
Abstract
Objective
To describe (i) the clinical characteristics of individuals referred to the Tertiary Referral Service for Psychosis (TRSP) and (ii) the recommendations TRSP made for future treatment across psychopharmacological and other intervention domains.
Method
Retrospective audit of clinical data collected during the assessment process of individuals who accessed TRSP between 02/06/2020 and 31/12/2022. Categories of recommendations made following collaborative care planning comprised psychopharmacological, neuropsychological, psychological, psychosocial, physical health, substance misuse and other domains.
Results
Eighty-two individuals were included, with diagnoses most commonly of schizophrenia (54.9%) and schizoaffective disorder (30.5%). The median PANSS score was 88.0 (73–100). Social occupational functioning was very poor (SOFAS M = 37.0, SD = 15.1). Cognitive functioning was poor (RBANS: M = 74.6; SD: 15.0). 67.1% had physical health comorbidities, with high prevalence of smoking (52.4%) and substance misuse (25.6%). Psychopharmacological recommendations (made for 81.7%) included clozapine trial (25.6%), clozapine dose change/augmentation (22.0%) and rationalisation of polypharmacy (12.2%). Neuropsychological (73.2%), psychological (39.0%) and psychosocial (85.4%) recommendations included access to cognitive remediation, psychological therapy and disability support. Physical health and substance misuse interventions were recommended for 91.5% and 20.7%, respectively.
Conclusions
Individuals referred to the TRSP had marked clinical and functional impairments. Holistic collaborative care planning complemented psychopharmacological interventions with psychological, psychosocial and physical healthcare recommendations.
Psychotic illnesses affect around 1 in 200 people globally 1 and have a detrimental impact on an individual’s daily functioning and relationships. 2 Whilst recovery following a first episode of psychosis is possible, many individuals experience multiple episodes of illness or the persistence of symptoms over a long duration. 3 Approximately one-third of individuals who experience psychosis have a treatment-resistant illness,4,5 which may include positive, negative and cognitive symptoms.6,7
Complex psychosis is a broad term used to refer to a diagnosis of psychosis that is characterised by ‘severe and treatment-resistant symptoms of psychosis and functional impairment’ (NICE Guidelines, UK). 8 This extends beyond treatment-resistant schizophrenia alone to include individuals for whom treatment has provided limited benefit, those who have a high illness burden in terms of symptom severity or functional capacity and those with co-occurring physical health conditions, substance misuse, intellectual disabilities or cognitive impairments. Such complexities often result in unidentified and unmet health needs, which contribute to increased use of acute services, such as emergency departments.9,10
The Tertiary Referral Service for Psychosis (TRSP) is an NSW-state-wide, publicly funded service providing specialist consultation to mental health teams who support people experiencing complex psychosis. The TRSP aims to improve the lives of people with complex psychosis through the provision of recovery-focused intensive and individualised therapeutic approaches for individuals and their families/carers. The TRSP draws upon research and international guidelines to formulate evidence-based holistic and comprehensive treatment recommendations which are discussed with the referring team and the individual to ensure that the final collaborative care plan is acceptable and deliverable. The service is described comprehensively elsewhere, where detail is provided of the subset of individuals who received a diagnosis from TRSP of treatment-resistant illness.11,12 Treatment-resistant schizophrenia is defined as ‘an inadequate clinical response to sequential treatment with at least two different antipsychotics at an adequate dose, duration, and adherence’ (TRRIP).
13
In real-world settings, however, there is heterogeneity in the diagnosis of treatment resistance, due to numerous factors including pseudoresistance, misdiagnosis, inadequate treatment and comorbidities.
