
Abstract
Despite the billions of dollars invested in improving Indigenous health and wellbeing outcomes in Australia, there is little evidence of program effectiveness to inform policy and practice. The deficiency of evaluations is problematic. Critical to this process is the effective engagement of commissioners with Indigenous peoples, which is not well documented. Currently, there is scant evidence on modes of commissioning practices used. This scoping review will aim to identify the spectrum of commissioning practices used when evaluating Indigenous health and wellbeing programs in Australia, codifying them into a model set. Documents (between 2008 and 2020) will be retrieved from Scopus, Proquest, Informit, Google Scholar and via a web-based search that refers to the commissioning of Indigenous health and wellbeing program evaluations in Australia, New Zealand, Canada or the United States. Importantly, the research team is Indigenous-led and the project’s governance, quality and translation framework will be informed by a project advisory group, including Indigenous associates. This will be the first scoping review globally to identify practices used to commission Indigenous health and wellbeing program evaluations. Results will be utilised to strengthen the commissioning practices of Indigenous health and wellbeing programs in Australia and overseas.
• Calls for evidence-based Indigenous health and wellbeing policy development have increased over the last few decades. • One way of generating evidence to inform this policy and practice is through funded program evaluation.
• This review considers what little is known about the commissioning processes for Indigenous health and wellbeing evaluations. • To date there are no developed models for commissioning Indigenous health and wellbeing programs. This will be the first step in their development to assist commissioners, evaluators or services providers when undertaking commissioning.What we already know:
The original contribution the article makes to theory and/or practice:
Introduction
The colonised experience of Aboriginal and Torres Strait Islander peoples, the Indigenous people of the country now called Australia, is often problematised via the presence of inequitable health outcomes, including complexities associated with morbidity and premature mortality (National Indigenous Australians Agency, 2023). The Aboriginal and Torres Strait Islander peoples’ experience is typically accompanied by a narrative which argues that substantial funds have been ‘invested in’ improving health with mixed outcomes or benefits to the wider society (Steering Committee for the Review of Government Service Provision, 2017).
Over several decades, calls for evidence-based health and wellbeing policy development have increased, particularly for policies that impact Indigenous peoples (Coalition of Peaks, 2023; Dwyer, 2004; Fredericks, Adams, & Edwards, 2011; Head, 2010; Larkin, 2006; Lowitja Institute, 2022; Productivity Commission, 2021). These have principally been to determine whether these policies attain their stated goals and, if there have been unintentional consequences, to determine to what extent these by-products have been positive or negative (Oliver et al., 2019). One way to generate evidence to inform policy and practice is for program commissioners and service providers to evaluate funded programs (Bowman et al., 2015; Broc et al., 2019; James, 2013; Maddox et al., 2021; Weaver & Cousins, 2007). In the case of complex evaluations in political contexts, it is suggested this should be with iterative, flexible approaches that consult with, and respond to, key stakeholders throughout the evaluation process so as to benefit the quality of findings (Stack et al., 2018). This includes evaluations of Indigenous health and wellbeing programs.
The Need to Consider the Complexity Surrounding Indigenous Health and Wellbeing Program Evaluations From Their Inauguration
Indigenous health and wellbeing program evaluations are inherently ‘situated within complex systems and influenced by their social, political, historical, and cultural contexts’ (Maddox et al., 2021, p. 333), which means their effectiveness rests on their sensitivity to cultural circumstances (Chouinard & Cram, 2019; Gollan & Stacey, 2021). Considering associated Indigenous contexts from the point of commissioning to evaluation conclusion facilitates the incorporation of local circumstances, standpoints and knowledges within the evaluation from the initiation of evaluation, making it more likely that evaluation outcomes consider the ideals of local Indigenous peoples and their communities (LaFrance & Nichols, 2008; Maddox et al., 2021). This is especially important as evaluations commissioned without considering community contexts may be culturally unsafe or inappropriate, as they can enact dominant Euro-Celtic standpoints and practices, further subjugating Indigenous practices and knowledges (Gollan & Stacey, 2021; Maddox et al., 2021; Rigney, 1999). Finally, this lack of consideration may ultimately result in reduced community participation, a lack of methodology and reduced data reliability and validity (Maddox et al., 2021). These deficiencies in turn, have been suggested to inevitably lead to a failure to truly evaluate program and policy achievements (Williams, 2018).
