
Abstract
Objectives:
This aim of this qualitative study was to explore the experiences of clinicians involved with inquiries into the mental health care of patients who were perpetrators of homicide in New Zealand.
Methods:
Our purposive sample comprised ten clinicians working in New Zealand district health board mental health services. These clinicians were individually interviewed. Interviews were audio-recorded, transcribed and thematically analysed. The coding framework was checked and peer reviewed by an independent researcher.
Results:
Five themes were identified: the inquiry process; emotional burden; impact on team dynamics; changes to individual clinical practice; and perceptions of inquiries being influenced by organisational culture. Clinicians involved with inquiries reported significant anxiety and disrupted multidisciplinary team dynamics. Some participants found inquiries led to changes to their clinical practice and perceived that a punitive organisational culture limited learning.
Conclusions:
Clinicians perceived inquiries as threatening, anxiety provoking and primarily concerned with protecting organisational interests. Communication of the inquiry process and ensuring inquiry findings are disseminated may enhance clinicians’ experiences of inquiries and facilitate their participation and their reflection on changes to clinical practice that could contribute to improving services. Support for clinicians and multidisciplinary teams should be emphasised by the commissioning agency.
In New Zealand, violence perpetrated by mentally ill people that results in homicide is a source of grave concern for the public and clinicians working in psychiatric services.1,2 District health boards are required by the National Adverse Events Reporting Policy to report serious incidents to the New Zealand Health and Quality Safety Commission, a centralised agency that collates data on adverse events in healthcare. Since 2010, it has recorded 21 incident reports of mental health related homicides.
For clinicians, a mental health related homicide is a worst-case scenario which may be compounded by the inquiry that invariably follows.3–6 Inquiries have various forms, ranging from internal to statutory. Their purpose is to provide an account of events, to ensure accountability, to distil lessons from events to improve practice and restore public confidence in the system.7,8 There is no standardised or accepted way of conducting inquiries into mental health incidents9,10 although inquiry panels may use a structured protocol that emphasises organisational and system problems. 11
An incident involving a death associated with healthcare can provoke intense emotional reactions in healthcare professionals. 12 Mental health clinicians may be distressed after a patient’s suicide and other violent acts including homicide.2,13 However, there is limited research into clinicians’ experiences of mental healthcare related inquiries. 14 We found one survey of psychiatrists with forensic expertise about different types of inquiries in the United Kingdom and other European countries and one qualitative study of English social workers, who reported anxiety and defensive practices in relation to inquiries. 15 Therefore, we aimed to investigate the experiences of clinicians with mental health care related inquiries, specifically after a homicide where a perpetrator was a mental health patient. The study is part of wider research on inquiries9,16 that includes different perspectives of family members and members of inquiry panels.
Methods
Participants
Participants were identified by hospital managers who supplied reports of serious incident reviews following a homicide committed by a mental health patient under the care of three district health boards in Auckland, New Zealand, between 2007 and 2017. We used a stratified approach to sampling, with the aim of selecting participants from different professional disciplines involved with the care of patients in inpatient and community settings and/or the subsequent inquiry. The sample is fairly homogeneous in that all participants worked within a team structure and the impact of inquiries on their individual practice and teams could be compared. We acknowledge the potential for sampling bias, for example, resident medical officers were difficult to establish contact with and did not respond to invitations to participate.
