
Abstract
After prolonged periods of criminalisation, 20th and 21st century law reform has now moved abortion care closer to being regulated as health care in all Australian jurisdictions. However, no jurisdiction has yet tested the proposition that specific laws for abortion care are unnecessary. This article analyses the capability of health law, policy and ethics to regulate abortion comprehensively, without the need for either stand-alone laws or special provisions within health law. We examined this question in the South Australian context and concluded that the health framework provides the basis for equitable, safe and accountable abortion care that is also acceptable to the community.
Abortion is a common occurrence in women’s lives, and a significant activity in health care. 1 More effective contraceptive methods have assisted women and their partners to reduce the incidence of unplanned pregnancy in many countries, 2 but progress in women’s reproductive health and rights globally is neither comprehensive nor secure. 3 In all Australian jurisdictions, reform of abortion laws over the last 50 years has established the conditions for access to safe legal abortion care in most, but not all, circumstances. 4 Access problems remain, particularly with cost, location and restrictions on later abortion (variously specified as abortion after 14 to 24 weeks). 5
Recent decades have also seen the development of the modern Australian framework of general health law, policy and ethics (henceforth ‘the health framework’) which regulates the safety and standards of health care generally, creates conditions for equitable access to care and mandates appropriate accountability for health care providers. The suitability of this framework for regulating most abortion care is generally accepted in practice and recent legal reforms have largely brought abortion care into the medical domain, to be regulated as health care.
However, throughout Australia special laws governing abortion remain, in criminal law, abortion specific law and health law, such that abortion care has conditions placed upon it that do not apply to health care generally. Constraints are most frequently placed on later abortion, with various restrictions applying in all jurisdictions. 6 Abortion after 20 weeks is rare 7 and only occurs when fetal abnormality is diagnosed, in the aftermath of rape and reproductive coercion, or when there is serious illness or other complex social and health factors affecting pregnancy and care. 8
Legislative changes over the last 50 years, since South Australia (SA) became the first jurisdiction to liberalise access to abortion care, 9 have been in line with strong and growing public support for the availability of safe abortion care. 10 However, there is little evidence concerning Australian attitudes to later abortion. A News Poll conducted in 2004 and reported in The Australian newspaper found 15 per cent of respondents would approve abortion after 20 weeks ‘under any circumstances’ whereas the majority (61 per cent) would allow it ‘if it is proven the pregnancy will cause psychological or medical harm to the mother’, and 15 per cent would not allow it at all. 11 A survey conducted in 2008 asked respondents not if later abortion should be ‘allowed’ or ‘banned’, but rather whether doctors should be punished for providing later abortions in various circumstances. 12 Levels of support for doctors not to face sanctions varied from 78 per cent (if the circumstances were risks to the life of the woman or severe fetal abnormality), to 31 per cent (if the circumstance was simply the woman’s decision). However, in no circumstance was there a majority who believed that doctors should face sanctions.
In 2019, we undertook a public opinion survey of South Australian adults that assessed community acceptance of applying the health framework to decision-making about later abortion. 13 This study found strong majority support for later abortion care to be available ‘when the woman and her health care team decide it is necessary’ (63 per cent support in all circumstances, and a further 22 per cent in specified circumstances that cover the majority of later abortions). This phrase – ‘when the woman and her health care team decide it is necessary’ – describes the decision-making process that would apply under the health framework in the absence of specific abortion law, and the results indicate community acceptance of the health framework as an appropriate regulatory approach in the case of later abortion.
Currently in SA regulation of abortion remains in the criminal law and the maximum penalty for unlawful abortion is life imprisonment for both patient and doctor. 14 There are also important restrictions on practice, such as the decision regarding abortion being determined by two medical practitioners, 15 provided only in prescribed hospitals, 16 and available only to SA residents. 17 Current parliamentary debates in SA 18 and a recent review of abortion law and practice 19 have re-opened the question of how best to regulate abortion care, and whether special laws have a continuing purpose.