14
Therefore, a comprehensive approach to treatment of severe psychosis should extend beyond treatment resistance illness alone, as reflected in TRSP reasons for referral (Figure 1). Reasons for referral to the Tertiary Referral Service for Psychosis (TRSP)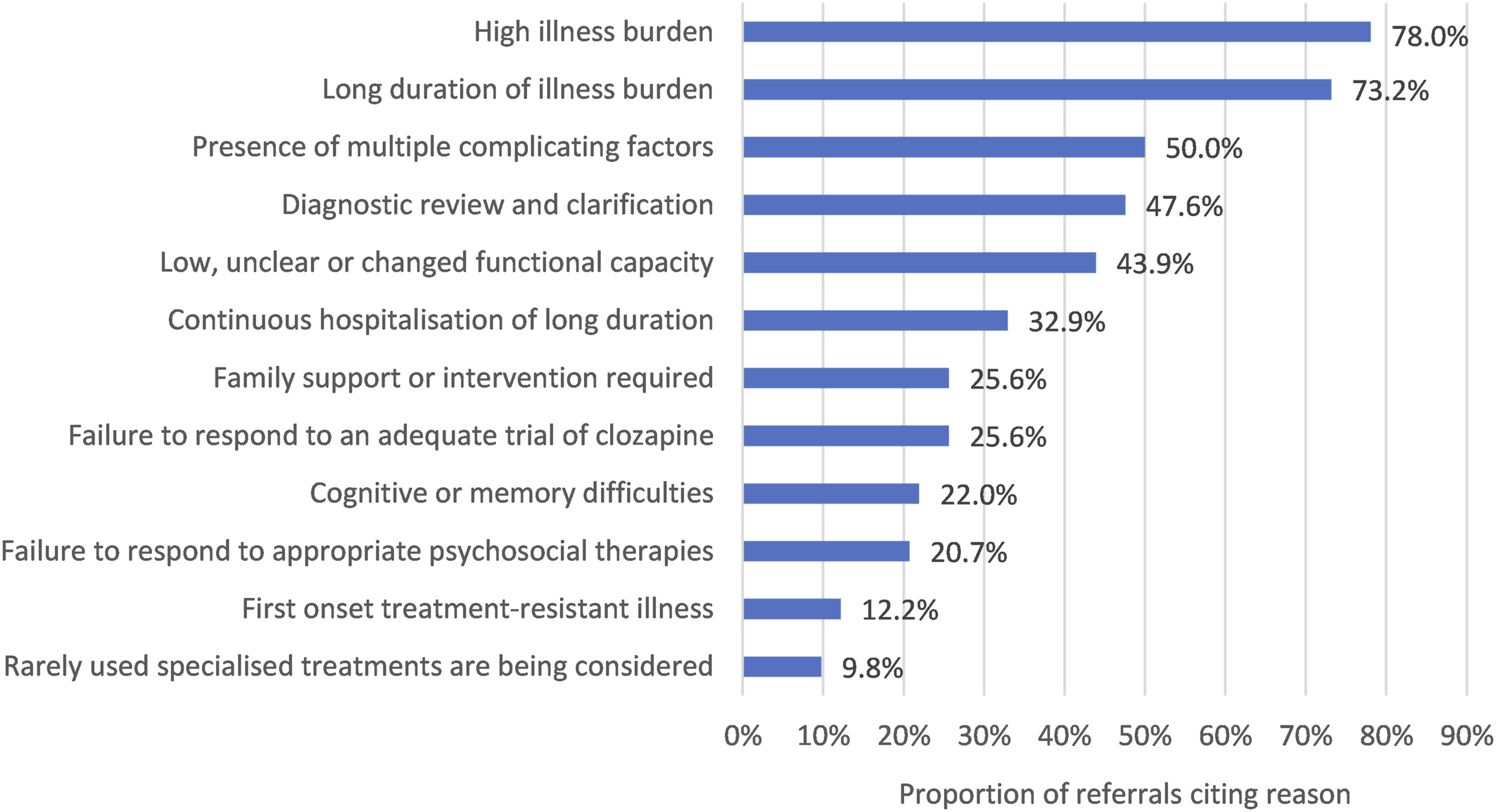
The aims of this article are to describe (i) the clinical characteristics of individuals referred to the Tertiary Referral Service for Psychosis since inception and (ii) the recommendations for future treatment across psychopharmacological and other intervention domains.