Procedure
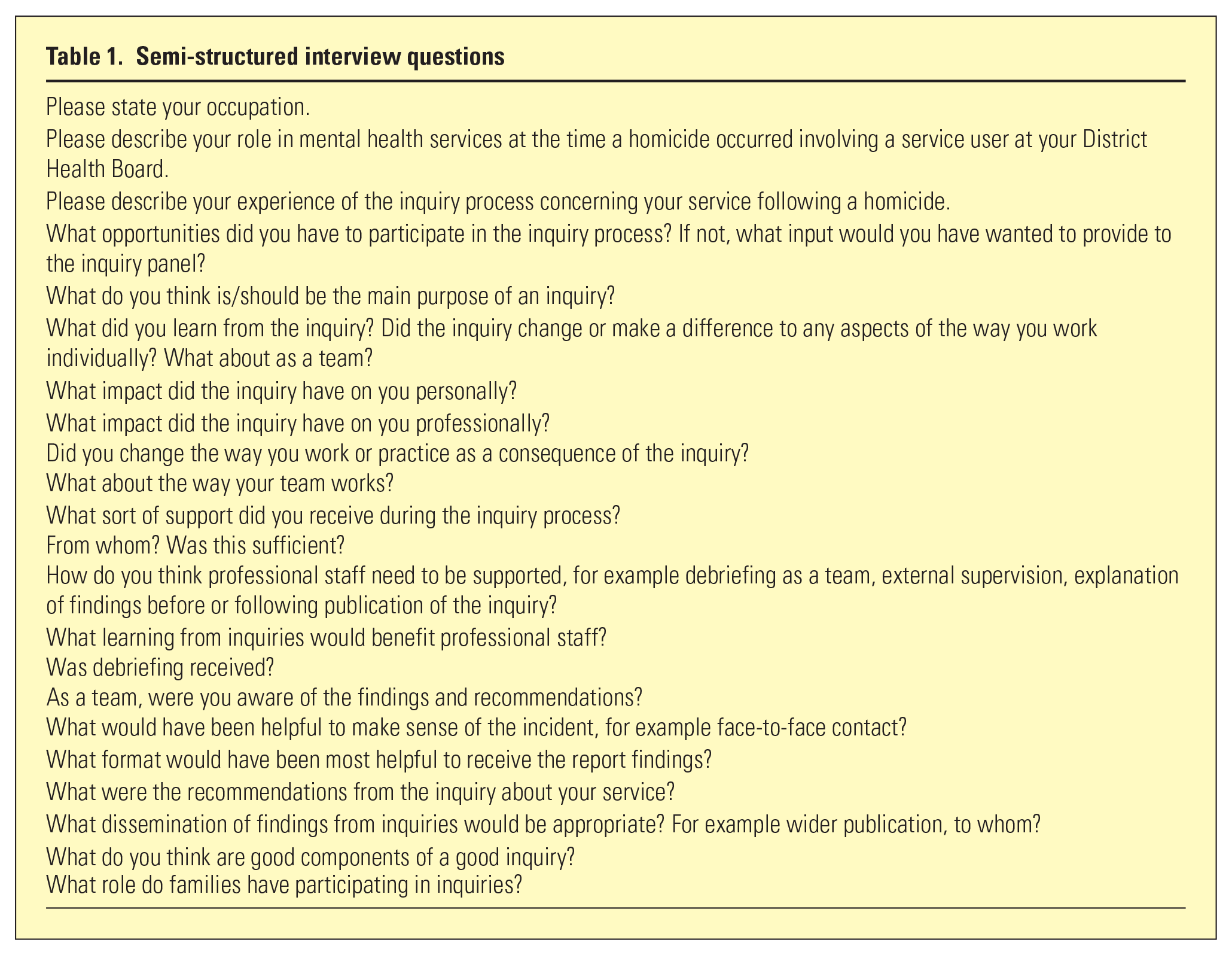
The study was approved by the New Zealand Health and Disability Ethics Committee. Participants gave their written consent to take part. The first author interviewed all participants, using a semi-structured interview guide (Table 1). At the time of the interviews, participants were made aware they could access employee-assisted counselling. Interviews were audio-recorded and transcribed. Following transcription, audio-recordings were deleted.
Semi-structured interview questions
Data analysis
Data were de-identified prior to storage in NVivo, a computer assisted qualitative data analysis programme. Transcripts were returned to the participants to confirm accuracy of the data, intensively read and coded by the first author 17 by labelling, organising and interpreting data. Memoranda were documented, highlighting observations, reflections and critical questions to provide an audit trail of the iterative process. The coding framework and memoranda were peer reviewed by an independent researcher to facilitate the development of concept themes. Codes and memoranda were progressively refined to form higher-order themes.
Results
The sample of ten participants included four psychiatrists, a nursing manager, three registered nurses, a social worker and a community support worker. All were employed by a mental health service at the time of the interview. The clinicians’ experience ranged from two to 30 years. The five themes identified – the inquiry process, emotional burden, impact on team dynamics, changes to individual clinical practice and perceptions of inquiries being influenced by organisational culture – are illustrated by quotations in Table 2.
