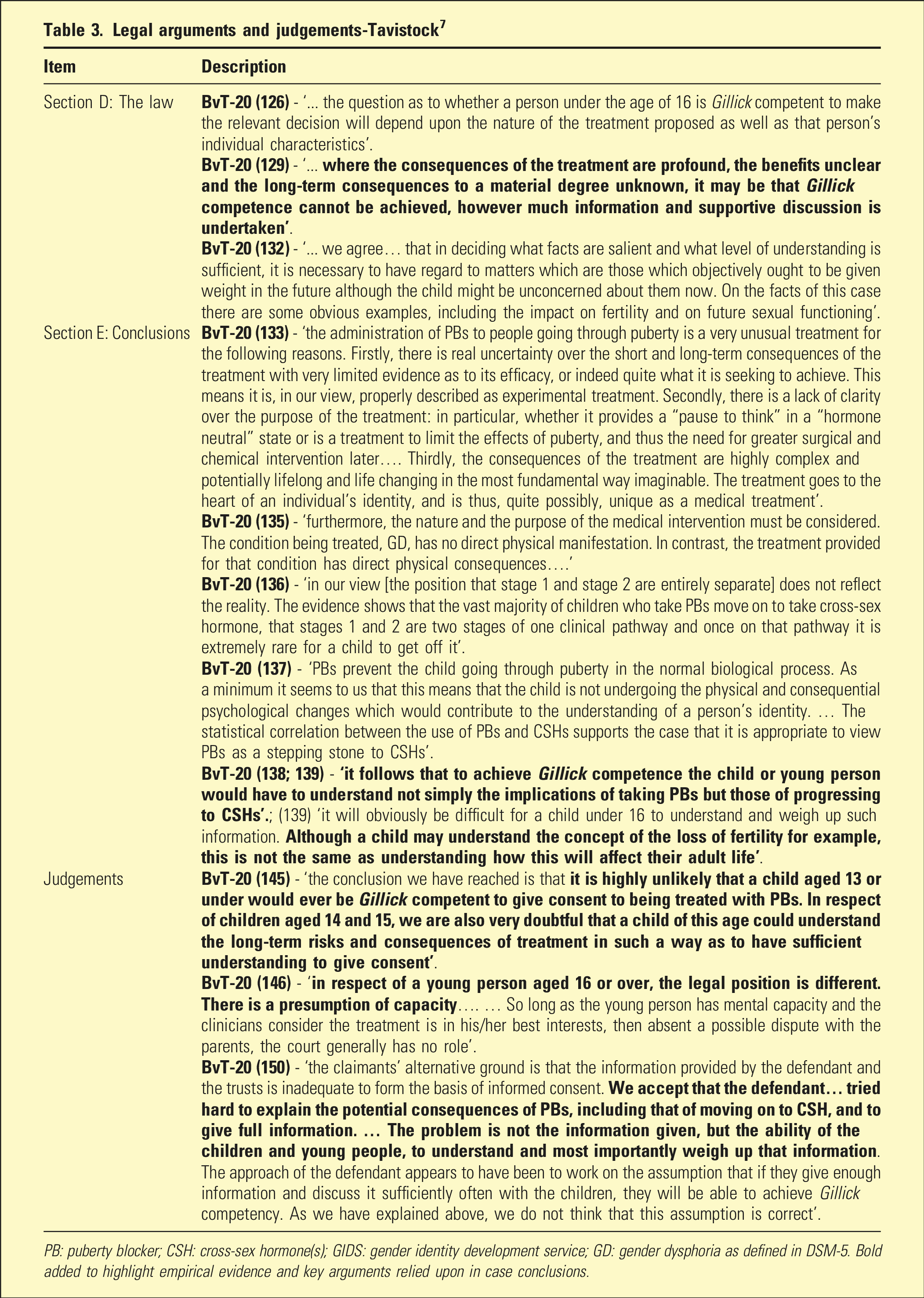
Comprehensive treatment of gender dysphoria relies on in-depth individual and family interviews including exploration of childhood adversity and trauma and comprehensive formulation with differential diagnosis and treatment options.9,10 In contrast, the Tavistock model of gender affirming care described in rulings by the UK’s High Court7 and Appeals Court11 appears to have relied upon unwarranted assumptions about the efficacy of treatment, lack of significant side effects, and capacity of young children to understand complex information (Tables 2 and 3).
