
Abstract
Objective
To explore the knowledge and attitudes of psychiatrists about psychedelics therapies.
Method
Access to a cross-sectional survey was distributed to psychiatrists through social media channels. Attitudes and knowledge about psychedelic therapies were recorded using Likert scales and ranking questions.
Results
Fifty-eight complete responses were collected (44 fully trained +14 trainee RANZCP members). Greater than 85% of respondents agreed there is a shortfall in effective psychiatric treatments, and greater than 65% agreed that psychedelic therapies might address this shortfall. The psychiatrists did not consider themselves knowledgeable about psychedelic therapies, with 60% showing interest in further training on this topic. About 70% of the sample hold various concerns about psychedelic therapies, and more believe that the prescription of psychedelics should be limited to psychiatrists in the future.
Conclusion
Considering these results in the context of a rapidly changing landscape relating to psychedelic research and regulations, we suggest there is scope to develop up-to-date education about psychedelics for psychiatrists.
Humphry Osmond publicly coined the word psychedelic in 1956, with the intent it is ‘clear, euphonious, and uncontaminated by other associations’. 1 Over half a century later, the word psychedelic keeps just one of these original intents alive: it is still more pleasing to the ear than its alternatives, for example, hallucinogen or psychotomimetic.
Unfortunately, in 2022 it is unclear what a psychedelic is. Though taxonomies exist for classifying psychedelics, none are universally accepted. 2 In this paper, it is meant as defined by the RANZCP Clinical Memorandum on psychedelic therapies: ‘any psychoactive drug that can induce states of altered perception and thoughts, often with heightened awareness of sensory input but with diminished control over attention and experience’. 3
Regarding the third hope Osman held for the word psychedelic, seventy-plus years of history means it is now inextricably laden with socio-political associations. 4 Psychedelics have been subject to the most prohibitive level of substance control since the War on Drugs began in the 1970s. Indeed, researchers suggest this is because of such associations, rather than in response to clear physiological, psychiatric, or evidence collected, otherwise which shows they are highly harmful – especially in comparison to many substances under lower controls – or lack therapeutic potential.5–7
To the contrary, the available research shows that in therapeutic doses, psychedelics ‘demonstrate an initial high safety ratio and low-risk profile with limited physiological concerns’. 3 There is also emerging evidence that they show therapeutic promise for a range of mental disorders. Consequently, a change is underway in the landscape of psychedelic regulation and research. For example, the US-FDA has granted ‘Breakthrough Therapy’ status to multiple trials of psychedelics over the last 5 years, meaning psilocybin and 3,4-Methylenedioxymethamphetamine (MDMA) are potentially on an accelerated path towards clinical approval.8–10
As with the translation of any new therapy from benchtop-to-bedside, a willing uptake by practising clinicians is a prerequisite. In the context of conflict between historical connotations and the rapidly evolving evidence base, what do psychiatrists think, know, and feel about psychedelics? As a brief survey of psychiatrists, this study aims to add to the nascent evidence base which is beginning to answer these crucial questions.
Methods
A cross-sectional survey was designed by the authors and approved under institutional ethics governance. The survey included the collection of demographic data and a questionnaire: within were 14 items (S1) about psychedelic therapies – given on a 7-point Likert scale ranging from Strongly Disagree to Strongly Agree – and two additional items about psychedelics, which asked respondents to rank given options in order from most-to-least probable. SurveyMonkey hosted the survey between 10/01/2022 and 07/04/2022.
Sampling and consent
A call-for-participation (S2), including a hyperlink to the survey, was emailed directly to colleagues of the investigators, posted on social media platforms (e.g. Twitter), and allowed to spread via passive snowball (i.e. word-of-mouth). Consent for participation was obtained online, during which the respondent affirmed they were either a full-trained psychiatrist or a psychiatry trainee.
