
Abstract

Dear Editor,
Methodological issues in the Coulston and Leahy paper. a
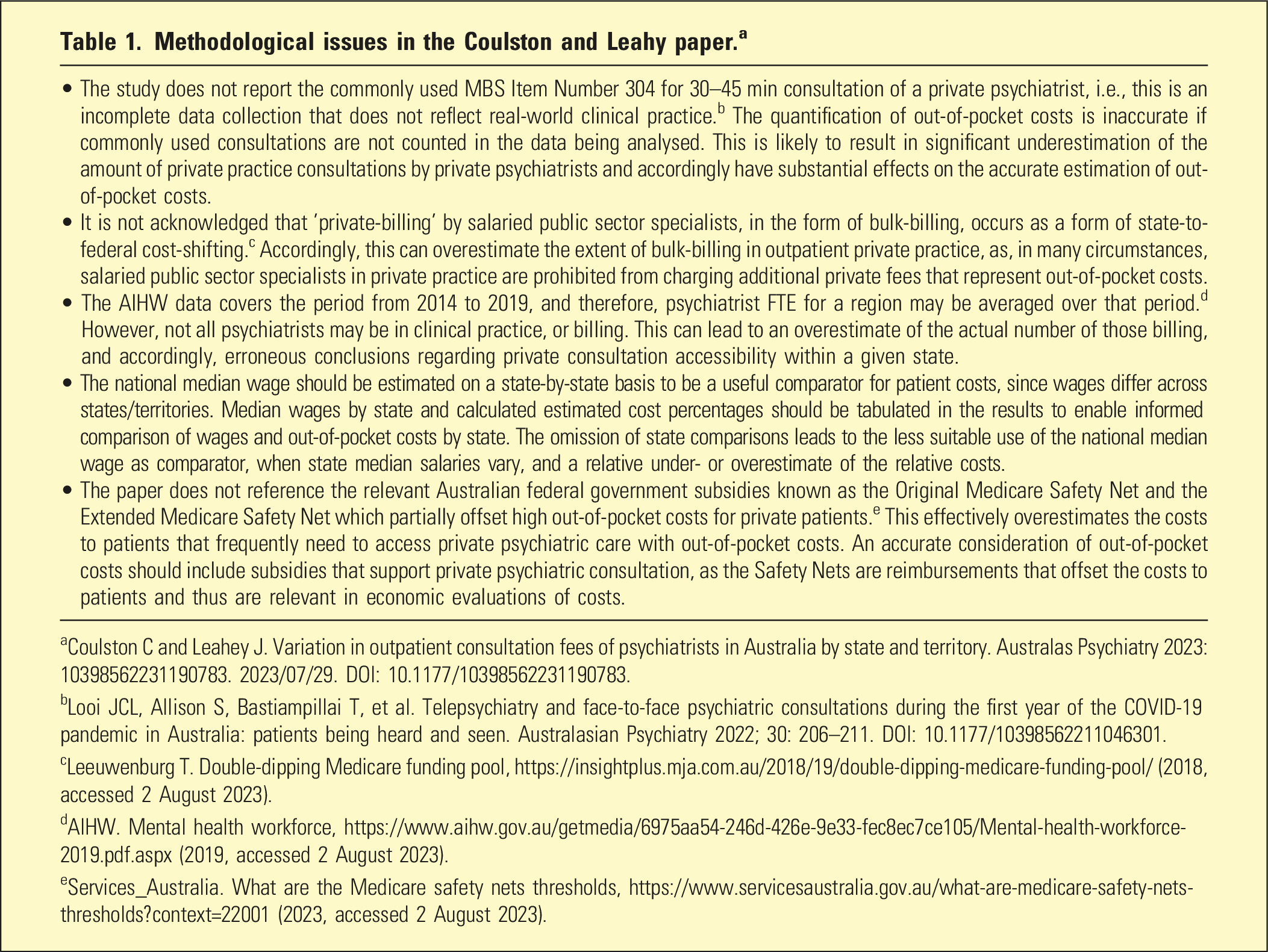
aCoulston C and Leahey J. Variation in outpatient consultation fees of psychiatrists in Australia by state and territory. Australas Psychiatry 2023: 10398562231190783. 2023/07/29. DOI: 10.1177/10398562231190783.
bLooi JCL, Allison S, Bastiampillai T, et al. Telepsychiatry and face-to-face psychiatric consultations during the first year of the COVID-19 pandemic in Australia: patients being heard and seen. Australasian Psychiatry 2022; 30: 206–211. DOI: 10.1177/10398562211046301.
cLeeuwenburg T. Double-dipping Medicare funding pool, https://insightplus.mja.com.au/2018/19/double-dipping-medicare-funding-pool/ (2018, accessed 2 August 2023).
dAIHW. Mental health workforce, https://www.aihw.gov.au/getmedia/6975aa54-246d-426e-9e33-fec8ec7ce105/Mental-health-workforce-2019.pdf.aspx (2019, accessed 2 August 2023).
eServices_Australia. What are the Medicare safety nets thresholds, https://www.servicesaustralia.gov.au/what-are-medicare-safety-nets-thresholds?context=22001 (2023, accessed 2 August 2023).
The usual practice in interpretation and discussion of research studies is to begin from the findings of the study. As listed in Table 1, there are methodological issues that raise questions as to the completeness and accuracy of the data collection and analysis. However, these methodological issues, which constitute limitations of the paper, have not been acknowledged. Consequently, the validity of the findings remains questionable.
In this context, the arguments that are expressed in the discussion do not necessarily have a foundation in valid study findings. In addition, the usual practice is that explanation and discussion of the findings should, at least initially, be based on the data in that study, before exploration of proposed actions or further research. There appears to be a conflation between interpretations and proposed actions in this paper.
Specifically, the discussion of Private Health Insurance (PHI) extension to outpatient care is not based on the findings of the study and in this context is substantively non sequitur, for example, ‘…Freed and Allen suggested that the Australian Government’s rule preventing health insurers from covering outpatient consultations had failed to prevent increases in fees…' 1 and ‘Allowing health insurers to subsidize outpatient psychiatric consultations would improve access for the 45.2% of Australians who hold private health insurance'. 1 These statements imply that the PHI market can address out-of-pocket costs and propose action which is not supported by the findings of the study, which does not involve research into why and how out-of-pocket costs are addressed to improve equitable access to care. Furthermore, US-style PHI managed care initiatives that encompass outpatient care have not demonstrated efficacy and have instead limited clinical and patient autonomy regarding choice of and access to care. 2
A recent comprehensive health economic analysis of out-of-pocket healthcare costs for Australians observed that there was a linear relationship between costs and healthcare access by patients, that is, the higher the cost, the less patients accessed care. 3 However, this paper noted that there needs to be broader consideration of the healthcare ecological context to develop equitable accessibility, and this may include improving access to out-of-pocket cost subsidies such as the Medicare Safety Net and Pharmaceutical Benefits Schedule. 3
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.