BvT-20 (126) - ‘... the question as to whether a person under the age of 16 is Gillick competent to make the relevant decision will depend upon the nature of the treatment proposed as well as that person’s individual characteristics’. BvT-20 (129) - ‘... where the consequences of the treatment are profound, the benefits unclear and the long-term consequences to a material degree unknown, it may be that Gillick competence cannot be achieved, however much information and supportive discussion is undertaken’. BvT-20 (132) - ‘... we agree… that in deciding what facts are salient and what level of understanding is sufficient, it is necessary to have regard to matters which are those which objectively ought to be given weight in the future although the child might be unconcerned about them now. On the facts of this case there are some obvious examples, including the impact on fertility and on future sexual functioning’.
Section E: Conclusions
BvT-20 (133) - ‘the administration of PBs to people going through puberty is a very unusual treatment for the following reasons. Firstly, there is real uncertainty over the short and long-term consequences of the treatment with very limited evidence as to its efficacy, or indeed quite what it is seeking to achieve. This means it is, in our view, properly described as experimental treatment. Secondly, there is a lack of clarity over the purpose of the treatment: in particular, whether it provides a “pause to think” in a “hormone neutral” state or is a treatment to limit the effects of puberty, and thus the need for greater surgical and chemical intervention later…. Thirdly, the consequences of the treatment are highly complex and potentially lifelong and life changing in the most fundamental way imaginable. The treatment goes to the heart of an individual’s identity, and is thus, quite possibly, unique as a medical treatment’. BvT-20 (135) - ‘furthermore, the nature and the purpose of the medical intervention must be considered. The condition being treated, GD, has no direct physical manifestation. In contrast, the treatment provided for that condition has direct physical consequences….’ BvT-20 (136) - ‘in our view [the position that stage 1 and stage 2 are entirely separate] does not reflect the reality. The evidence shows that the vast majority of children who take PBs move on to take cross-sex hormone, that stages 1 and 2 are two stages of one clinical pathway and once on that pathway it is extremely rare for a child to get off it’. BvT-20 (137) - ‘PBs prevent the child going through puberty in the normal biological process. As a minimum it seems to us that this means that the child is not undergoing the physical and consequential psychological changes which would contribute to the understanding of a person’s identity. … The statistical correlation between the use of PBs and CSHs supports the case that it is appropriate to view PBs as a stepping stone to CSHs’. BvT-20 (138; 139) - ‘it follows that to achieve Gillick competence the child or young person would have to understand not simply the implications of taking PBs but those of progressing to CSHs’.; (139) ‘it will obviously be difficult for a child under 16 to understand and weigh up such information. Although a child may understand the concept of the loss of fertility for example, this is not the same as understanding how this will affect their adult life’.
Judgements
BvT-20 (145) - ‘the conclusion we have reached is that it is highly unlikely that a child aged 13 or under would ever be Gillick competent to give consent to being treated with PBs. In respect of children aged 14 and 15, we are also very doubtful that a child of this age could understand the long-term risks and consequences of treatment in such a way as to have sufficient understanding to give consent’. BvT-20 (146) - ‘in respect of a young person aged 16 or over, the legal position is different. There is a presumption of capacity…. … So long as the young person has mental capacity and the clinicians consider the treatment is in his/her best interests, then absent a possible dispute with the parents, the court generally has no role’. BvT-20 (150) - ‘the claimants’ alternative ground is that the information provided by the defendant and the trusts is inadequate to form the basis of informed consent. We accept that the defendant… tried hard to explain the potential consequences of PBs, including that of moving on to CSH, and to give full information. … The problem is not the information given, but the ability of the children and young people, to understand and most importantly weigh up that information. The approach of the defendant appears to have been to work on the assumption that if they give enough information and discuss it sufficiently often with the children, they will be able to achieve Gillick competency. As we have explained above, we do not think that this assumption is correct’.