Commissioning in Practice
In Australia, Canada, New Zealand and the USA, substantial investments from national and state/provincial/regional governments have been made in Indigenous health and wellbeing programs, which are ostensibly aimed at achieving health parity between Indigenous peoples and other people in their respective jurisdictions (Allard-Côté et al., 2016; Council of Australian Governments (COAG), 2020; Government of Canada, 2021; Productivity Commission, 2020b; Steering Committee for the Review of Government Service Provision, 2017). Yet only a small number of Aboriginal and Torres Strait Islander programs are evaluated, and fewer still from Indigenous peoples’ perspectives (Fredericks et al., 2017; Hudson, 2017; Williams, 2018). Within this context, Indigenous leaders have been calling for opportunities to influence decision-making processes within the health system and across sectors and for the commissioning of health and wellbeing programs to reflect their needs, priorities and views on program design, delivery and evaluation (Aboriginal & Torres Strait Islander Social Justice Commissioner, 2009; Gibbs, 2020; Lowitja Institute, 2020; Malezer, 2013; National Aboriginal Community Controlled Health Organisation (NACCHO), 2022; Reconciliation Australia, 2016). This call necessitates better designed and evaluated programs to benefit Indigenous populations and achieve the Closing the Gap (CTG) targets. This is supported by recommendations from the Productivity Commission for government and non-government agencies to partner with Indigenous peoples to ensure that programs and their evaluation capture Indigenous interests (Productivity Commission, 2012). It also aligns with Articles 18–21 and 23 in the United Nations Declaration on the Rights of Indigenous Peoples (United Nations, 2009), which outline the right of Indigenous peoples to act as full and effective participants in the decision-making processes that affect their health, economic and social wellbeing. However, recent scholarship points to the dichotomous relationship between what funders want and what Indigenous communities need when evaluations are being commissioned (Finlay et al., 2021). Ultimately if robust evidence is generated from this project, that meets the needs of stakeholders, it may then be applied to further improve policy and practice.
The commissioning of program evaluations tends to be conceptualised as a series of activities or steps (Finlay et al., 2021). Typically, the process begins when a funding body initiates an evaluation and ends with the final reporting of the evaluation findings. From the moment the evaluation is initiated until its completion, the commissioner of evaluation is central to the way program evaluations are carried out and the quality of evidence that is generated (Finlay et al., 2021). The commissioning process often sets the budget, selects the evaluators, and places parameters around the evaluation aims, objectives and data collection methods. These pre-determined variables, set the stage for the cultural safety and power dynamics of the evaluation (Finlay et al., 2021), or lack thereof for participating individuals and communities. This process can be particularly problematic with Indigenous evaluations, which are typically considered a threat to Indigenous peoples. This is firstly due to the historical role of research in the colonisation of Aboriginal nations (Andersen & O'Brien, 2017; Fredericks, 2008; Katz et al., 2016; Moreton-Robinson, 2021; Rigney, 1999; Walter & Andersen, 2016) and secondly, because evaluative research methodologies can be grounded in ‘world views’ which are hostile towards non-Eurocentric belief systems or do not have methods designed around other ways of knowing (Martin & Mirraboopa, 2003; Moreton-Robinson, 2021; Rigney, 1999; Smith, 2021). However, this is changing as evaluation gradually comes to be viewed as a resource that can be utilised for self-determination, advocacy and cultural-linguistic maintenance (Blair, 2015; Katz et al., 2016; Kovach, 2021; Wilson, 2008) and may further change through decolonisation.
The Decolonisation of Evaluation Commissioning
Decolonising denotes the dismantling of the legacy of colonisation and coloniality (Auriacombe & Cloete, 2019; Laenui, 2000; Sherwood, 2009), where coloniality is defined as the established (matrixes or) ‘patterns of power’ (Maldonado-Torres, 2007, p. 243), which are the result of colonialism (Mignolo & Walsh, 2018). These have come to define ‘culture, labour, intersubjective relations, and knowledge production well beyond the strict limits of colonial administrations’ (Maldonado-Torres, 2007, p. 243), so that they colour all aspects on individuals’ lives (Mignolo & Walsh, 2018). Decolonisation does not infer the ‘absence of coloniality’ (Mignolo & Walsh, 2018, p. 81), rather it entails active, continuous, but sometimes indirect, movement towards the ‘possibility of other modes of being, thinking, knowing, sensing and living; that is, an otherwise in plural’ (Mignolo & Walsh, 2018, p. 81; Muller, 2023). It is additionally ‘a process that requires the positioning of oneself in history and the recognition of ideas and assumptions that have informed one’s worldview’ (Sherwood et al., 2011, p. 194). In essence, it doesn’t just change the content of the discussion, as de-westernisation does, it changes its terms or provisions (Mignolo & Walsh, 2018) and our selves.
