
Abstract
This article describes the background behind the development of a novel evaluation approach of an Aotearoa New Zealand rural health service using an equity-focused, strengths-based approach to complement the traditional audit process. This approach avoids a deficit-based, gap-analysis of service shortcomings in favour of a strengths-based model through which services can draw on identified assets in planning future service initiatives. The approach discussed aims to identify and mobilise assets and strengths of people and services that promote quality outcomes, with a particular focus on those that address the deeply embedded health inequities for Māori (the indigenous people of Aotearoa). The asset model will be used to evaluate a rural service that is uniquely co-located with other health-related hospital services. This article aims to provide a commentary on the benefits of an asset-based approach to rural general practice evaluation.
What we already know:
• Asset-based approaches to health have been shown to improve equity and facilitate individuals and community to have agency over their own health.
The original contribution the article makes to theory and/or practice:
• This article describes the background behind a novel approach for evaluating a rural primary care health service that focuses on assets and strengths as a complement to the traditional audit evaluative approach. • This asset-based approach is a novel approach to health service evaluation that promotes the use of identified strengths within individuals, whānau (family), the service and the community to enhance outcomes for Māori and others.
Introduction
Health inequities within Aotearoa New Zealand primary healthcare are well documented, particularly in rural settings (Adcock et al., 2019; Beazley, 2019; Chepulis et al., 2020; Dalbeth et al., 2018; Gifford et al., 2021; McMenamin, 2021). In recent years, it has been identified that these healthcare inequalities are maintained by deficit-based approaches to health (Glasgow Centre for Population Health, 2014). In contrast, approaches focused on assets or strengths and co-production have been increasingly employed in the health sector, with great success. These approaches require collaboration between health services, the community and tāngata whaiora (individuals seeking wellness).
It is important to recognise that people have both assets, expertise and personal resources that can contribute to positive health outcomes (Glasgow Centre for Population Health, 2014). Including service users, and working alongside, them empowers those using services to become increasingly resilient, while contributing to sustainable, holistic service development (de Schweinitz et al., 2017; Glasgow Centre for Population Health, 2014). Identification of how service delivery may be changed to meet the needs of patients and their whānau (family), in turn, contributes to more equitable outcomes. Asset-based approaches rely, however, on existing within a larger multi-faceted, intergenerational, communal approach if they are to bring about equitable outcomes (Glasgow Centre for Population Health, 2014; Van Bortel et al., 2019). This means that they must be ‘complementary to existing good public service provision, social support and protection, and established interventions to improve health and wellbeing’ (Glasgow Centre for Population Health, 2014, p. 14). The contribution of asset-based approaches lies in the identification of the health-enhancing strengths and assets provided by individuals, service providers, and the surrounding community, allowing for mobilisation of these resources.
Health-related research begins from one of two standpoints: (a) what are the factors making us ill? or (b) what are things that are keeping us healthy? (Migeot et al., 2022). The type of health strategies employed depend on the standpoint taken. When research is taken from the perspective of what makes us unwell (i.e. a deficit-based model), risk-based strategies are employed. Risk-based strategies aim to minimise risks associated with developing a specific disease or illness and promote costly, welfare-based approaches to health (Glasgow Centre for Population Health, 2014; Van Bortel et al., 2019). When viewed from the perspective of what keeps us healthy, however, strategies are focused on promoting and strengthening the protective factors that maintain and contribute to positive health and wellbeing; referred to as asset-based strategies (Glasgow Centre for Population Health, 2014). A 2022 rapid literature review identified that only 10.5% of human health-related research currently adopt an asset-based approach (Migeot et al., 2022).
Delivery and evaluation of health services is traditionally based on a deficit model, identifying health in terms of what the community lacks or the ‘problems’ they need resourcing to ‘fix’ (Morgan & Ziglio, 2010). This is particularly true of rural health services (health services centred outside metropolitan areas) (Kenny et al., 2013), where efforts are often seen as an attempt to reduce extant health inequalities between rural and urban populations (Bourke et al., 2010). Unfortunately, this deficit perspective may inadvertently contribute to health-related inequities (Glasgow Centre for Population Health, 2014; Morgan & Ziglio, 2007; Van Bortel et al., 2019), particularly the stigmatisation of ‘high need’ communities (Shepherd, 2012).
