
Abstract
Objective
This paper updates clinicians and service leaders on evidence bases relevant to rehabilitation for older Australians with mental illness.
Methods
Narrative review of literature and relevant public domain data supported by reflections on NSW service development.
Results
There is a paucity of high-quality evidence regarding mental health rehabilitation in older people. Available evidence supports integrating lessons from physical healthcare with adaptations of ‘adult’ mental health rehabilitation. Adaptation is required to respond to the specific needs, strengths and service use of older people with mental illness. Challenges for older people include ageism, increased physical and cognitive comorbidities, lower access to mental health services and earlier residential aged care entry. Strengths of older people include an ongoing desire for recovery, ongoing developmental change and often closer connections with carers and GPs. Evidence is consistent with evaluation of relevant NSW service models and initiatives including the Pathways to Community Living Initiative. Integration of recovery-oriented practice and wellness models may provide a framework for future innovative inpatient and community-based models.
Conclusions
There is sufficient evidence to guide development of models of rehabilitation with older people, but innovation and evaluation are essential if older people are to have equal opportunities in their recovery journeys.
Older people with severe or complex mental illness have needs related to both ageing and mental ill-health. Unclear service responsibilities 1 and poor access to services designed for their specific needs impede opportunities for recovery and contribute to early entry to residential aged care internationally. 2
This paper aims to assist clinicians and service leaders to improve the lives and outcomes of older Australians with mental illness by reviewing evidence bases available to guide their rehabilitation. It goes on to propose an initial framework and questions to assist local decision-making and service development.
Rehabilitation has been defined as ‘a set of interventions designed to optimize functioning and reduce disability in individuals with health conditions in interaction with their environment’ 3 occurring ‘during all phases of acute, sub-acute and long-term care’. 3 However, mental health rehabilitation guidance focuses on individuals with well-established severe or complex psychotic illness,4,5 without describing adaptation for older people. This begs the question ‘What does being older mean for individuals who may benefit from mental health rehabilitation?’
Methods
This article has used this question to guide a narrative review of literature, analysis of public domain data sets, and reflections on service models, evaluations and experience within NSW older people’s mental health (OPMH) services. The literature review utilized Google Scholar, commencing with key terms ‘rehabilitation’, ‘mental health’ and ‘elderly’, ‘geriatric’ OR ‘older’. Articles were selected for review based on abstracts, with citations used to identify further sources.
Results
Evidence bases to inform adaptation of adult rehabilitation guidance
Recovery and older people
Older people with mental illness experience ongoing changes in needs and strengths, with a continuing desire for recovery,
6
including in the presence of dementia.
7
Older people with mental illness have described recovery as ‘continuing to be me’,
6
with three distinctive aspects: • an established and enduring sense of identity; • using strategies to enhance continuity and reinforce identity and • managing impacts of coexisting physical illness.
6
Practice implications include actions to maintain identity through supporting long-term friendships, social networks and established roles. Supporting families and carers to help maintain a person’s identity over time is particularly important for people with dementia. Innovative methods for co-design with older people, 8 age-relevant peer work 9 and systemic changes of service orientation 10 are emerging. A statewide recovery-oriented practice project focused on older people with mental illness 11 identified strategies to support empowerment, agency and self-management as fundamental. This was enabled through age-relevant peer work, recovery/wellness programs, collaborative care planning incorporating recovery goals and wellness planning.
Application of wellness models to older people with mental illness 12 has added the concept of ‘developmental wellness’ to existing models. The other wellness dimensions are similar to the domains of a meaningful life fundamental to ‘personal recovery’ for older people with mental illness. 13
Rehabilitation needs of older people with mental illness
‘Developmental wellness’ relates to an individual’s responses to ageing. It includes lifestyle factors, subjective experience of ageing and the ‘early aging’ and disability that may be experienced by people with severe mental illness. Such early aging occurs with lifelong experiences of stigma, psychiatric medication, lengthy and/or recurrent hospitalizations and managing multiple mental health and health conditions.