Selected quotations to illustrate study themes
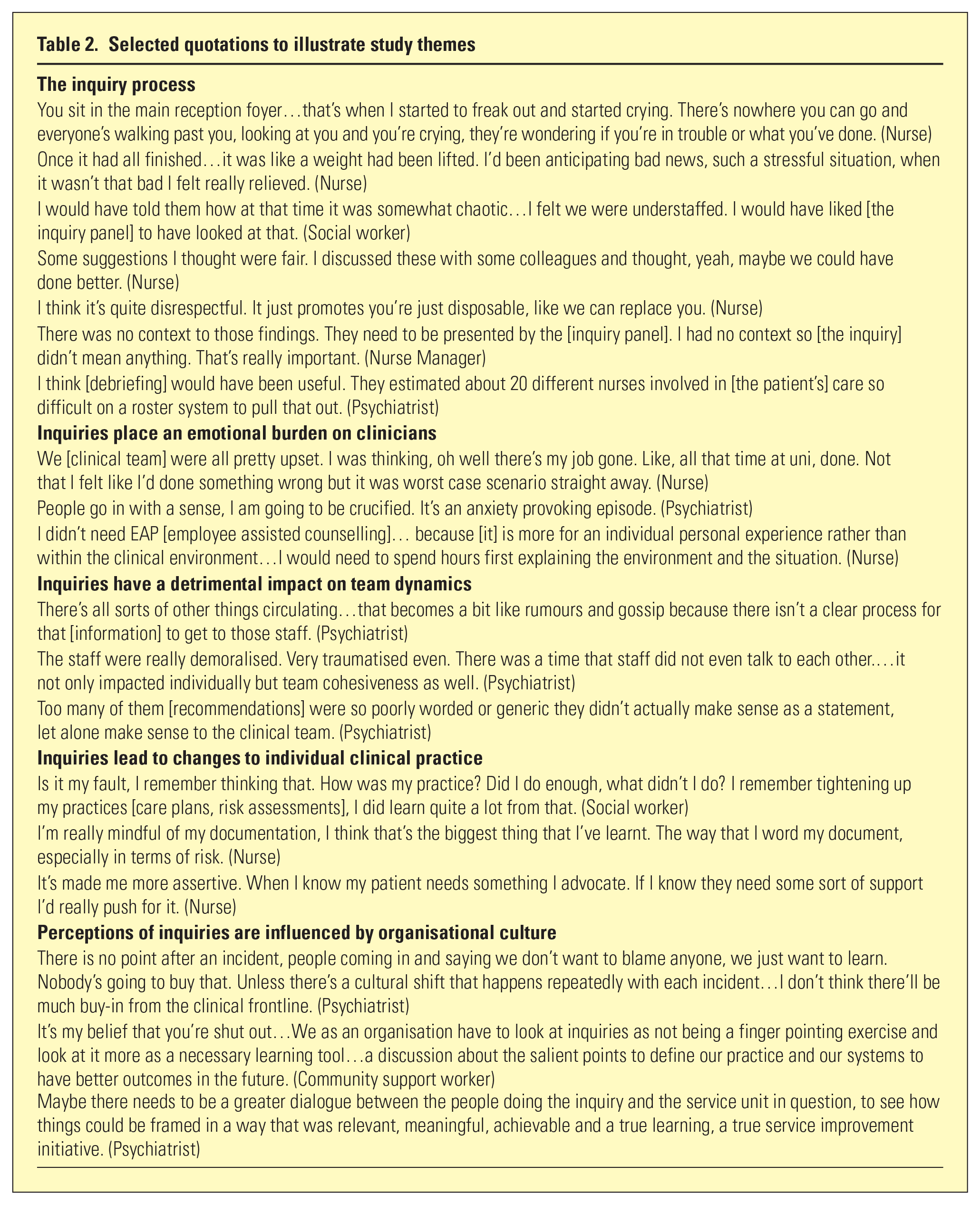
The inquiry process
The experiences of being notified about the homicide were variable. Some participants reported feeling poorly informed about the process. Most dreaded being interviewed by the inquiry panel yet some found the actual experience more positive. The stress of interview made some feel unable to articulate the pressures in their working environment to the inquiry panel. There were varied experiences of dissemination. Half of the sample did not receive any feedback. Two were involved with the feedback of inquiry findings to their team. All participants reported that specific time for the team to reflect on inquiry findings and recommendations would be beneficial.
Inquiries place an emotional burden on clinicians
Clinicians described feeling shocked to discover their patient had killed someone. Many felt stressed by the prospect of being sanctioned, including even highly experienced clinicians. Participants with no prior experience of inquiries were more significantly affected. Most participants sought support from peers or senior colleagues. None accessed free employee assisted counselling and some considered more specialised counselling was required.
Inquiries have a detrimental impact on team dynamics
Many participants perceived a heightened tension in their working environment during the inquiry. Minimal communication about the incident led to unhelpful speculation. Some reported that the inquiry had a negative impact on the team and observed that their teams struggled to make sense of an inquiry’s findings.