In the context of evaluations or research praxis, this has been suggested to be actions guided by transparent consultation, principles (i.e. researcher responsibility), confidentiality, respect for and recognition of rights, consent, safety, collaboration, reflection and mutual benefits (Brant et al., 2023; Fredericks et al., 2011; Herman, 2018; Muller, 2007; Sherwood, 2010; Sherwood & Edwards, 2006; Smith, 2008; Tunón et al., 2016). Evaluative research with the consent of the community and individuals who participate aligns with Indigenous epistemologies and the political realities of Indigenous lives. This approach also respects social and communal knowledge as well as individual knowledge, making it consistent (Brant et al., 2023; Cajete, 2017; Chilisa, 2012; Rigney, 1999). Put simply, it is the evaluations that honour the principles of conducting research with and for Indigenous peoples and which move away from the harmful and unethical practices of the past, where the word ‘research’ became ‘one of the dirtiest words in the Indigenous world’s vocabulary’ (Smith, 2021, p. 1). It is changing the way of thinking to ‘give First Nation people a voice’ (Radcliffe in Gollan & Stacey, 2021, p. 8), through meaningful engagement, reciprocity, the recognition of diversity and the incorporation and utilisation of Indigenous knowledge systems (Andersen & O’Brien, 2017; Bower et al., 2015; Moreton-Robinson, 2021).
It is well documented that the success of evaluations is determined by Indigenous peoples’ engagement throughout all stages of the evaluation, from identifying the need for an evaluation to the final reporting (Auditor-General, 2019; Better, 2022; Bowman et al., 2015; Productivity Commission, 2020). This is also evidenced in the numerous human research ethics processes and other documents that describe the best practice principles for evaluating Indigenous health and wellbeing programs (Centre for Social Research and Evaluation: Te Pokapü Rangahau Arotake Hapori, 2004; Williams, 2018). For example, in New Zealand, evaluations involving Māori should be conducted using the principles outlined in ‘Nga Ara Tohutohu Rangahau Māori Guidelines for Research and Evaluation with Māori’ (Centre for Social Research and Evaluation: Te Pokapü Rangahau Arotake Hapori, 2004). In Australia, evaluations are guided by two sets of research guidelines, inclusive of evaluation: the National Health and Medical Research Council’s (NHMRC) (2018) Ethical conduct in research with Aboriginal and Torres Strait Islander Peoples and communities: Guidelines for researchers and stakeholders 2018 and the Australian Institute of Aboriginal and Torres Strait Islander Studies (AIATSIS) (2020) AIATSIS Code of Ethics for Aboriginal and Torres Strait Islander Research. More recently, we have seen the development of Indigenous and cultural evaluation frameworks by other organisations in Australia – such as the National Indigenous Australians Agency (Department of the Prime Minister and Cabinet, 2018), Productivity Commission (Productivity Commission, 2020b), Lowitja Institute (Kelaher et al., 2018) and the Australian Evaluation Society (Gollan & Stacey, 2021) – all of which offer additional principles and further guidance about pursuing Indigenous evaluations.
What is unclear is how and to what extent best practice principles, including effective Indigenous engagement, are being considered or supported in the commissioning of program evaluations, if at all, as there is currently no research on this topic. This gap in knowledge makes it difficult for commissioners to apply best practices in procuring evaluation tenders for Indigenous health and wellbeing programs. It also impedes the development of an evidence base to inform policy decisions regarding strategic financial investments to improve Indigenous health outcomes. With better-designed programs and evaluations, and improved commissioning practices, there is an increased likelihood of achieving improved Indigenous health outcomes.
The first step in understanding the commissioning practices of Indigenous health and wellbeing evaluations is to undertake a scoping review of the literature from Australia, New Zealand, USA and Canada. This protocol outlines the scoping review methodology that will be used to fill in this important knowledge gap.