What do we know about strengths and needs? Proportion of inpatients identified with either clinically significant or severe/very severe problems on HoNOS or HoNOS65+ at a 91-day review
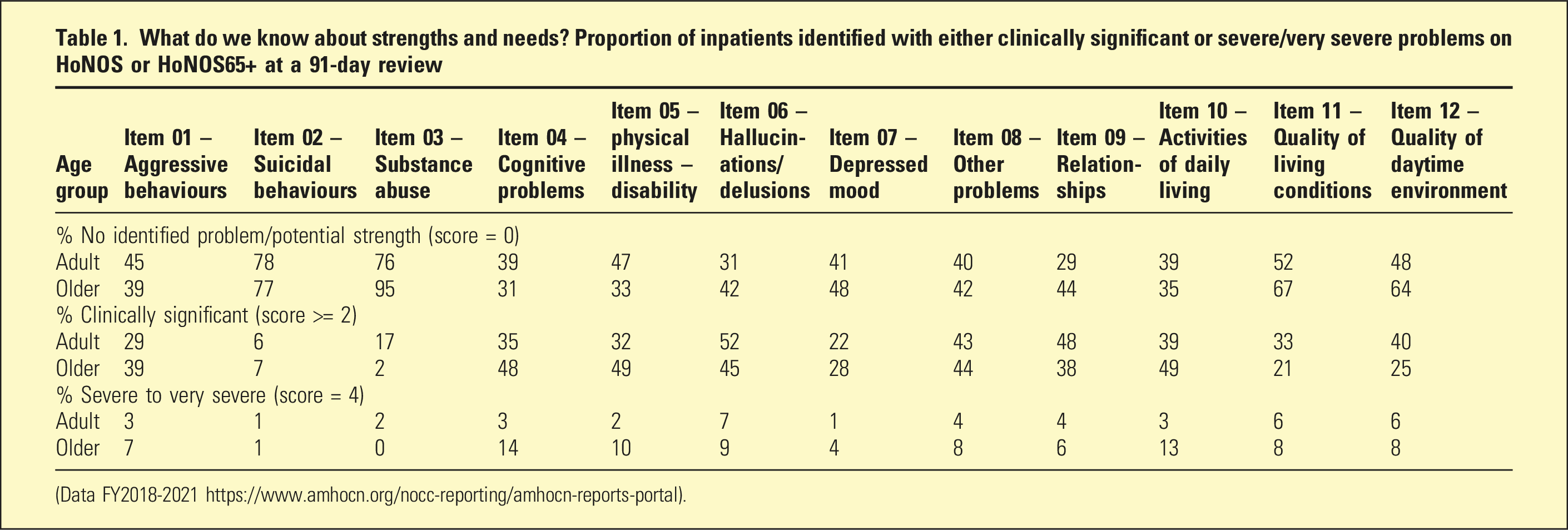
(Data FY2018-2021 https://www.amhocn.org/nocc-reporting/amhocn-reports-portal).
Proportion of older people at a 91-day review requiring assistance as measured on resource utilization group activities of daily living (RUG_ADL)
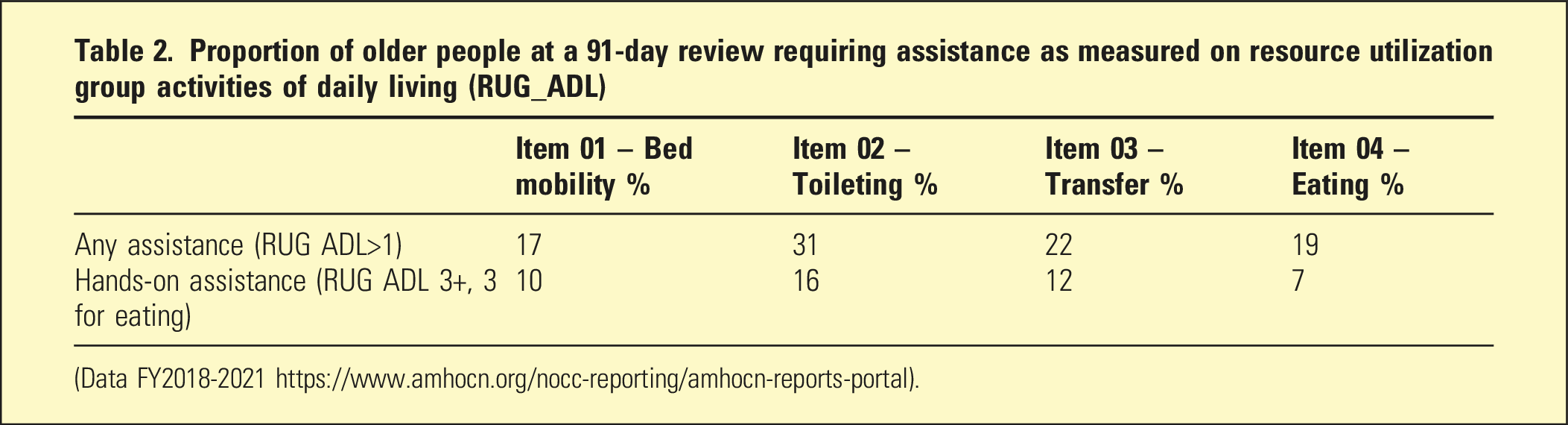
(Data FY2018-2021 https://www.amhocn.org/nocc-reporting/amhocn-reports-portal).