In this context, this study aimed to assess whether there is any continuing need for abortion-specific laws (in criminal or health law); or whether the framework of general health law, and its supporting body of regulations, policies, codes of conduct, professional ethics and clinical protocols (the health framework) is adequate to the task of regulating abortion care, including later abortion.
Method
This study involved a comparative assessment of the adequacy of the existing SA criminal law and the health framework, for the purposes of regulating abortion care. We sought to answer the questions ‘what regulation is required for high-quality, accountable abortion care?’ and ‘is there any aspect of abortion care that cannot be provided for under the framework of health law, policy and ethics?’ To answer the first question we analysed the
regulatory requirements for abortion care, categorised according to the relevant domains of the Australian Health Performance Framework. 20 We then compared the provisions of the current criminal law and health framework against the regulatory requirements to assess the adequacy of each, and to identify any gaps that would need to be addressed if the criminal law was repealed.
Results
Comparison of abortion care regulation under the health framework and criminal law
Comparison of SA criminal law and the health framework for regulation of abortion care.
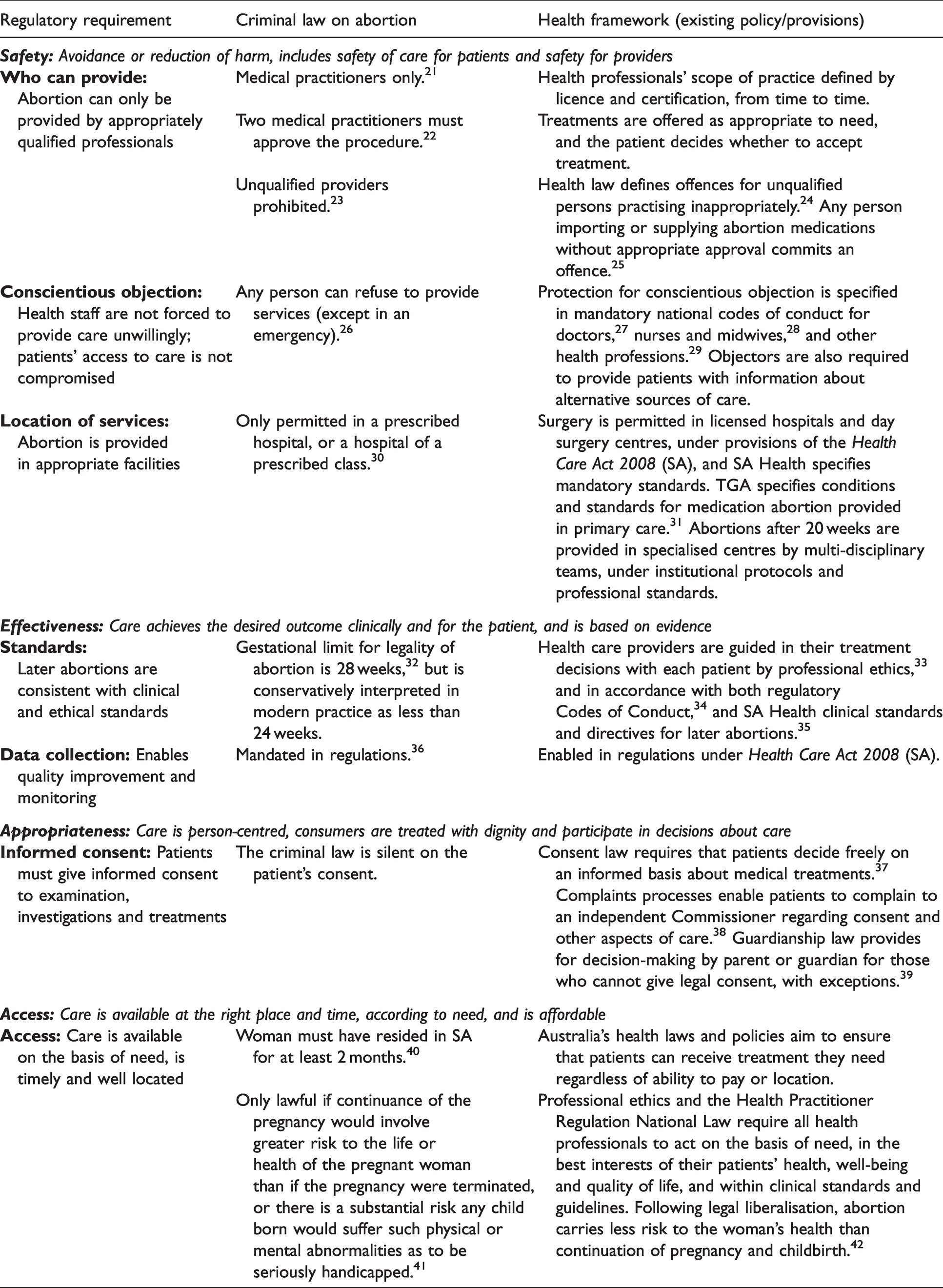
Safety for patients and staff: Qualified willing providers in appropriate facilities
Both SA’s current criminal law and the health framework prohibit the provision of abortion by anyone other than licensed medical practitioners. However, the health framework allows for change over time as medical technologies and the training of health professionals change, through a system of defined scopes of practice, specialised training for particular roles and procedures, and accreditation of individual practitioners accordingly. 43 Thus the criminal law relies simply on the (antiquated) category of profession, 44 whereas the health framework is more precise, reflective of current practice and flexible enough to incorporate future developments.
Protection of practitioners’ conscientious objection also applies in both regulatory systems. In the criminal law, any person can object to being involved in abortion care, without any specified obligation to the intending patient. Under the health framework, all health professionals have the right to exercise their conscientious objection to particular kinds of health care (such as abortion, assisted dying or IVF), but they also have obligations to ensure that their personal objection does not compromise patient access to care.