Reporting and Statistical analysis
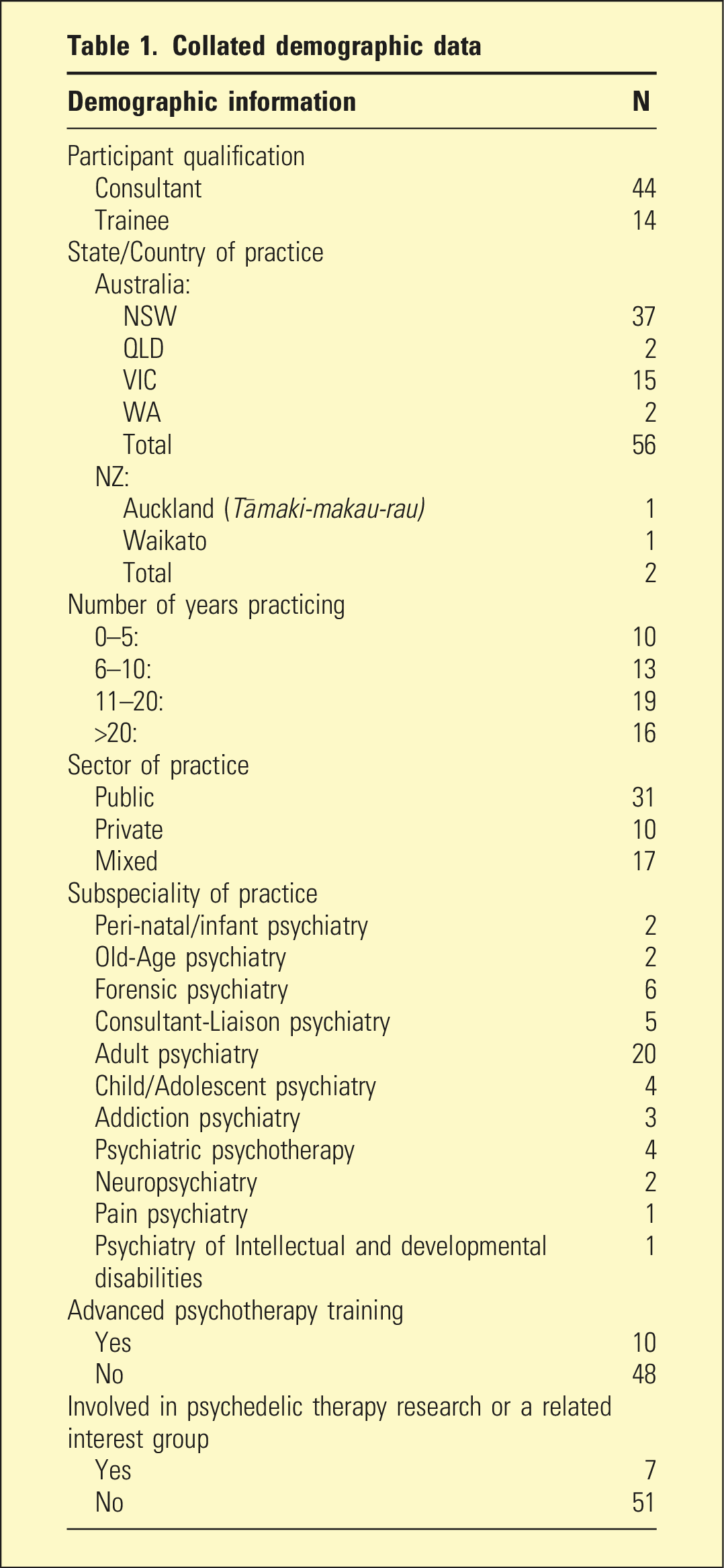
Collated demographic data
Results
Demographics
The sample (n = 58, Male = 40, Female = 18; Age mean = 46 y.o., Age range. = 27–66 y.o.) included 44 fully trained specialists and 14 psychiatry trainees: approximately 0.8% and 0.7% of their RANZCP groups, respectively. The sample consisted of approximately 3:1:2 private-to-public-to-mixed-private–public practitioners, with greater than 95% practising within Australia.