National data reported at https://www.aihw.gov.au/mental-health suggests limitations in older people’s access to mental health care and support to promote recovery. Older people have very limited access to psychosocial support services, specialist homelessness services or mental health residential care services. As people age above 65 years, they have steeply declining access to Medicare-funded mental health services, and markedly increased likelihood of experiencing mental health admissions without recorded specialized mental health care.
Mental health rehabilitation guidance specific to older people
The only relevant systematic review regarding mental health rehabilitation in older people concluded evidence was insufficient to make recommendations for an older population. 14 Studies are almost all community-based, small in size, inclusive of ‘middle-aged’ people and without analysis of impacts of age. 14 However, innovative pilots have shown promise, and the largest randomized control trial with age impact analysis 15 demonstrated no decline in outcomes with age. This study of integrated community physical health care, social interventions and mental health care had a mean age of 60 years and diagnostic profile (45% mood disorders) similar to relevant Australian services. Published studies highlight the importance of social reintegration 16 in older people regaining optimal functioning, and of neglected wellness domains in trials involving older people. 17
Physical health rehabilitation guidance
While a review is outside the article scope, guidance on rehabilitation related to physical illness, such as impaired mobility, hip fracture or heart attack may all be relevant for some older people with complex mental illness. Of particular note is the importance placed on early rehabilitation, 18 prior to deconditioning.
Reflections on NSW service models
Variability in service models and responsibilities is a prominent impediment to Australian service development. 1 Reviewing the evidence base for rehabilitation for older people with mental illness highlights the importance of the ‘phases of care’ concept underpinning mental health activity-based funding (ABF) in Australia. 19 ABF links funding to the purpose of care rather than the name or nature of the team providing it. Mental health rehabilitation can, and in the case of older people probably does, occur outside designated ‘non-acute’ or rehabilitation services. This may complicate interpretations of the National Mental Health Services Planning Framework (https://www.aihw.gov.au/nmhspf).
Within NSW there has been progressive development of a range of older people’s mental health (OPMH) services. 20 ‘Rehabilitation’ is not clearly articulated in NSW OPMH policy frameworks 20 or models of care,13,21 but NSW OPMH guidance emphasizes the distinctive and individual nature of older people’s recovery journeys, the multiple dimensions of recovery and the multiple partnerships required to support recovery and wellness for older people with mental illness. Consultation with older people has highlighted they frequently have complex systems supporting their recovery that are often unfamiliar to adult mental health services, with varied philosophies and regulatory frameworks. Mental health services are only one element of support, required at different intensities over time.
Evidence from consultations, models of care and evaluations in NSW provides some guidance to support key directions in rehabilitation and recovery-oriented practice with older people with mental illness across settings. All emphasize: • multidisciplinary care; • individualized, recovery-oriented approaches; • being inclusive of consumers with a broad range of diagnoses (most notably schizophrenia, depressive disorders, dementia-related disorders and bipolar disorder) and comorbidities and • actively developing methods to enable genuine input from older people.