PB: puberty blocker; CSH: cross-sex hormone(s); GIDS: gender identity development service; GD: gender dysphoria as defined in DSM-5. Bold added to highlight empirical evidence and key arguments relied upon in case conclusions.
The independent Cass review5 confirmed the limited evidence base for gender affirming care, concerns with systematic and protocol issues as practised at gender clinics, and attendant risks of iatrogenic morbidity for vulnerable adolescents and their families. Hannah Barnes’ narrative account of the collapse of the GIDS identifies the influence of activist organisations such as Mermaids on the evolution of clinical practices, especially treatment selection and protocols: “… over time, Mermaids became more political and harder to work with. Their position appeared to be that there was only one outcome for these children and young people - medical transition.” (p. 32).12
We consider Tavistock GIDS’ closure as tacit acknowledgement the gender affirming model was influenced by non-clinical activists with greater understanding of, and interest in, political and social progress than individual patient care. We find supportive evidence of this influence in the affirming care suffered by Keira Bell at the Tavistock and documented in the High Court case Bell v Tavistock7 (Tables 2 and 3).
While the Court focused on ‘informed consent’, the case also reveals assumptions, clinical practices, and standards of evidence accepted by the Tavistock. We view Bell v Tavistock7 as a cautionary tale of the dangers of allowing activist groups like Mermaids to influence models of care over the objections of clinical staff (Table 3).
Gender affirming care assumes that emotionally distressed minors expressing gender dysphoria have such a degree of certainty in their self-experience that it is potentially life-threatening to explore the stability of their experience.4,8,13 Bell7 and Barnes’ book12 show how pressure by activists like Mermaids can prevent necessary clinical exploration of a patient’s stated desire to ‘transition’. This approach has persisted despite evidence that a significant proportion of young people reporting gender dysphoria later accept their birth gender. In many cases, greater tolerance of natal sex is accompanied by acceptance of same-sex attraction.14
The natural history of gender dysphoria suggests two critical ethical questions: first, is the ‘transition pathway’ – social, medical or surgical – in the best interest of the child? and second, is that pathway consistent with the principle ‘first, do no harm’?
There is no compelling evidence that affirmation decreases the risk of suicide.15 The dilemma in which distressed parents are challenged to imagine choosing between a dead child and a trans-child16 appears to use parents’ caring instinct and trust in experts’ knowledge/ethics to force them to suppress the impulse to question any aspect of gender affirming care. Parents are the primary source of feedback and support for minors.17 This cooption of their role in clinical decision-making may be the most potent factor in gender affirming care, by preventing exploration of potential positives of sex-congruent gender identity; or potential negatives of sex-incongruent identity contrary.
The first author has been treating suicidal young people for over 40 years, including children under the age of 10. Effective treatment accommodating children’s often unfixed concept of death is among the most complex clinical challenges in psychiatric practice. Clearly, clinical presentations including suicidality demand assessment of intent, planning, lethality, history of attempts, treatment and outcome(s), co-morbid conditions, and inter alia. The claim that exploring identity is likely to lead to suicide seems to us grossly unprofessional.16
The gender affirming care described in the Bell case included little in-depth examination of mental life/living, reasons underlying her adolescent decision to transition, or the re-evaluation leading to de-transition in her early twenties. In particular, follow-up and monitoring for social, medical, and surgical side-effects/complications of transition seemed limited. For some clinicians, discussion of the significant number of patients who have detransitioned after gender affirming care remains out of bounds, despite detransitioners’ credibility as witnesses with lived experience of the affirmation model.12
Lessons and warnings
The UK’s High Court7 found most minors lack the Gillick competence to make life-altering decisions as it is impossible for them to understand a priori the realities of sexual development. The substitution of gender affirming for evidence-based care at the prestigious Tavistock raises issues of clinical governance, the influence of activist groups on ethical oversight, and the potential for iatrogenic harm. The published cases highlight limitations in the Tavistock’s governance of clinical processes found to have directly contributed to harms sustained by Keira Bell. Nonetheless, it is encouraging that research is gradually improving understanding of gender affirming care. Kozlowska et al.18 provide clinicians with evidence of gender dysphoria’s complex diagnostic profile to provide informed consent before embarking on life-changing intervention.