Inquiries lead to changes to individual clinical practice
All participants viewed inquiries as opportunities for reflection on their clinical practice. They identified other areas of learning: completing documentation, advocating for patients and asking critical questions in the clinical context.
Perceptions of inquiries are influenced by organisational culture
Most participants stated that their perceptions of inquiries were influenced by their district health board’s culture. Half of the sample perceived that blame was still a prominent feature of inquiries and were frustrated that inquiry findings were not transparent nor disseminated widely enough to clinical teams. More than half were mistrustful of the district health board and reported a disconnection between inquiry panels and clinical teams. The participants expressed empathy toward family members and most were open to meeting with families if this had been supported by the district health board.
Discussion
This study reports the experiences of clinicians who participate in an inquiry following a homicide perpetrated by a patient with a mental illness. The main findings were that such inquiries caused staff increased anxiety and disturbed team dynamics. There was a positive impact when staff reflected on aspects of clinical practice that could be improved, although this was not always the case. Clinicians believed inquiries were adversely influenced by organisational culture with a perceived disconnect between inquiry teams and clinical staff.
In other studies of serious mental health incidents, nurses have reported heightened anxiety associated with a homicide perpetrated by one of their patients.2,13 The participants in our study experienced a prolonged state of anxiety, in anticipation of an inquiry and during the process. Those who did not receive inquiry findings were left disappointed, some with a lack of resolution and a sense of not being valued. Most participants had collegial support and none sought formal psychological input. This is consistent with literature that clinicians turn to valued colleagues and supervisors after adverse events. 18
Our study has implications for organisational handling of inquiries and support for staff during the process. 19 Our results suggest that at least some clinicians believe that they may suffer professionally as a consequence of an inquiry of this type, and many do suffer emotionally. Therefore, we suggest that the commissioning agency should consider providing more information and formal organisational support for clinicians involved with inquiries of this type, to mitigate longer term psychological impacts on staff and further negative impacts on patient care. The fact that clinicians were sensitive to being blamed despite being told that the emphasis would be on improving the quality of services is consistent with commentary from other writers. 20 A real focus is needed on addressing this aspect of inquiries, and we recommend both written and verbal communication to explain the purpose and process of an inquiry and what staff can reasonably expect to receive in terms of feedback and support. This information must be backed by an institutional commitment to honour the undertakings provided.
Health professionals are influenced by their perceptions of their organisation’s culture and may be sceptical of their institution’s intent for inquiries of this type. 12 Given the strength of participants’ emotional responses and their reports of the negative impact on team dynamics, we recommend careful consideration of facilitated team-based reflection within a supportive environment. 21 This should be accompanied by evaluation to ascertain whether this measure promotes understanding of inquiry findings and is beneficial for clinicians and teams. Organisations should use these inquiries to promote reflection on systems, learning from mistakes and open disclosure of inquiry findings to families. Supporting staff during inquiries may prevent them from exiting professions or services because of the compounding distress related to serious incidents.
Limitations
The transferability of our findings to other regions of New Zealand or other countries, and other mental health related incidents and types of inquiries, is limited by our modest sample size and our somewhat pragmatic process of identifying potential participants by incident reports from district health boards.
Conclusion
The clinicians in this study experienced inquiries as threatening, anxiety provoking and primarily concerned with protecting organisational interests. Written as well as verbal communication of the inquiry process and ensuring the dissemination of inquiry findings may enhance clinicians’ perceptions of inquiries, enable them to optimally participate and reflect on changes to clinical practice that could contribute to improving services. Support for clinicians individually and within their multidisciplinary teams during the inquiry process should be ensured by the commissioning agency.
Footnotes
Acknowledgements
The authors gratefully acknowledge the contributions of the research participants. Thank you to Ruth Allen for her assistance with the analysis.
Author Contributions
Lillian Ng was responsible for the acquisition, analysis and interpretation of data of the data. All authors contributed to the concept of the work, critically revising the content of the article and approving the final version. The authors are jointly responsible for the accuracy and integrity of the work.
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research was supported by a Faculty Research Development Fund award from The University of Auckland (L.N., grant number 3715260)
Data Availability
The authors report direct access to the study data. Access to transcripts of interviews with participants is ongoing and stored in accordance with New Zealand ethics committee guidelines. The analysed data is provided and can be accessed via supplementary material.