Both codes also require that abortion is provided in safe facilities. The criminal law specifies ‘prescribed hospitals’, reflecting clinical practice in 1969. This requirement is not compatible either with modern methods of abortion (including EMA which is otherwise provided by GPs in primary care and/or by use of telemedicine technology), nor with safety under pandemic conditions (when face-to-face consultations are more risky than telemedicine for staff, patients and the community). The health framework provides standards for hospitals, day surgery centres and GP facilities, and regulates telemedicine, all of which are clinically appropriate for abortion care.
Effectiveness: Care achieves the intended outcome clinically and for the patient, based on evidence
Perhaps the most difficult conflict arises where the criminal law proscribes later abortions based on length of gestation (currently interpreted as more than 24 weeks). The health framework requires that doctors offer appropriate treatments of benefit for the patient’s present and future health, and that patients decide whether to accept any offered treatment. Health professionals are obliged to offer all care on the basis of need, taking into account all relevant circumstances of the pregnancy and the patient, one of which is gestational length. The upper limit of weeks in SA criminal law distorts decision-making (for example, by forcing decisions based on fetal factors to be made before all diagnostic tests can be completed) and in some circumstances forces patients to seek treatment interstate or overseas.
Appropriateness: Person-centred care, dignity is respected and patients participate in care decisions
The criminal law is silent on informed consent, and some of its provisions are incompatible with the criterion of appropriateness. Specifically, the requirement in criminal law for two doctors to personally examine the patient and certify their approval of the abortion is not compatible with the dignity of patients, nor the requirement for informed consent because patient consent to examination by a second doctor is coerced. Further, the requirement for two doctors to approve the offering of treatment is inconsistent with patients’ rights to treatment on the basis of need, and in small communities it compromises their privacy rights. Patient consent is also not required for the mandated reporting of identifying information about the patient to the health department.
Access: Affordable care according to need, at the right place and time
The criminal law is silent on access but specifies conditions that limit access in relation to both need and the place and time at which care is provided (due to the prescribed hospital, examination and certification by two doctors, and SA residency requirements). Patients living in regional and remote areas are forced to travel long distances, making even public sector care expensive. Delays are incurred due to both supply restrictions in the prescribed public hospitals and the absence of EMA in primary care.