Locally, we have been troubled by the suspension of a senior child psychiatrist from a major Australian children’s hospital after expressing concern the hospital’s gender affirming model was neither supported by evidence nor consistent with best practice.5 The suspension reportedly came after the complaint of a single patient distressed by the psychiatrist’s public expression of potential risks associated with gender affirming care.19 Based on public information, the psychiatrist appears to have been punished for accurate information about an area of active international concern.
Conclusions
In our opinion, the Bell case documents harms directly arising from the subordination of clinical governance to social and political goals and promoted by poor governance of the boundaries between clinical units like the GIDS and activist organisations like Mermaids, well-documented by Barnes12 and the Cass Review.5 We believe that advocates for those experiencing gender dysphoria want them to receive the best care. However, the Tavistock case shows this drive has risked patients’ health and family wellbeing on clinical frameworks unbacked by evidence. As the Cass Review makes clear, the certainty associated with gender affirming care is not backed by any strong evidence about the natural history of gender dysphoria or the efficacy/sequelae of the treatment alternatives, particularly over the long term.
We are aware of growing efforts to provide better empirical foundations for the detection, diagnosis, and ethical treatment of patients with gender dysphoria. We also believe that clinicians caring for this group of patients will continue to be subject to strong political and social influences for the foreseeable future. Given the widespread failures of the last few years, psychiatrists treating patients with gender dysphoria must ground their practice in evidence; recognise, understand, and keep separate the clinical, social, and political issues associated with gender dysphoria; and provide leadership to patients, parents, and other health workers attempting to navigate these deep and troubled waters.
Footnotes
Declaration of conflicting interests
The Authors declare that there were no conflicts of interest to report and no ethics approval was required for this paper. The first author is on the Editorial Committee and the second author is Deputy Editor of Australasian Psychiatry.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
George Halasz
Andrew Amos
References
1.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed.Washington, DC: American Psychiatric Association, 2013.
2.
World Health Organization. ICD-11: international classification of diseases. 11th ed.Geneva, Switzerland: World Health Organization, 2022. (11th revision) [Internet]. [cited 2023 Jul 17]. Available from: https://icd.who.int/en
ColemanERadixAEBoumanWP, et al.Standards of care for the health of transgender and gender diverse people, version 8. Int J Transgend Health2022; 23(Suppl 1): S1–259.
ClaytonA. Gender-affirming treatment of gender dysphoria in youth: a perfect storm environment for the placebo effect—the implications for research and clinical practice. Archives of Sexual Behavior2023; 52: 483–494.
9.
FrewTWatsfordCWalkerI. Gender dysphoria and psychiatric comorbidities in childhood: a systematic review. Aust J Psychol2021; 73(3): 255–271.
10.
ByneWBradleySColemanE, et al.Report of the APA task force on treatment of gender identity disorder. Am J Psychiatr2012; 169(8): 1–35.
BarnesH. Time to think: the inside story of the collapse of the Tavistock’s gender service for children. La Hulpe, Belgium: Swift Press, 2023.
13.
The Lancet Child & Adolescent Health. A flawed agenda for trans youth. Lancet Child Adolesc Health2021; 5: 385.
14.
LittmanL. Individuals treated for gender dysphoria with medical and/or surgical transition who subsequently detransitioned: a survey of 100 detransitioners. Arch Sex Behav2021; 50(8): 3353–3369.
15.
JacksonD. Suicide-related outcomes following gender-affirming treatment: a review. Cureus2023; 15: e36425.
16.
AyadSRobertoLDDianna KennyM, et al.A clinical guide for therapists working with gender-questioning youth. Oslo, Norway: GETA, 2022.
17.
VrouenraetsLJde VriesALCArnoldussenM, et al.Medical decision-making competence regarding puberty suppression: perceptions of transgender adolescents, their parents and clinicians. Eur Child Adolesc Psychiatr2023; 32: 2343–2361. (Online before print).
18.
KozlowskaKChudleighCMcClureG, et al.Attachment patterns in children and adolescents with gender dysphoria. Front Psychol2021; 11: 582688.