Objectives
The objectives of the scoping review are: 1. To systematically search the literature to identify government and non-government agencies commissioning practices of Indigenous health and wellbeing program evaluations, and characterise commissioning practices according to Indigenous best practice principles, 2. To review commissioning practices and construct models that represent the range of commissioning practices using Indigenous best practice principles and 3. To identify knowledge gaps in the commissioning of Indigenous health program evaluations.
Context
This scoping review was initiated to identify existing commissioning models of evaluation commissioning as part of a broader project considering the implications of modes of evaluation commissioning of Aboriginal and Torres Strait Islander Health and Wellbeing Programs. A team of eight researchers led by Yorta Yorta woman Dr Summer May Finlay will conduct this scoping review with guidance from a stakeholder project advisory group (which has strong Indigenous representation from across government and the Aboriginal community-controlled sectors), in collaboration with the research team of which over 50% identify as Indigenous. Foley’s (2003) Indigenous standpoint theory, along with other seminal Indigenous standpoint theory work by Moreton-Robinson (2021) and Nakata (2007), will be used as the lens to assist with interpreting the results. This is because central to this review and all aspects of the broader research project is the adoption of an Indigenous standpoint.
Indigenous standpoint theory recognises that historical knowledge remains prejudiced by Eurocentric or colonial perspectives, which restrict Indigenous voices, therefore, it opposingly privileges Indigenous voices and subjectivities (Henry & Foley, 2018; Hokowhitu et al., 2020; Moreton-Robinson, 2021; Nakata, 2007; Rowe et al., 2015; Walker et al., 2013). It ‘is research by, with and for Indigenous peoples, not just “about” Indigenous peoples’ (Henry & Foley, 2018, pp. 221–222), which means it is built on reciprocal respect and understanding of culture and identity (Bessarab & Ng’Andu, 2010; Bishop, 2008; Bower et al., 2015; Rogers et al., 2017). It utilises Indigenous ontology, or beliefs about existence and reality, an epistemology founded on an Indigenous perspective of what counts as knowledge and axiology grounded in those cultural values and a methodology influenced by these three factors (Denzin et al., 2008; Durie, 2004; Foley, 2018; Henry & Foley, 2018; Moreton-Robinson, 2021; Nakata, 2007; Rigney, 1999). With this in mind, throughout the production of this scoping review, Indigenous researchers and the project advisory group will play key roles in ensuring reciprocal appreciation for, and understanding of, Indigenous culture and identity is paramount in the way this review is presented, in the research questions asked and in interpretations of results (Chilisa, 2012; Fredericks, 2010; Hokowhitu et al., 2020; Walter & Andersen, 2016).
This article reports on the methods used to conduct this review.
Methods
Funding Agency
This study was funded by the National Health and Medical Research Council of Australia (GNT1165913), with the aim of strengthening the commissioning practices of Indigenous health and wellbeing programs in Australia.
Study Design
A scoping review will be conducted following the methodological framework of Arksey and O’Malley (2005) and Levac et al.’s (2010) methodological enhancements. Distinct from systematic literature reviews which assess the quality of studies (Arksey & O'Malley, 2005; Levac et al., 2010), scoping reviews clarify key concepts in the literature and the extent to which they are reported, identify key characteristics or factors related to a concept and uncover knowledge gaps to inform future research (Munn et al., 2018; Peters et al., 2020). As to date, there has been no formal synthesis of commissioning practices or models applied to Indigenous health program evaluation; researchers feel this study best aligns with the aim of a scoping review to clarify concepts (such as commissioning models) in the literature.
Four academic databases will be searched, however, given the focus of this study, grey literature will also be included (i.e. print and electronic documents produced by government, academic and industry sources that are not controlled by commercial publishers). This may include evaluation studies published by consultants as reports or policy papers on the websites of government departments (Lawrence et al., 2014). The websites of commissioning organisations will also be searched from a starter list of organisations identified by the research team, project advisory group and their respective professional networks. We expect to find tender documents, call for proposals, principles and frameworks and gain a sense of timelines and conditions in the funding agreements and where and how Indigenous peoples are engaged in the commissioning process. Research organisations and their electronic databases that publish journal articles, research reports, evaluation reports and policy directives relevant to the topic will also be reviewed (e.g. Australian Indigenous Health Info net).
The scoping review framework has six stages: (1) identifying the research question, (2) identifying relevant studies, (3) selecting studies, (4) charting the data, (5) collating, summarising and reporting the results and (6) consultation. The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) extension for scoping reviews and the PRISMA flow diagram will be used to guide the conduct and reporting of the scoping review (Tricco et al., 2018). This review is the first of its kind and will identify knowledge gaps in commissioning practices of Indigenous health and wellbeing program evaluations, with the aim of informing future health policy and practice.