Methods
Setting
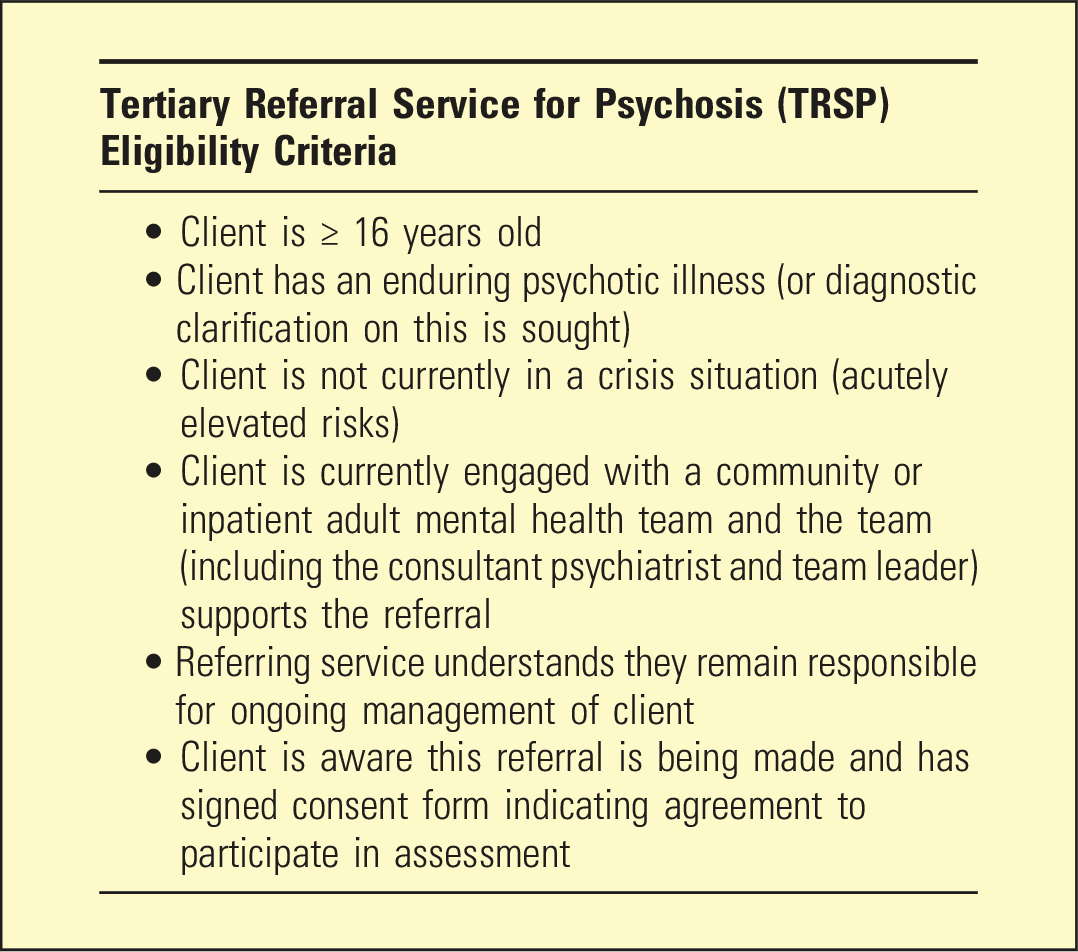
Referrals to the TRSP can be made from public mental health services for individuals who meet the eligibility criteria (Box 1). Individuals were seen in-person or by telehealth. Medical assessments were completed by the consultant psychiatrist and registrar, neuropsychological assessments by the neuropsychologist, psychosocial assessments by the social worker and occupational therapist and physical health assessments by the TRSP-affiliated general practitioner. Collateral information was sought from clinicians, support workers, family and broader support networks where consent was given to do so.
Study design
A retrospective audit was conducted of clinical data collected as part of the assessment process for individuals who accessed the service from inception (2 June 2020) to 31 December 2022. This project was reviewed and approved as a quality improvement project by South Eastern Sydney Local Health District (Ref: T20/81560).