Likert items
Attitudes about current and emerging treatments
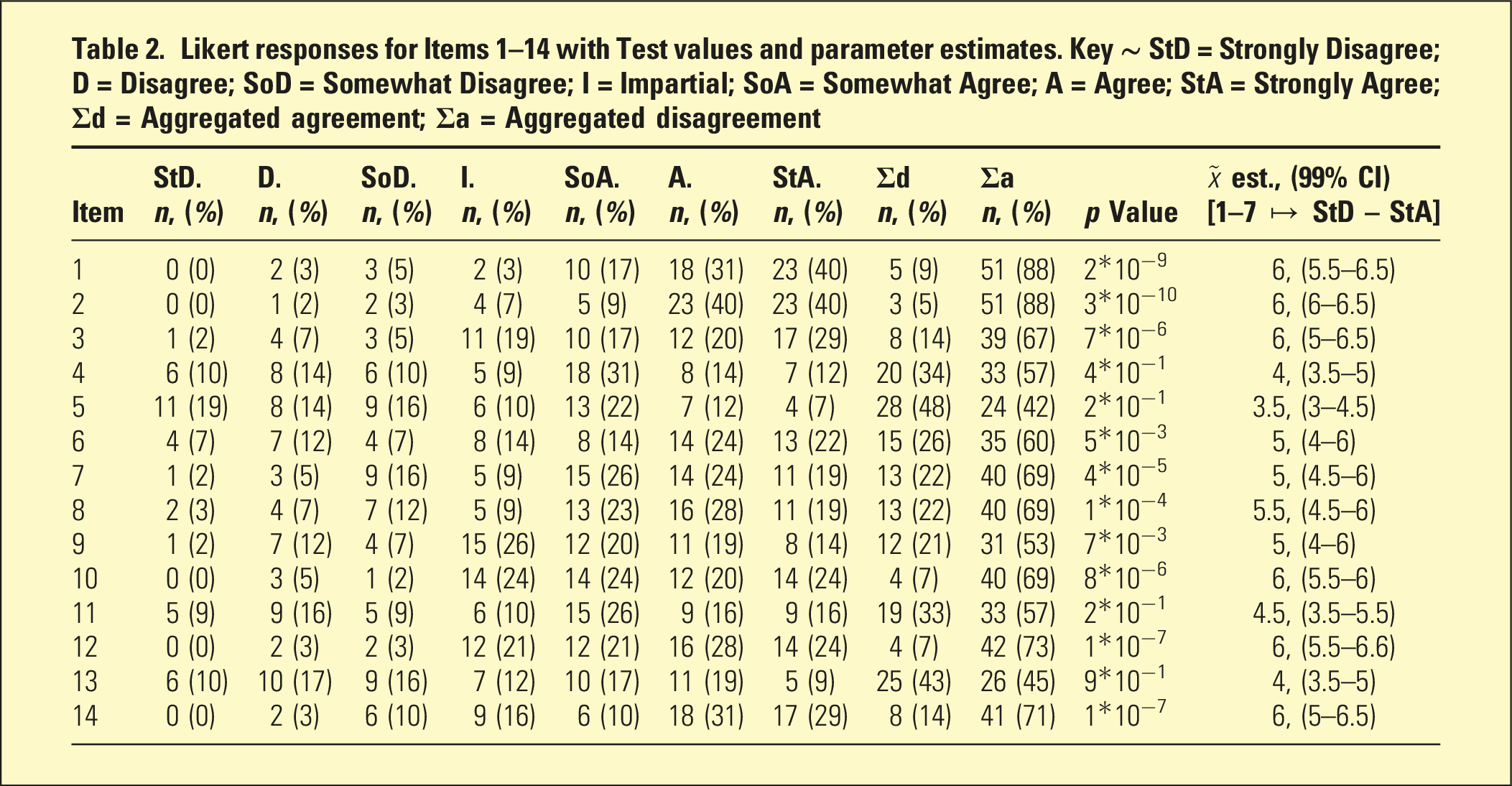
Likert responses for Items 1–14 with Test values and parameter estimates. Key ∼ StD = Strongly Disagree; D = Disagree; SoD = Somewhat Disagree; I = Impartial; SoA = Somewhat Agree; A = Agree; StA = Strongly Agree; Σd = Aggregated agreement; Σa = Aggregated disagreement
Knowledge about psychedelics and interest in further training
The responses to Items 4 and 5 (Table 2) were not significant evidence against the Hnull, suggesting the psychiatrists are equivocal about their knowledge regarding the theory and practicalities of psychedelic therapies. Yet, with 60% of respondents agreeing to Item 6, this was significant evidence (Table 2) to suggest many are interested in undertaking further training to bolster their knowledge. Though the tendency of responses to this item was to mark Somewhat Agree, notable minorities (>20%) marked Agree and Strongly Agree.
Concerns about psychedelic therapies
The responses to items 7, 8, 9, and 10 were significant evidence (Table 2) that shows the psychiatrists have concerns about the safety, access, and regulations of psychedelic therapies. The tendency of the sampled responses for each of these items was to have marked Somewhat Agree, with about 70% of the respondents agreeing with concerns elaborated in Items 7, 8, and 10. Yet only a slim majority (53%) agreed with Item 9, that is, holding concerns about the affordability of psychedelic therapies, and almost equal proportions being equivocal or disagreeing.