Stage 1: Identifying the Research Question
This scoping review will be the first step to characterising the commissioning practices of Indigenous health and wellbeing program evaluations. It seeks to answer the following question: What practices are used by government and non-government agencies to commission Indigenous health and wellbeing program evaluations and how are they aligned with Indigenous best practice principles?
Stage 2: Identifying Relevant Studies
The following databases will be systematically searched: Scopus, Proquest, Informit and Google Scholar. Grey literature will be retrieved by searching the world-wide web via the Google search engine. Following Pham (2014), we aim to screen the first 100 hits from the Google search as further screening is deemed unlikely to yield many more relevant documents (Stevinson & Lawlor, 2004). We anticipate the search will lead to reports, policy submissions and potentially websites with links to commissioning documents. Supplementary documents, including websites to relevant commissioning documents, will be obtained by discussing the scoping review search strategies with the project advisory group at scheduled advisory meetings and then following up with individual advisory group members. Research team members will utilise their professional networks to obtain reports, policy submissions and websites that may not surface in the database searches. Finally, we will circulate a list of documents to advisory group members and colleagues to see whether any grey literature documents are missing.
Specific search strategies will be designed for each database. Separate search strings will be designed to capture terms related to: ‘Indigenous’, ‘evaluation’, ‘program’, ‘commissioning’ and ‘health’ related documents. Following a period of trialling the search, with advice from a research librarian, an optimal set of search strings will be generated. We anticipate that the search strategy will be iteratively refined. Documents will be downloaded, imported and stored in Covidence, the web-based software platform.
Stage 3: Study Selection
In the first step of stage 3, using Covidence, duplicate documents will be removed and full-text documents retained for the second step of screening. Subsequently, all titles and abstracts will be screened independently by two reviewers, based on the eligibility criteria below. Where no abstracts exist, such as is the case for some grey literature, full-text scanning will occur. Any discrepancies between the reviewers will be resolved through discussion and, if needed, moderated by a third reviewer. In the second step, documents meeting the eligibility criteria will be included in the full-text review. Both reviewers will independently assess the full-text documents, with disagreements resolved through discussion and moderation by a third reviewer, if needed. As per Levac et al.'s (2010) enhancement, the two reviewers (initials blinded) will meet weekly at the beginning, midpoint and final stages of the study selection process to discuss any challenges that arise in the study selection process. We are open to the study selection process occurring iteratively with the literature search and initial review of documents used to refine the search strategy.
Eligibility Criteria
Documents meeting the following criteria will be included in the review: English-based studies from 2008 to 2020 that refer to the commissioning practices of Indigenous evaluations of health or wellbeing programs for Indigenous populations in Australia, New Zealand, Canada or the USA. In this manner, the search will identify practices that can inform Australia’s ‘Closing the Gap’ health policy, initiated in 2008 (Australian Government, 2008), a focus of the broader funded research grant. Limiting the search to August 2020 coincides with the release of Australia’s Indigenous Evaluation Strategy (Productivity Commission, 2020a), which provides a whole-of-government framework for selecting, planning, conducting and using evaluations of policies and programs affecting Indigenous peoples in Australia. The search was limited to 2020, with the knowledge that very recent advancements associated with the development of Australia’s Indigenous Evaluation Strategy and National Indigenous Australians Agency (Department of the Prime Minister and Cabinet, 2018) Indigenous Evaluation Framework may artificially skew the review findings. Another review will be conducted at a later date to capture these developments. The search will be restricted to Indigenous populations in developed countries to capture commissioning practices within countries with similar histories of colonisation and subsequent policies impacting Indigenous peoples in Australia.
Documents will need to refer to one or more aspects of the commissioning of an evaluation, that is, refer to the terms of reference for an evaluation, process/criteria for selecting an evaluator, contractual obligations, how variations to an evaluation protocol are managed, how the commissioned evaluation was conducted in relation to commissioner expectations/contractual arrangements, or express a viewpoint about the commissioning practices of Indigenous health and wellbeing evaluations. Health and wellbeing programs in this scoping review will be restricted to programs with a focus on health promotion/social determinants of health and a non-clinical focus.