Measures
During clinical interview, the psychiatrist collected information on relevant clinical history and utilised standardised measures to assess the severity of illness and functioning. Psychotic symptom severity was assessed using the Positive and Negative Symptoms Scale (PANSS) 15 and the Clinical Global Impression Schizophrenia scale (CGI-SCH). 16 The Social and Occupational Functioning Assessment Scale (SOFAS), Health of Nation Outcome Scales (HoNOS) 17 and Life Skills Profile-16 (LSP-16) 18 were used to assess current socio-occupational functioning. Current mental distress was measured using the Kessler Psychological Distress Scale (K10). 19 Antipsychotic side effects were assessed via the Glasgow Antipsychotic Side-Effect Scale (GASS). 20
The neuropsychologist completed the Repeatable Battery Assessment of Neuropsychological Status (RBANS-Form A) 21 with all appropriate consumers as part of a wider neuropsychological battery. Age-corrected scaled scores (SSs) for the total score were calculated using manual normative data.
Comprehensive case note reviews were used to supplement information collected through interviews.
Data extraction
All data were collated and stored in REDCap. 22 Data were extracted by the TRSP research officer. In addition to the measures outlined above, data were also extracted on demographic information, reason cited for referral, duration of illness, diagnosis of psychotic illness, diagnosis of treatment-resistant psychotic illness, physical health comorbidity and tobacco and other substance use. Data on past and present treatments received were extracted, including past and current clozapine use, past receipt of psychological therapies, past receipt of ECT, current polypharmacy and current use of other psychopharmacological treatments (non-antipsychotic medications). Polypharmacy was defined as the prescription of two or more antipsychotics (excepting clozapine augmentation).
TRSP treatment recommendations were categorised as follows: psychopharmacological (e.g. clozapine trial or augmentation, polypharmacy rationalisation); neuropsychological (e.g. cognitive remediation therapy [CRT]); psychological (e.g. cognitive behaviour therapy for psychosis [CBTp]); psychosocial (e.g. initiation of/increase to disability support packages [National Disability Insurance Scheme in Australia], support/interventions for families/carers, occupational therapy assessments and behaviour support); physical health (e.g. smoking cessation, treatment of cardiometabolic conditions, preventative health screening); substance use support; and other (e.g. immunological treatment).