The NSW OPMH community model of care 13 emphasizes the importance of bringing OPMH clinical expertise to partnerships with other services. The NSW OPMH acute inpatient unit model of care 21 raises the question of whether early rehabilitation interventions should be, or are already, occurring in acute OPMH units (with a 40-day average length of stay). Elements of the model of care 21 are consistent with this, but greater emphasis on rehabilitation functions may be warranted, particularly in reducing risks related to deconditioning or medication side effects. The non-acute Transitional Assessment and Intervention Service inpatient model extends the concept of rehabilitation to older people with very severe behavioural and psychological symptoms of dementia. 22
In NSW, specialized mental health residential aged care partnership services are an important part of the spectrum of care. Evaluation of the NSW Pathways to Community Living Initiative
23
identified important elements of these services including: • early discharge planning in inpatient settings for entry into specialized residential aged care services to reduce hospital stays; • person-centred, individualized assessment, transition planning and care; • embedding of recovery orientation within routine practice; • working with a person’s strengths, capacities and preferences and • follow-up care from specialist OPMH clinicians.
Findings are explored in more depth in the evaluation report. The PCLI outcome and assessment tools may provide a good basis for the development of specialized older people’s mental health rehabilitation services. Their starting point of understanding a person’s desired setting for future care, rather than what settings are most available is pertinent.
Discussion
Guidance for adults with psychosis provides an important evidence base and reference point for mental health rehabilitation with older people and will be directly applicable to some older people. However, this guidance is insufficient in scope for many older people with mental illness. Moreover, such guidance does not easily facilitate communication and integration of care with non-mental health services that older people with mental illness may need to access to support rehabilitation.