Stage 4: Charting the Data
Data extraction tool that includes definitions of best practice principles and extraction guidance.
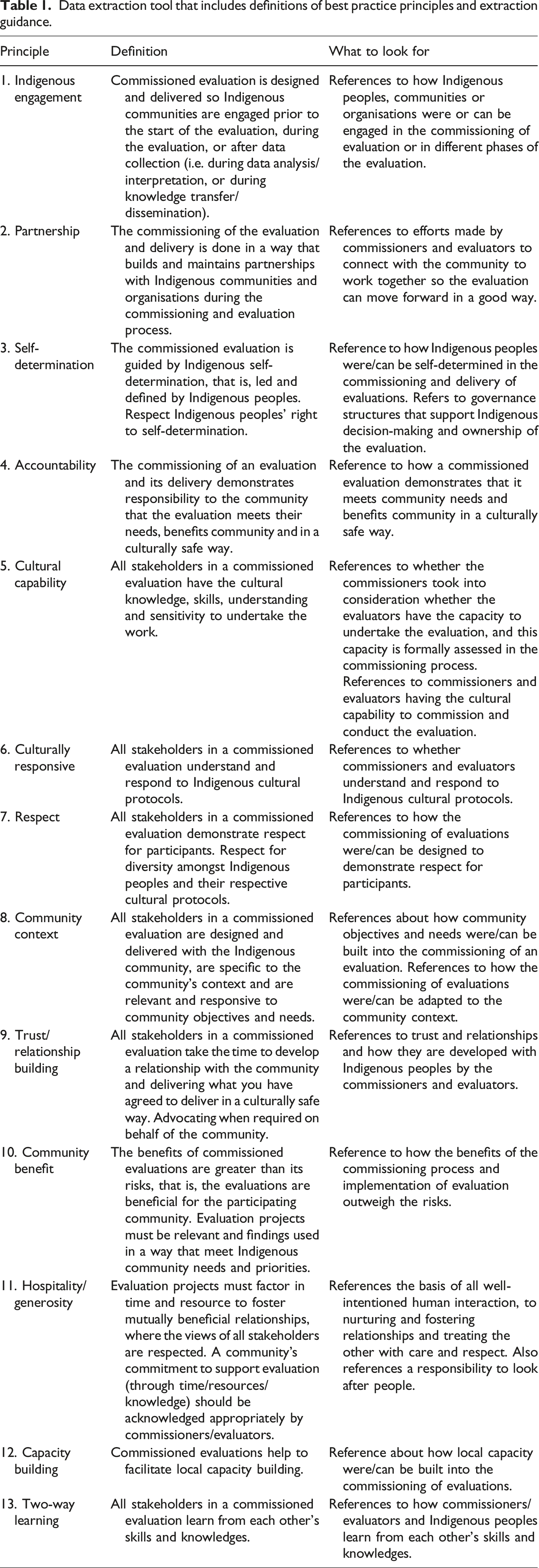
Throughout the review, each primary document will be coded for the presence, or absence, of these principles using NVivo qualitative software. MS Excel will be used to capture the following descriptive characteristics from primary documents: country, document type, purpose of document and whether it is empirical or not. The extraction of data from primary documents will be Indigenous-led with support from a second research team member. Primary document authors will not be contacted to provide additional information. At this stage, we do not anticipate undertaking a critical appraisal of the primary documents as we anticipate the documents will be policy and practice-based.
Stage 5: Collating, Summarising and Reporting the Results
Document characteristics will be extracted and analysed using frequencies, with each primary document coded according to the 13 principles. Given the interdependence of the best practice principles (e.g. self-determination and Indigenous participation), we anticipate using simultaneous or co-occurrence coding (Saldana, 2012). This qualitative coding procedure is appropriate when a segment of text suggests multiple meanings that justify the use of more than one code. Simultaneous coding will also allow for the more complex social interactions that would be expected between commissioners, evaluators and Indigenous community members or service providers in the evaluation of Indigenous health and wellbeing programs. The simultaneous coding of documents using principles, with consideration to their presence or absence, may facilitate the identification of commissioning models – the anticipated output of the synthesis process. Notes for each primary document will be summarised in memos and contribute to the two data analysts building consensus on the development of the commissioning models, through a synthesis of the included documents. We anticipate that commissioning models identification will be an iterative process between the two researchers with ongoing feedback from project stakeholders used to refine the commissioning models. The commissioning models will be visually represented according to the best practice principles.