Data analyses
Demographic and clinical characteristics are reported descriptively using frequency statistics and measures of central tendency. The Shapiro–Wilk test was conducted to assess continuous data for normality. Means and standard deviations are used where the data were normally distributed and medians and interquartile range where those data did not meet normality criteria. Frequency statistics were used to report receipt of past treatment and to describe the categories of treatment recommendations made by the team.
Results
Eighty-three individuals were assessed. One individual referred for diagnostic review was found to have a non-psychosis diagnosis and was thus excluded. 45.1% (n = 37) were referred from inpatient services and 54.9% (n = 45) from community mental health teams. The most common reasons for referral were high burden of illness (78.0%) and long duration of illness burden (73.2%) (Figure 1).
Demographic and clinical characteristics of individuals accessing the Tertiary Referral Service for Psychosis (TRSP)
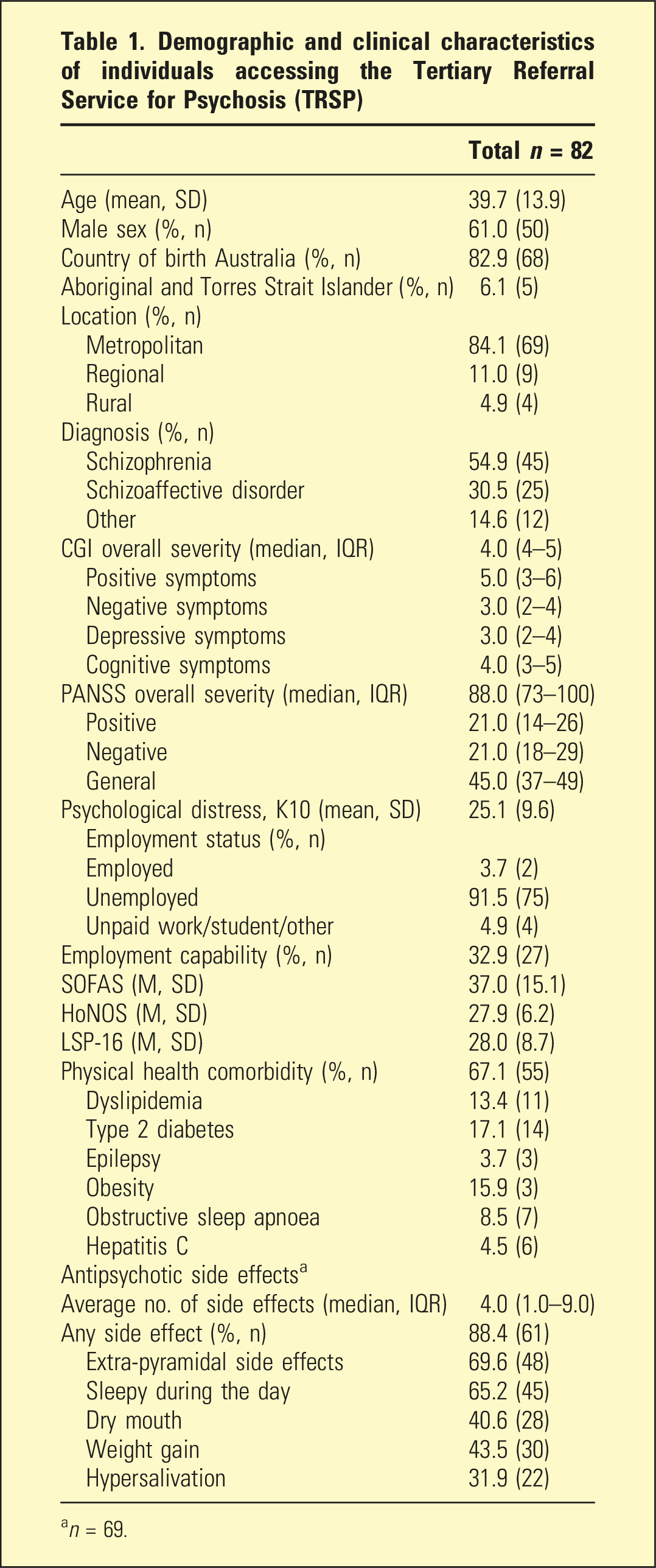
an = 69.
Neuropsychological assessments were completed for 74.4% (n = 61) individuals. Overall, the group had borderline-impaired global cognitive functioning (RBANS M = 74.6; SD: 15.0). 32.1% (n = 18) performed in the impaired range (Total RBANS SS <70), with another 28.6% (n = 16) scoring in the borderline-impaired range (Total RBANS SS 70–79).
Almost two-thirds (63.4%, n = 52) had been prescribed clozapine at some point and a quarter (26.8%, n = 22) were currently prescribed clozapine. Rates of polypharmacy were high at 37.8% (n = 31). Other prescribed psychopharmacological agents included antidepressants (28.0%, n = 23) and mood stabilisers (35.4%, n = 29). A fifth had previously received ECT (22.0%, n = 18). Only a third had ever received any psychological therapy (30.5%, n = 25). Of those, none had received CRT and just 8.0% (n = 2) had received CBTp.