The health framework avoids unwarranted regulatory restrictions on access, but we note that access problems also have other causes, including inadequate training of health professionals and insufficient availability of an appropriately skilled workforce. 45
Our assessment confirms that the health framework addresses all the regulatory requirements for safe, effective, appropriate and accessible care, and covers all matters currently dealt with in the criminal law (albeit in different ways). However, the comparative analysis highlights several instances where the criminal law is inconsistent with the health framework, and tends to compromise modern approaches to safety, effectiveness, appropriateness and access, including in relation to conscientious objection, location of services, availability of medication abortion, abortion after 24 weeks, and access to care. Some of these problems have arisen because the criminal law has no ready mechanism for ‘future proofing’ to allow for clinical and technology developments. Others may be more correctly seen as intentional barriers against access to abortion care.
Other purposes of the criminal law and the question of later abortion care
Our analysis identified three purposes of the SA criminal law unrelated to the regulation of abortion as health care (the focus of our second research question). The first of those other purposes, served by the residency requirement, was to prevent Adelaide becoming ‘the abortion capital of Australia’, but this is no longer a concern following decriminalisation of abortion in all other jurisdictions.
The second purpose encoded in the SA criminal law was precisely to circumvent normal health care decision-making (ie, by the patient in consultation with health professionals), in favour of two doctors deciding for the patient. This goal has largely been discredited in light of increasing recognition of the human rights of women (and other pregnant people) 46 to bodily autonomy and self-determination (among other rights). 47 Its basis has also been invalidated in practice by development of the health framework, which provides an entitlement to equitable access to health care without discrimination on the basis of need. Professional ethics as well as health law require all health professionals to act on the basis of need, in the best interests of their patient’s health, well-being and quality of life, and within clinical standards and guidelines.
While the primacy of the patient’s decision is widely accepted in early pregnancy it is still contested as gestational length approaches the time at which the fetus could survive outside the body, and this third purpose of the 1969 law is the focus of current debates. Patients who undergo abortion after 20 weeks are invariably in distressing and complex circumstances. The decision of legislators as to a legal upper limit is one that must balance the benefits and harms of two alternatives: to negate the agency and needs of the patient, and the clinical judgment of health professionals, at a certain rule-of-thumb number of weeks, or to enable patients and their health care teams to make each decision based on the full complex range of factors in each pregnancy.
The medical consensus on the lower limit of potential survival of premature birth is generally agreed to be 23 to 24 weeks, assuming a healthy fetus and care in a neonatal intensive care unit. 48 However, the relevance of this consensus in the context of actual decisions about later abortion is not established, unless the possibility of the physical survival of the fetus is the only concern. We note that actual decisions are made case by case and, in the majority, the fetus is not healthy, because of fetal abnormalities, or factors in the pregnancy and/or the woman’s own health.
In the absence of specific legal limits on gestational age, each decision about later abortion care would be made by the patient and her health care team within institutional policy and practice guidelines. 49 The health framework provides three foundations to guide this decision-making.
First, the modern health framework acknowledges and codifies the rights of patients to make informed decisions, to give or withhold informed consent to any medical treatment, and to receive equitable access to care that is safe and of good quality. Under the health framework, the decision-making process needs to respect: the rights of those confronted with the need for a later abortion; their decision-making autonomy as people and as patients (with adequate time, information and advice, and without pressure); and the requirement for their informed consent to any treatment or investigation.
Second, the modern health framework requires health professionals to practise safely and ethically and protects their right to act in accordance with their conscience, but also places an obligation upon them to inform intending patients about alternative sources of care if they act on a conscientious objection and decline to provide certain care. 50 Health professionals make decisions about what treatments will be offered in accordance with their clinical judgement and their professional obligations and ethics. Just as women do not undergo later abortion without compelling reasons, health professionals also take this matter seriously. As in all health care, they must respond to the health and circumstances of the patient, ensure any treatment is clinically indicated and that informed consent is given.
Third, existing provisions in the health framework require both that individual professionals practise within their scope of competence and licensing, and practitioners with needed skills are included in care and decision-making. One corollary of this requirement is that women should not be subjected to, and health professionals should not impose, examinations, approvals, or gatekeeping by people not involved in the patient’s care. To do so violates patient autonomy and rights to privacy and timely care, and is often a barrier to therapeutic relationships and a waste of resources.