Prescription and delivery of psychedelic therapies
The responses to Item 11 were not significant evidence (Table 2) against the Hnull, despite more than 55% of respondents agreeing with the statement. For Item 12, the responses represent significant evidence against the Hnull (p = 1 × 10−7). Conversely, the responses to Item 13 did not supply significant evidence against the Hnull (p = 9 × 10−1). Indeed, the responses showed approximately equal minorities, with about 45% agreeing and disagreeing. Finally, greater than 70% of the sample agreed with Item 14, supplying significant evidence against the Hnull. Their results show that the sample believes that future prescriptions of psychedelic therapies should generally be restricted to psychiatrists, and delivery of these therapies should occur in specialised centres.
Ranking items
In ranking which types of mental disorders may benefit from psychedelic assisted-therapy (Figure 1), greater than 85% of respondents ranked two types as the most probable: Trauma-related and Mood. Equally so, the respondents were clear in showing that they thought Psychotic disorders greater than 55%, followed by Developmental disorders less than 30%, are least likely to receive help from these therapies. Psychiatrists’ rankings of which disorder are likely to benefit from psychedelic therapies.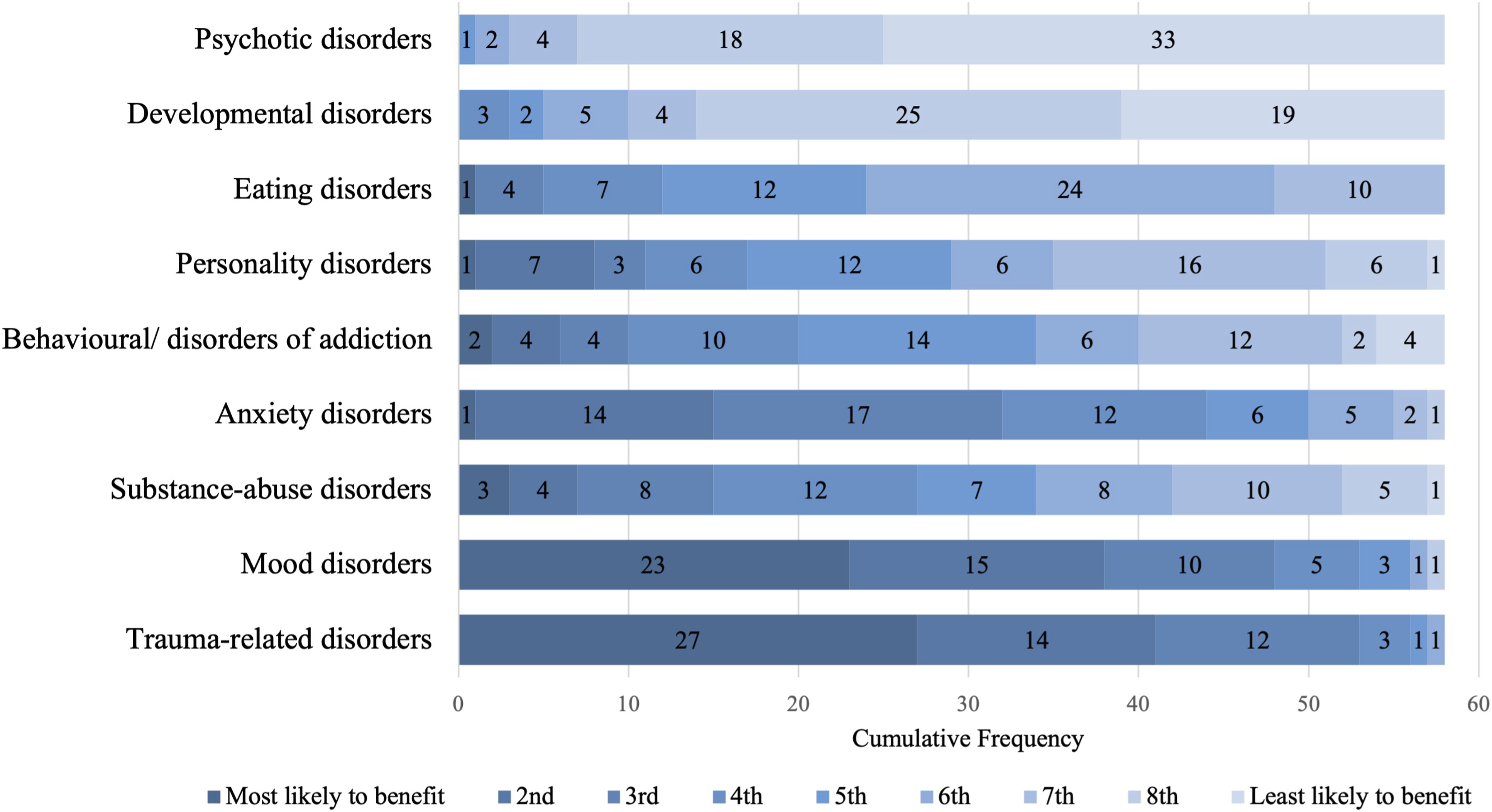
When ranking which substances the respondents believed is most promising as part of psychedelic assisted-therapy (Figure 2), greater than 70% ranked one of two as the most probable: psilocybin (40%) and ketamine (33%). Conversely, in ranking the substance, they believed the least promising, greater than 80% ranked one of three as the least probable: ayahuasca (38%), mescaline (33%), and DMT (28%). Psychiatrists’ rankings of which substance are most likely to be useful as part of psychedelic therapy. MMDA = 3,4-Methylenedioxymethamphetamine.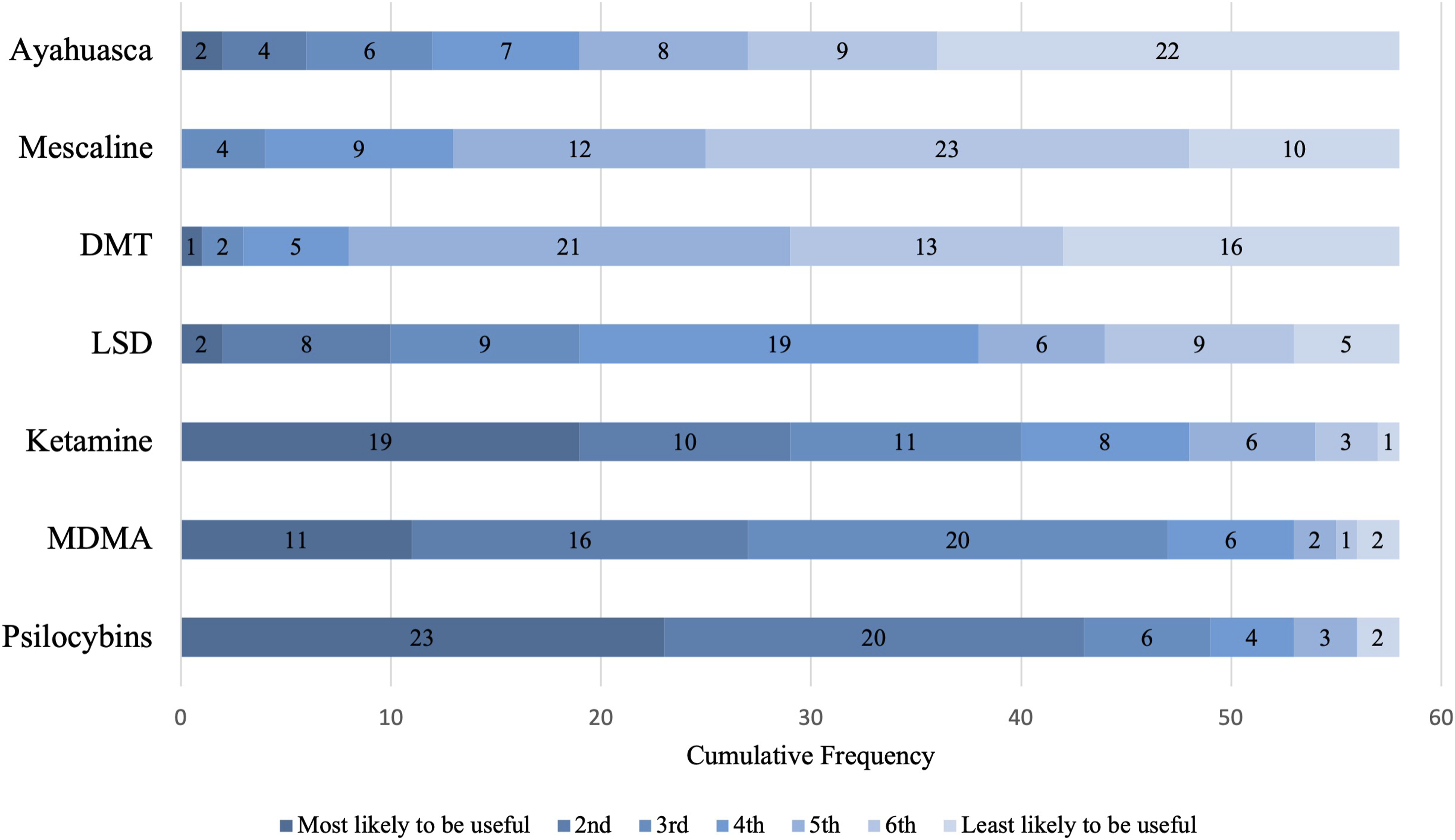
Discussion
The results from this survey add to the nascent evidence base13,14 informing us of psychiatrists’ attitudes about psychedelic therapies. These come in the context of a world where mental health disorders are: widespread (1-in-8), undertreated (e.g. <70% of psychoses are treated), under-resourced (just 2% of the average health worldwide), and have recently shown an uptick due to the COVID-19 pandemic. 15