Recommendations made by the TRSP team
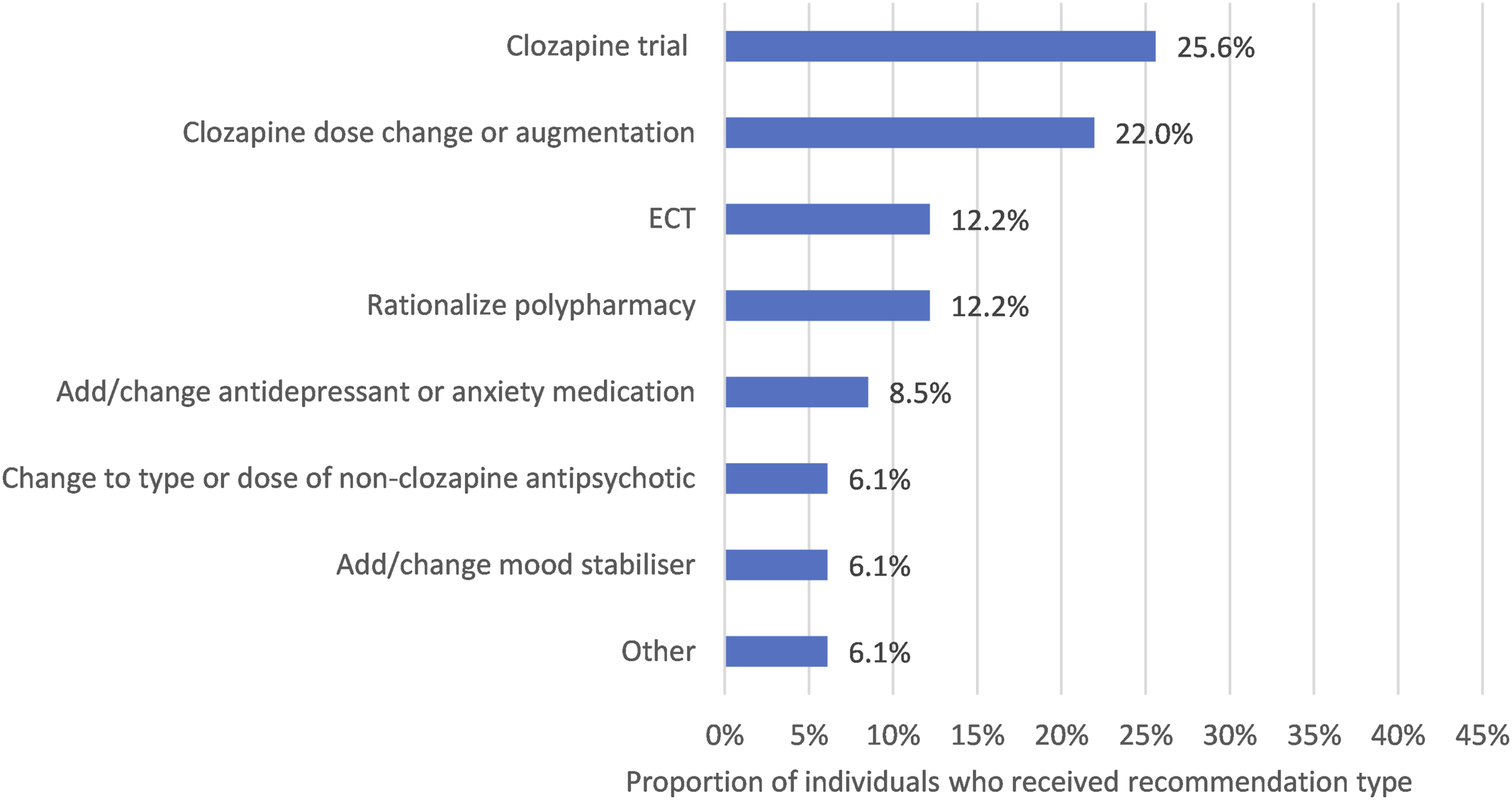
Pharmacological recommendations were made for most individuals (81.7%, n = 67) (Figures 2 and 3). These included recommendations for a clozapine trial (25.6%, n = 21), change to current clozapine dose or introduction of augmentation agent (22.0%, n = 18), ECT (12.2%, n = 10) and strategies to rationalize polypharmacy (12.2%, n = 10). Neuropsychological recommendations were made for 73.2% (n = 60), including CRT (20.7%, n = 17), provision of cognitive strategies (43.9%, n = 36), educational support (6.1%, n = 5) and re-assessment for monitoring (11.0%, n = 9). Psychological