The purpose of evaluating a health service is to provide information on the best course of future direction (Ovretveit, 2004). Health services serve a heterogenous population of patients, with some presenting with complex needs (Eiriz & Figueiredo, 2005). Thus, when evaluating the effectiveness of health services for particular groups of patients, it is recommended that information be gathered from multiple sources. This includes those who attend the clinic (e.g. the patients and their whānau) and those who provide the care (e.g. clinicians, managers, receptionists, etc.). Importantly, it has been suggested that it is necessary to evaluate the relationship between the patients and the providers within the evaluation (Eiriz & Figueiredo, 2005). Typically, standard health service evaluations are typically done via audit, based on clinical measures and scales (i.e. the Servqual Scale) (Ovretveit, 2004; Pekkaya et al., 2019). The problem with this approach is that findings are usually interpreted through a deficit model lens (Ahmed et al., 2018; Greenwood & Zhan, 2019).
The shift away from the deficit perspective, toward asset-based approaches to health care, attempts to redress potential equity issues by identifying population and community strengths that may enhance health outcomes (Rippon & South, 2017). In contrast to a traditional deficit approach, asset-based health approaches focus on the potential and strength within a community as a foundation for enhancing health and the things that are working well within that population (Graham et al., 2021; Hopkins & Rippon, 2015; Van Bortel et al., 2019). In this respect, an asset-based approach may help resource-poor rural health services identify existing community and health service strengths that could be further drawn on for the enhancement of current service provision.
New Zealand rural context
The Urban/Rural Profile classification, developed by Statistics New Zealand, uses seven categories to describe rural and urban New Zealand (National Health Committee, 2010). Within these, four are considered to encompass the concept of rural. These include highly rural/remote area, rural area with low urban influence, independent urban area, and rural area with moderate urban influence. There are unique challenges associated with providing health care to those living in rural areas of Aotearoa, which includes the fact that the population is both diverse and spread across large areas. This makes access to emergency and secondary care services difficult, with many having to travel long distances to access care.
In addition, there are recognised inequities between Māori and non-Māori living in rural areas versus urban areas (National Health Committee, 2010). Non-Māori living in rural areas have a similar life expectancy to those of non-Māori living in urban areas. For Māori, however, there is a discrepancy for those living in rural areas, with rural Māori men and women living1.5 years and 1.2 years, respectively, less than urban Māori men and women. In addition, there are socioeconomic differences between rural and urban Māori; for example, rural Māori are more likely to be from highly deprived backgrounds (quintile 5) than urban Māori. This is important, given that socioeconomic status is linked to health outcomes.
Asset-based approach
An asset-based approach – which is derived from the Asset Model – draws on three components; salutogenesis, asset mapping and asset indicators (durable assets that provide a proxy for income) (McKenzie, 2005; Morgan & Ziglio, 2007; Rippon & South, 2017; Van Bortel et al., 2019). Combining the Greek words for health (salus) and origin (genesis) (Hopkins & Rippon, 2015), salutogenesis theory was developed as a move away from a pathogenic focus on health deficits, and toward understanding the factors maintaining health (Antonovsky, 1987). It has been described as ‘a health disease continuum between dis-ease and ease’ (Bonmati-Tomas et al., 2019, p. 2). According to Hopkins and Rippon (2015) exploration of salutogenesis ‘refers to the study of the origins and causes of wellbeing, including the mental, social, and other resources that people draw on and that influence their wellbeing’ (p. 3). In this manner there are a number of vital questions at the core of a salutogenic, or strength-based approach: What are the key factors that generate health? Who are the individuals or groups who stay well? Which health resources are contributing to their experiences and positive outcomes? (Rippon & South, 2017). The two key components of salutogenesis are generalised resistance resources (GRRs) and sense of coherence (SOC) (Bonmati-Tomas et al., 2019). ‘GRRs are defined as ‘a property of a person, a collective or a situation which, as evidence or logic has indicated, facilitates successful coping with the inherent stressors of human existence’. SOC is defined as ‘the ability to understand the overall situation and the capacity to use available resources’ (Bonmati-Tomas et al., 2019, p. 2). One current model for reducing health inequity, which uses the concept of strengthening people’s existing GRRs, are health promotion programs (HPPs). These programs focus on improving social determinants of health (e.g. improving access to food or housing); however, they cannot reduce inequity alone.