Thus, it is argued that decisions about investigations and treatments are best made by the patient and her health care team together; the team offer appropriate options, provide information and give advice as needed, and the patient decides to accept or reject those options, involving significant others as she considers appropriate. We suggest that this framework of ethical decision-making is more reliable for good practice than lists of indications (including gestational limits) encoded in law.
The capability of the health framework for this purpose is demonstrated in the experience of Victoria, where there are no absolute legal gestational limits (although after 24 weeks, two doctors must be involved in the decision), and yet there has been no sustained increase in the rates of later abortion. 51 It is not prohibition, but rather diagnoses and decisions made within the health care setting by those involved – patients and health professionals – that determine the need for later abortion. However, it should be noted that the actual number of later abortions conducted can also be influenced by problems in the supply of services. The availability of a skilled, accredited and willing workforce continues to be influenced by shortcomings in the training of doctors in procedures for later abortion, and the chilling effect of the history of criminality on the numbers who decide to take on this work. This problem may be a factor in Victoria and elsewhere.
Discussion and conclusion
Our analysis shows that there is no compelling case for a continuation of specific laws to regulate abortion care, 52 and further that they will almost inevitably cause unforeseen access and quality problems because they cannot allow for medical and other advances affecting abortion care.
We suggest that the only remaining barrier to the repeal of all specific abortion laws is the influence of those who oppose abortion care per se, based on their personal views of the moral status of abortion and their conviction that those views should be enforced on others by the State. Opponents of safe abortion care still seek to maintain the framing of abortion as a matter for legal prohibition or exceptional restriction, based on the concept of fetal rights, which they assert should take precedence over the human rights of women, particularly in relation to later abortion.
However, public opinion research indicates that the community is generally more comfortable framing later abortion care as health care rather than as a more abstract contest of rights. That is, these decisions are best accepted when they are made case by case and day by day, within the safety net of the health framework that brings to bear the full spectrum of health law, policy and ethics. This level of community acceptance of regulation under the (nationally consistent) health framework supports the proposition that the repeal of specific abortion laws is a feasible policy option in the Australian democracy.
Significant development in the health framework in recent decades has now codified the regulatory requirements for safe, effective, appropriate and accessible abortion care, including the accountabilities of health care providers. Abortion care is safe and effective in practice, but access problems remain. Decriminalisation is necessary but not sufficient to overcome the chilling effects of the long criminal history of abortion, seen in problems in the training of health professionals, the standing of abortion providers among their peers, the application of conscientious objection provisions 53 and the size of the available workforce for abortion care. 54 While there is evidence of progress in these workforce factors, access to care is also compromised in several jurisdictions by the decisions of public hospitals not to provide abortion care, so that patients are forced into the private system. 55 We suggest that decriminalisation of abortion in Australia will over time enable the further policy and service delivery changes within the health system that are needed to ensure that abortion care in Australia is also timely, affordable, and accessible in practice.
This study supports the conclusion that there is no continuing role for specific laws on abortion care, and that if the existing laws were simply repealed (excepting only those that regulate the actions of opponents to safe abortion) the delivery of abortion care, including for later abortion, would be able to proceed under normal health care frameworks, best summarised as when the patient and her health care team decide that it is necessary.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosure
The authors are volunteer members of the SA abortion action coalition, which advocates for better access to abortion care and for law reform.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
1
See, eg, Suzanne Belton, Felicity Gerry, and Virginia Stulz, ‘A Reproductive Rights Framework Supporting Law Reform on Termination of Pregnancy in the Northern Territory of Australia’ (2018) 6(2) Griffith Journal of Law & Human Dignity 25, 28.
2
See Amy Deschner and Susan A Cohen, ‘Contraceptive Use is Key to Reducing Abortion Worldwide’ (2003) 6(4) Guttmacher Policy Review 7.
3
See Mahmoud Fahmy Fathalla, ‘Safe Abortion: The public health rationale’ (2020) 63 Best Practice & Research Clinical Obstetrics & Gynaecology 2.