recommendations were made for 39.0%, (n = 32) (Figure 2), including CBTp (15.9%, n = 13), and other psychological support (24.4%, n = 20) such as referrals to specialist trauma services, family therapy and interventions for mood/anxiety symptoms. Recommendation types made by the Tertiary Referral Service for Psychosis (TRSP) team (n = 82) Psychopharmacological and ECT recommendation types made by the Tertiary Referral Service for Psychosis (TRSP) team (n = 82)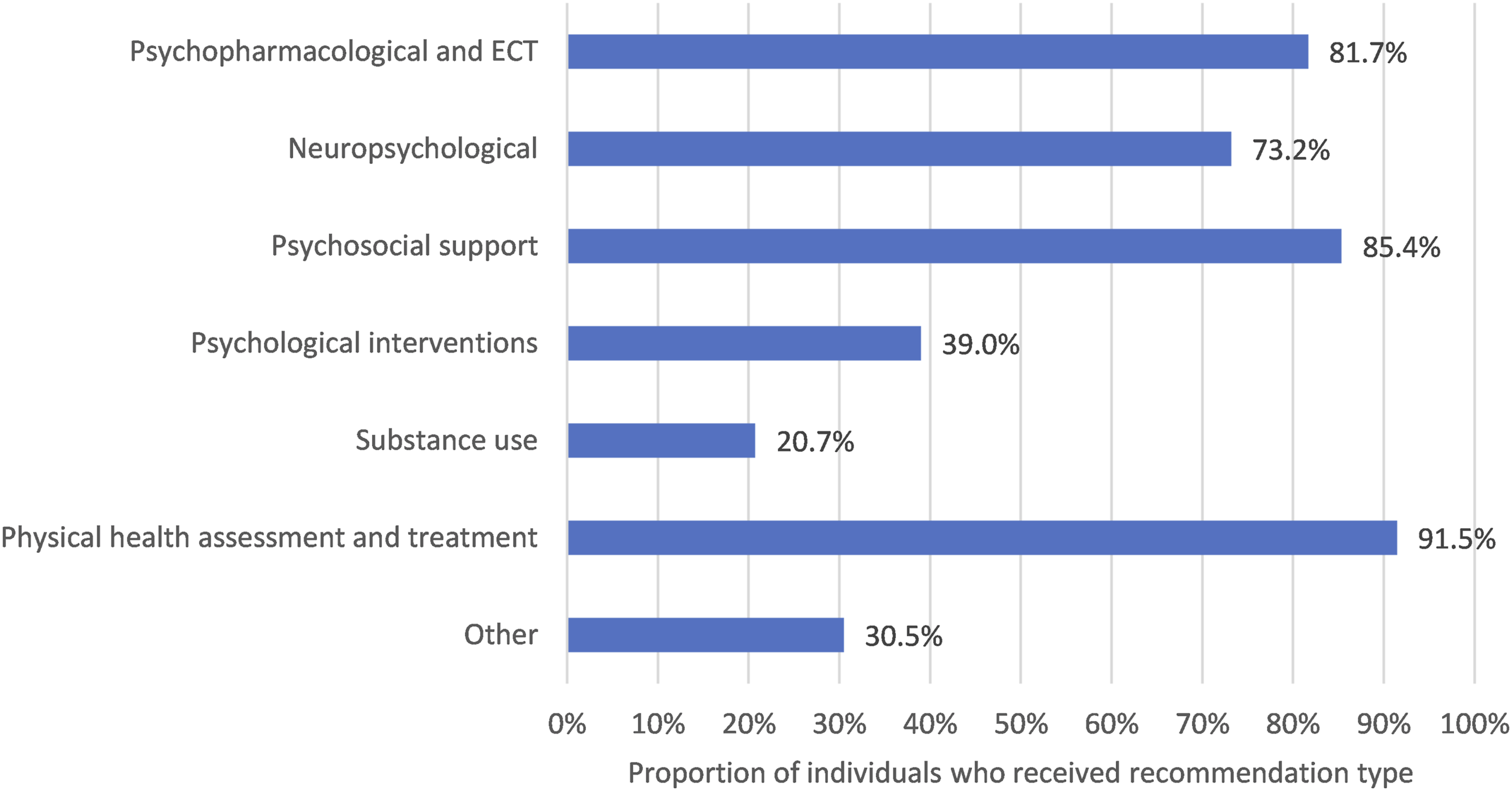
Most received psychosocial recommendations (85.4%, n = 70), of which two-thirds included the initiation of or increased disability support packages (65.9%, n = 54).