The results from this survey show that the psychiatrists unequivocally agree there exists a shortfall in safe-and-effective psychiatric treatments, and there is a great need to address the shortfall. They also show that psychiatrists tend to agree (>65%) that psychedelics are a promising avenue for addressing this perceived shortfall, with few disagreeing (<15%) or staying impartial (∼20%). Despite holding this hope for psychedelics, psychiatrists seem not to be confident in their knowledge about them. In line with these results, 60% displayed interest in further training about the theory and application of psychedelics within a clinical setting. We suggest these results reveal the scope to develop up-to-date education about psychedelics for psychiatrists.
Previously, Wright et al. (2021) showed there exists hesitancy amongst Australian psychiatrists for the recommendation of a psychedelic assisted-therapy compared with an unlabelled comparator. Wright et al. suggest this hesitancy may result from historical stigma or concern generated through the generalisations of harm associated with high recreational dosing. 14 The responses made by the psychiatrists to items 7–10 showed about 70% of this sample do have concerns about the safety of psychedelic therapies, amongst other factors such as access and regulation. In accord with hesitancy driven by concern about harm, a similar majority (∼70%) also agreed that future prescriptions should be restricted to psychiatrists. Moreover, the sample remained equivocal (45% agreeing and 45% disagreeing) on whether other clinicians, such as palliative care physicians or general practitioners, should be able to prescribe psychedelic therapies, even if in consultation with a psychiatrist.
Yet despite the concerns and cautions reflected in these results, in response to Item 11, querying whether the respondents would consider using special access pathways prior to conventional pathways becoming available, the psychiatrists were equivocal – surprisingly, there was a small minority (>55%) who agreed with this item. We suggest that most of the psychiatrists did not disagree with this item out-of-hand because, despite having concerns, the perceived shortfall of effective treatment alternatives and the burden of mental disorders reflect a perceived risk-benefit