4
See, eg, Abortion Law Reform Act 2008 (Vic); Termination of Pregnancy Act 2018 (Qld); Abortion Law Reform Act 2019 (NSW).
5
The NT imposes further restrictions post 14 weeks (see Termination of Pregnancy Law Reform Act 2017 (NT)), while Victoria imposes further restrictions post 24 weeks (see Abortion Law Reform Act 2008 (Vic)).
6
For a concise summary of such laws see South Australian Law Reform Institute (SALRI), Abortion: A Review of South Australian Law and Practice (Report No 13, October 2019, 88–9). Note: While the ACT places no specific upper limits on lawful abortion, the ACT retains the offence of child destruction (Crimes Act 1900 (ACT) s 42), which arguably creates an implicit upper gestational limit upon lawful abortions: see Mark J Rankin, ‘The Offence of Child Destruction: Issues for Medical Abortion’ (2013) 35(1) Sydney Law Review 1.
7
Abortions after 20 weeks represent 2 per cent of all abortions in SA: see South Australian Abortion Reporting Committee, Annual Report for the Year 2018 (November 2020) 8.
8
9
See Criminal Law Consolidation Act 1935 (SA) s 82A.
10
See Sarah Cameron and Ian McAllister, ‘Trends in Australian Political Opinion: Results from the Australian Election Study 1987–2019’ (Monograph, School of Politics & International Relations, ANU College of Arts & Social Sciences, December 2019) 117.
11
Patricia Karvelas, ‘Majority stays pro-choice’, The Australian (Sydney, 29 December 2004) 2, cited in Katherine Betts, ‘Attitudes to Abortion: Australia and Queensland in the Twenty-First Century’ (2009) 17(3) People and Place 25.
12
See Lachlan J de Crespigny et al, ‘Australian attitudes to early and late abortion’ (2010) 193(1) Medical Journal of Australia 9.
13
Monica Cations, Margaret Ripper and Judith Dwyer, ‘Majority Support for Access to Abortion Care including Later Abortion in South Australia’ (2020) 44(5) Australian and New Zealand Journal of Public Health doi: 10.1111/1753-6405.1299.
14
Criminal Law Consolidation Act 1935 (SA) s 81.
15
Ibid s 82A(1)(a).
16
Ibid.
17
Ibid s 82A(2).
18
In terms of legislative activity, the SA Parliament has passed the Health Care (Safe Access) Amendment Act 2020 (SA), which creates (through amendments to the Health Care Act 2008 (SA)) health access zones around protected premises that provide abortion care. The Termination of Pregnancy Bill 2020, which decriminalises abortion, was passed by the SA Parliament in March 2021.
19
See SALRI Report (n 6).
20
See National Health Information and Performance Principal Committee, The Australian Health Performance Framework 2017 (September 2017).
21
Criminal Law Consolidation Act 1935 (SA) s 82A(1)(a).
22
Ibid.
23
Ibid s 81(2).
24
See, eg, various offences under Health Practitioner Regulation National Law (South Australia) Act 2010 (SA).
25
See various offences under Therapeutic Goods Act 1989 (Cth).
26
Criminal Law Consolidation Act 1935 (SA) ss 82A(5)-(6).
27
Medical Board of Australia, Good Medical Practice: A code of conduct for doctors in Australia (March 2014) cl 2.4.6.
28
Nursing and Midwifery Board of Australia, Code of Conduct for Nurses (March 2018) cl 4.4(b).
29
See, eg, Pharmacy Board of Australia, Code of Conduct for Pharmacists (March 2014) cl 2.4(f) & 2.4(g).
30
Criminal Law Consolidation Act 1935 (SA) s 82A(1)(a).
31
32
Criminal Law Consolidation Act 1935 (SA) s 82A (7)-(8).
33
See, eg, Australian Medical Association (AMA), AMA Code of Ethics 2004 (Revised 2016).
34
Codes of Conduct establish standards for doctors, nurses and midwives, and all health professionals: see, eg, Medical Board of Australia (n 27), Nursing and Midwifery Board of Australia (n 28), Pharmacy Board of Australia (n 29).