Physical health recommendations (91.5%, n = 75) were made for almost everyone, including cardiometabolic screening and assessment, immunisation, smoking cessation and preventative health screening. Substance misuse support was recommended in 20.7% (n = 17). Other recommendations (made in 30.5%, Figure 2) included a broad range of supports and interventions unique to an individual’s care plan (e.g. genetic testing, consideration of guardianship, cultural supports, referral to specialist services).
Discussion
Individuals assessed by the Tertiary Referral Service for Psychosis demonstrated major impairment in social occupational function and were markedly ill, with notable cognitive impairment, in keeping with a complex psychosis population. The TRSP cohort was similar in age, gender, duration of illness and diagnosis to the population described by the UK inpatient National Psychosis Unit, 24 which specialises in providing care for people with treatment refractory psychosis in an inpatient setting rather than via the consultation-liaison model employed by the TRSP.
TRSP psychopharmacological recommendations were made in almost all cases, reflecting the high prevalence of treatment resistance illness. 12 Recommendations were made, where feasible, to rationalise polypharmacy, in line with international treatment guidelines, given its potential to increase side effects 25 which were commonplace in the cohort.
International guidelines suggest that individuals considered to have complex psychosis benefit from a focus on recovery and rehabilitation, beyond that of symptom management alone. 8 TRSP holistic recommendations extend beyond pharmacological interventions to include neuropsychological and psychological therapies, psychosocial interventions to develop skills, education or occupational support, collaboration with families and carers and physical health assessments and screening. Evidence-based neuro/psychological therapies such as CRT and CBTp had been previously provided to almost none of the cohort, in line with evidence of poor access to psychosocial interventions in Australia for people with severe mental illness. 26 Family therapy has a strong evidence base in reducing relapse and carer burden but similarly is rarely accessible for people living with severe mental illness, and this is due not to individual characteristics but rather to the ability of services to offer and deliver this care. 27 There is growing recognition of the need to increase access to trained therapists in these evidence-based modalities. 11
Psychosocial support was recommended for every five in six people, demonstrating that current support was non-optimal. Documented reports provided through TRSP occupational therapy and social work assessments were designed to enable referring teams to apply for or enhance existing disability support packages. Physical health interventions were recommended for almost everyone, reflecting the very high prevalence of physical health comorbidities observed in people with complex psychosis, particularly cardiometabolic issues and high rates of smoking.28,29 Smoking cessation and substance misuse interventions were frequently offered and accepted. The comprehensive physical health review conducted by the TRSP-affiliated GP drew attention to issues which individuals and referring clinicians were generally very willing to pursue treatment for. This was somewhat at odds with some of the psychopharmacological treatments initially proposed in the collaborative care planning meetings: where indicated, for example, in the case of treatment-resistant illness, where clozapine had not been trialled or was underutilised, individuals at times refused to consider retrial/increase in dose of clozapine. This was also observed at times when ECT was mooted for the same indication. The TRSP ethos of collaborative care planning, where individuals retain decision-making capacity, acknowledged the views of the individuals in such cases so that final recommendations comprised only those interventions which they agreed to. There remained high proportions of people who were willing to consider clozapine trial or augmentation.
A limitation of this study is the retrospective nature of data collection through case note review which was in turn limited by the quality of the medical record, meaning that key information about receipt of previous trials of medication or psychosocial therapies was recorded as present only if it had been documented in the medical record.
Conclusions
The NSW Tertiary Referral Service for Psychosis provides support to people with complex psychosis through both comprehensive multidisciplinary assessment and holistic recommendations across psychopharmacological, psychological, psychosocial and physical health domains. The holistic recommendations in line with recovery principles hold promise for a person-centred approach to care of complex psychosis which could be extended throughout Australia.
Footnotes
Acknowledgements
The research team would like to thank all TRSP clinical and support staff and the individuals who participated in the Tertiary Referral Service for Psychosis assessments.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the New South Wales Ministry of Health, the Commonwealth Community Grants Hub and the Mindgardens Neuroscience Network.
Ethical approval
This project was reviewed and approved as a quality improvement project by South Eastern Sydney Local Health District (Ref: T20/8156).