Stage 6: Consultation Exercise
As noted earlier, the scoping review will be guided by the project advisory group and research team (‘project stakeholders’) and underpinned by Indigenous research methodologies. The project advisory group is comprised of Indigenous and non-Indigenous national and state representatives from Australian government and non-government agencies/associations. The members have broad based experience in Indigenous health policy/health policy, the commissioning/procurement/contracting of Indigenous program evaluations and Aboriginal Community Controlled Health Services. The Indigenous-led research team is comprised of Indigenous and non-Indigenous experts in health promotion/population health, education, health program planning and evaluation, Indigenous health policy and Aboriginal community-controlled health services. Together, the project advisory group and research team have extensive experience in the commissioning of Indigenous program evaluations by government and non-government agencies. The commissioning practices will be coded using the best practice principles into draft models. The models, as they are developed, will be regularly presented to both groups to check whether any models are missing, whether dimensions from models are absent and to check whether the models are consistent with members’ experiences with the commissioning of Indigenous health program evaluations.
Patients and Public Involvement
Patients and the public were not involved in the development of this scoping review protocol.
Discussion
Implications
The findings of this scoping review will be used to strengthen the commissioning practices of Indigenous health and wellbeing programs by government and non-government agencies in Australia and may also have broader applicability to other countries with Indigenous populations The researchers believe that the identification of the scope and nature of evaluation commissioning models and the ways they are understood to operate in practice will aid in the further development of commissioning Indigenous health and wellbeing evaluations.
The scoping review will also contribute to stage two of an Australian-based NHMRC project, where they will be used as a coding framework to further consider the ways in which the commissioning of Indigenous health and wellbeing program evaluations occurs in practice in Australia. More specifically, the commissioning models identified from this scoping review will be elaborated on through interviews with both commissioners of evaluation, evaluators and Indigenous health program providers in Australia, and in-depth case studies of completed commissioned evaluations of Indigenous health and wellbeing programs.
Ethics and Dissemination
Since this scoping review will only review publicly available materials, ethics approval from a Human Research Ethics Committee (HREC) is not required. The scoping review will however adhere to the National Health and Medical Research Council National Statement (National Health & Medical Research Council, 2007 (Updated 2018)) and the Ethical conduct in research with Aboriginal and Torres Strait Islander peoples and communities: Guidelines for researchers and stakeholders 2018 (National Health and Medical Research Council, 2018). A policy brief will be disseminated to project stakeholders, government and non-government commissioning agencies (e.g. the National Indigenous Agency of Australia) and relevant professional associations (e.g. the Australian Evaluation Society Cultural and Diversity Committee). The research team will work closely with project advisory group members to find optimal media to translate the review findings to influence and alter commissioning practices for the benefit of Indigenous communities. This effort may include face-to-face or online workshops with commissioners and evaluators. Scoping review results additionally will be disseminated through a peer reviewed publication and conferences/seminars.
Strengths and Limitations
A major strength of this scoping review is (and will continue to be) that from its induction Aboriginal researchers (and members of the project advisory group) have led and contribute(d) to its design and production. Resultingly this scoping review will reflect a broad range of Indigenous and non-Indigenous perspectives and evaluation and commissioning experience. The latter aside, importantly this research uses ‘evaluation principles derived from [a variety] Indigenous contexts’ (Maddox et al., 2021, p. 345).
Another strength will be its selection of databases. Given the risk associated with methodologies that limit themselves to academic literature and thereby potentially exclude literature regarding evaluation commissioning that may not have been published due to publication barriers (McGrail et al., 2006), this scoping review will include a web-based search as one method of identifying grey literature. Nonetheless, in limiting our research to include evaluations within the health and wellbeing context, we risk missing relevant literature as there may also be examples of good evaluation commissioning practice outside this field. A further limitation will be that only publicly available documents are identified. There may be government or non-government reports that include commissioning practices which are not accessible to the research team.
Conclusion
In conclusion, following calls from Indigenous leaders and academics for more recognition in the direction and processes of evaluations from their inauguration, this scoping review will inform evaluation stakeholders and policy makers in two ways. First, to characterise the scope and nature of commissioning models of evaluation commissioning that are applied in practice, and second, determine how these align with Indigenous best practice principles. This will be done from an Indigenous standpoint, allowing for the inclusion and direction of other ways of knowing and being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Health and Medical Research Council under grant GNT1165913.