An individualized approach to rehabilitation appears appropriate to meet the current needs of older people with complex mental illness. Figure 1 captures key elements, including the need to support individually prioritized dimensions of wellness and domains of a meaningful life. This approach has potential to integrate aspects of physical healthcare models with adaptations of general adult mental health rehabilitation models. Framework for mental health rehabilitation with older people.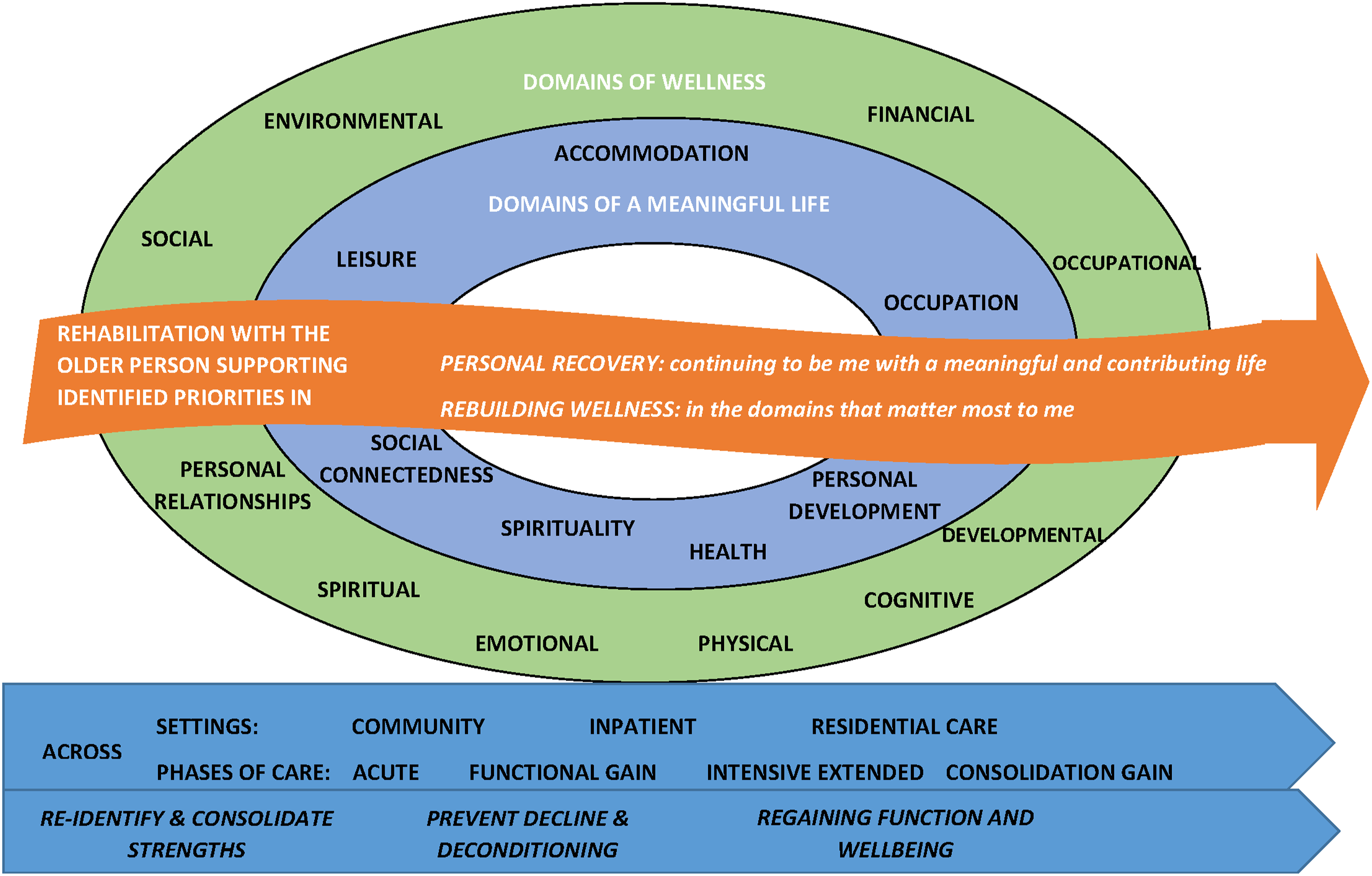
A rehabilitation approach should inform care across all settings and phases of care to: (1) Identify and consolidate strengths from the point of first contact (including sense of identity); (2) Prevent decline or deconditioning secondary to interventions and (3) Facilitate easier regaining of functioning and wellness.
Many factors should influence the location of care including realistic appraisal of local options but centred on the recovery and wellness goals of the person, supported as desired by their carer. This requires engagement with partner organizations relevant to those goals. It also requires overcoming the ageism that can inhibit the hope of professionals, the older person and those close to them. 26 For people with dementia, support from families and carers is critical in enabling a person’s continuing sense of identity. Enhancing older people’s access to specialized mental health rehabilitation that meets their needs can be achieved in part in current community, inpatient and residential care settings. However, further work is needed to develop models that integrate optimal environments, staff with rehabilitation skills, specialist older people’s mental health services and other care partners.
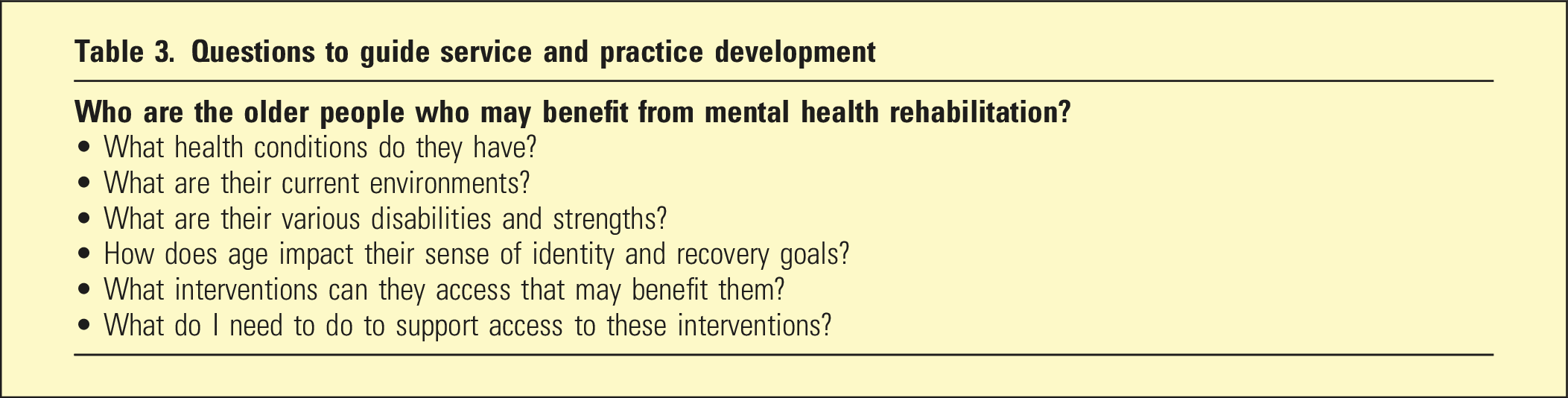
Questions to guide service and practice development
Effective rehabilitation with older people with complex mental illness and their carers has potential to enhance lives and save money through reduced hospital bed use and premature entry to residential aged care.