trade-off. Indeed, no treatment comes without a risk profile and early this year, Levin et al. (2022) showed that psychiatrists perceived at least one psychedelic substance (psilocybin) as safer, holding less abuse potential, and potentially more therapeutic than drugs of lower scheduling such as alprazolam or methamphetamine or even legal intoxicants like alcohol. Importantly, this perception of an incongruency between the drug harms and the high levels of controls imposed on many psychedelics is also supported by thorough research. 6
Limitations of this study include its cross-sectional, brief, and closed-question design and its modest sample size, meaning the full range of attitudes/opinions was likely not sampled. Also, the sampling methods that allowed for self-selection may have introduced unintended bias. Indeed, as reported, 12% of the respondents noted they were either involved in psychedelic research or part of a special interest group (i.e., more knowledgeable/interested about psychedelics than the expected median respondent).
In conclusion, this study has added insight into the attitudes of Australian and New Zealand psychiatrists about psychedelic therapies. We hope the results highlight the interest and knowledge of RANZCP members about psychedelics and may be useful for future policy direction about the education and training of members.
Supplemental Material
Supplemental Material - The prescription of psychedelic therapies in Australia and New Zealand: A brief survey of psychiatrists
Supplemental Material for The prescription of psychedelic therapies in Australia and New Zealand: A brief survey of psychiatrists by Joshua J Berger and Paul B Fitzgerald in Australasian Psychiatry.
Footnotes
Funding
The authors received no financial support for the research, authorship, or publication of this article.
Disclosure
The author reports no conflict of interest. The author alone is responsible for the content and writing of the paper.
Ethical approval
The planning and conduct of this study was completed under institutional ethics governance from Epworth HealthCare (No. EH2021-781).
Informed consent
Consent for participation was obtained online prior to the study, during which the respondent affirmed they were either a full-trained psychiatrist or a psychiatry trainee.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.