35
See SA Health, Standards for the Management of Termination of Pregnancy in South Australia (March 2014); SA Health, South Australian Perinatal Practice Guideline: Perinatal Loss (2014).
36
See Criminal Law Consolidation Act 1935 (SA) s 82A(4); Criminal Law Consolidation (Medical Termination of Pregnancy) Regulations 2011 (SA).
37
See Consent to Medical Treatment and Palliative Care Act 1995 (SA).
38
See Health and Community Services Complaints Act 2004 (SA).
39
See Guardianship and Administration Act 1993 (SA).
40
Criminal Law Consolidation Act 1935 (SA) s 82A(2).
41
Ibid s 82A(1)(a).
42
See, eg, Elizabeth G Raymond and David A Grimes, ‘The comparative safety of legal induced abortion and childbirth in the United States’ (2012) 119(2) Obstetrics & Gynecology 215.
43
Under this framework, and absent legal barriers, it is likely that in future accredited nurse practitioners and Aboriginal Health Practitioners with prescribing rights will be able to prescribe Early Medication Abortion (EMA) and supervise its use, as is common practice internationally.
44
Perhaps legislators who framed the 1969 law were concerned about high morbidity and mortality from illegal abortion, often provided by non-medical practitioners. However, following legal liberalisation, there has been no market for unqualified abortion providers: see World Health Organization, Safe abortion: technical and policy guidance for health systems (Department of Reproductive Health and Research, 2nd ed, 2012) 90; Human Rights Law Centre, Modernising NSW’s Archaic Abortion Laws: Submission on the Reproductive Health Care Reform Bill 2019 to the NSW Parliament Standing Committee on Social Issues (August 2019) 6.
45
SALRI Report (n 6) 167–8.
46
People undergoing gender transitions, non-binary and intersex people can also become pregnant and need abortion care. For this reason, the term ‘pregnant person’ is now used in some legislation.
47
A detailed exploration of the rights argument is beyond the scope of this article. For a ground-breaking discussion of the human rights violations that occur as a result of restrictive abortion laws see Rosalind Petchesky, Abortion and Woman’s Choice: The State, Sexuality, and Reproductive Freedom (Longman, 1984). See also Christine Forster and Vedna Jivan, ‘Abortion law in New South Wales: Shifting from Criminalisation to the Recognition of the Reproductive Rights of Women and Girls’ (2017) 24 Journal of Law and Medicine 850, 854–5.
48
See, eg, Noel French, ‘Consensus Statement on Perinatal Care’ (2007) Journal of Paediatrics and Child Health 492.
49
In the SA case, the removal of a legal upper gestational limit would trigger the updating of mandatory policy guidelines published by the Department of Health and Wellbeing.
50
See Medical Board of Australia (n 27), Nursing and Midwifery Board of Australia (n 28), Pharmacy Board of Australia (n 29).
51
52
However, we note that laws to prohibit the harassment or intimidation of patients and staff at abortion clinics is still needed, due to continuing opposition to the availability of safe legal abortion by a very small proportion of the Australian community (4 to 5 per cent in the most recent Australian Election Studies: see Cameron and McAllister (n 10) 117), and the willingness of a small proportion of that group to act on their views in a harassing or intimidating way. All jurisdictions other than WA have now enacted safe access zone legislation to address this issue, and there is currently a Bill before the WA Parliament to that end: see Public Health Amendment (Safe Access Zones) Bill 2020 (WA).
53
Louise Keogh et al, ‘Conscientious Objection to Abortion, the Law and its Implementation in Victoria, Australia: Perspectives of abortion service providers (2019) 20 BMC Medical Ethics doi: 10.1186/s12910-019-0346-1.
54
SALRI Report (n 6) 167–8.
55
For example, in Queensland the Health Department issued an instruction to regional health services to respond to decriminalisation by establishing a pathway to care for patients in their regional catchments, either by establishing services within hospitals or financing care in the private sector (Children by Choice, Abortion in Queensland FAQ (Web Page, 2019) ![]() .
.