Internationally, strengths-based HPPs have been successfully used for indigenous communities in rural areas. For example, a recent strengths-based study focussing on Aboriginal and Torres Strait Islanders in Australia highlighted the desire for self-determination by indigenous communities, with a focus on indigenous knowledge systems (Dudgeon et al., 2020). In addition, an Alaskan study implemented an HPP in an attempt to reduce the large number of suicides among Alaska Native (AN), by promoting holistic wellness (de Schweinitz et al., 2017). Participants expressed a preference for increased access to health care systems The HPP approach was viewed as a positive step toward the development of community hope.
Asset-based approaches currently used in healthcare
Two recent reviews of the literature have identified asset-based approaches as an important complement to traditional models, which could be used to guide health-related interventions (Migeot et al., 2022; Van Bortel et al., 2019). In their systematic review of the literature, Van Bortel et al. (2019) noted that, to date, the majority of asset-based research has been carried out in Western countries, particularly the USA, the UK, Norway and Spain. Moreover, research has tended to focus on the general population or higher-income groups, as opposed to low-income, vulnerable populations. Van Bortel and colleagues argued that this was problematic, given the potential for asset-based models to reduce health inequities, particularly given that ‘health assets’ were mostly commonly described using Morgan and Ziglio’s (2007) definition, which states that ‘a health asset can be defined as any factor (or resource) which enhances the ability of individuals, groups, communities, populations, social systems and/or institutions to maintain health and well-being and to help reduce health inequalitites’ (p. 18).
Van Bortel et al. (2019) also noted that many of the studies incorporated the concept of asset mapping; however, the majority of these studies focused on the procedural factors behind asset mapping, as opposed to their application within the research.
In their rapid review of asset-based strategies in health, Migeot et al. (2022) highlighted the need for increased promotion of asset-based approaches, stating the potential for reducing health inequity. They reported that ‘it appears possible to identify health assets from among the health determinants corresponding to the personal, social, economic and environmental factors influencing the health status of person and populations alike’ (p. 2).
The benefits of asset-based for services and communities
While traditional deficit-models help identify factors underpinning poor health outcomes, an asset-based approach founded on salutogenesis offers two important benefits for health services and communities. Firstly, it can identify strengths within an individual, community or service prior to any form of intervention (Morgan & Ziglio, 2010). Asset models are relational and uncover interconnections between groups of people, highlighting the ways through which these assets may be accessed (McLean, 2022; Morgan & Ziglio, 2010). An asset-based approach also provides a positive way of engaging, involving and empowering people both in the services and in the wider community (Morgan & Ziglio, 2010). In this manner, asset-based approaches also allow services to establish a set of salutogenic ‘indicators’ which can be assessed and monitored to understand the contexts within which they are most effective (Morgan & Ziglio, 2007). The second benefit is that it facilitates an equity-focus in health systems evaluation. The Asset Model evolved out of the recognition that many marginalised communities (i.e. those from high deprivation areas) are viewed from a deficit, needs-based model (McKnight & Kretzmann, 1990). This results in the belief that their needs can only be met by organisations outside of the community, relegating them to ‘client’ status, whose wellbeing is reliant on ‘others’. Over time, this mindset leads to communities surrendering the notion of being responsible for their own wellbeing, in exchange for becoming a consumer of a service; thus, perpetuating inequity.
The decision to change the focus from a deficit-to an asset-based model requires a complete systems change (McLean, 2022; Rippon & South, 2017). It is not enough to promote an assets approach as an ‘add-on’ to the traditional sectorial response, as this has minimal influence or impact on delivery, which, in turn, leads to a ‘disconnect’ between the service and the community (Rippon & South, 2017). To aid navigation while transitioning between the two models, Rippon and South have developed a theory of change (ToC) model (Figure 1). The model identifies themes and phases required to reach the point of asset-based outcomes. The theory of change for asset-based approaches (taken from Hopkins & Rippon, 2015, p. 8).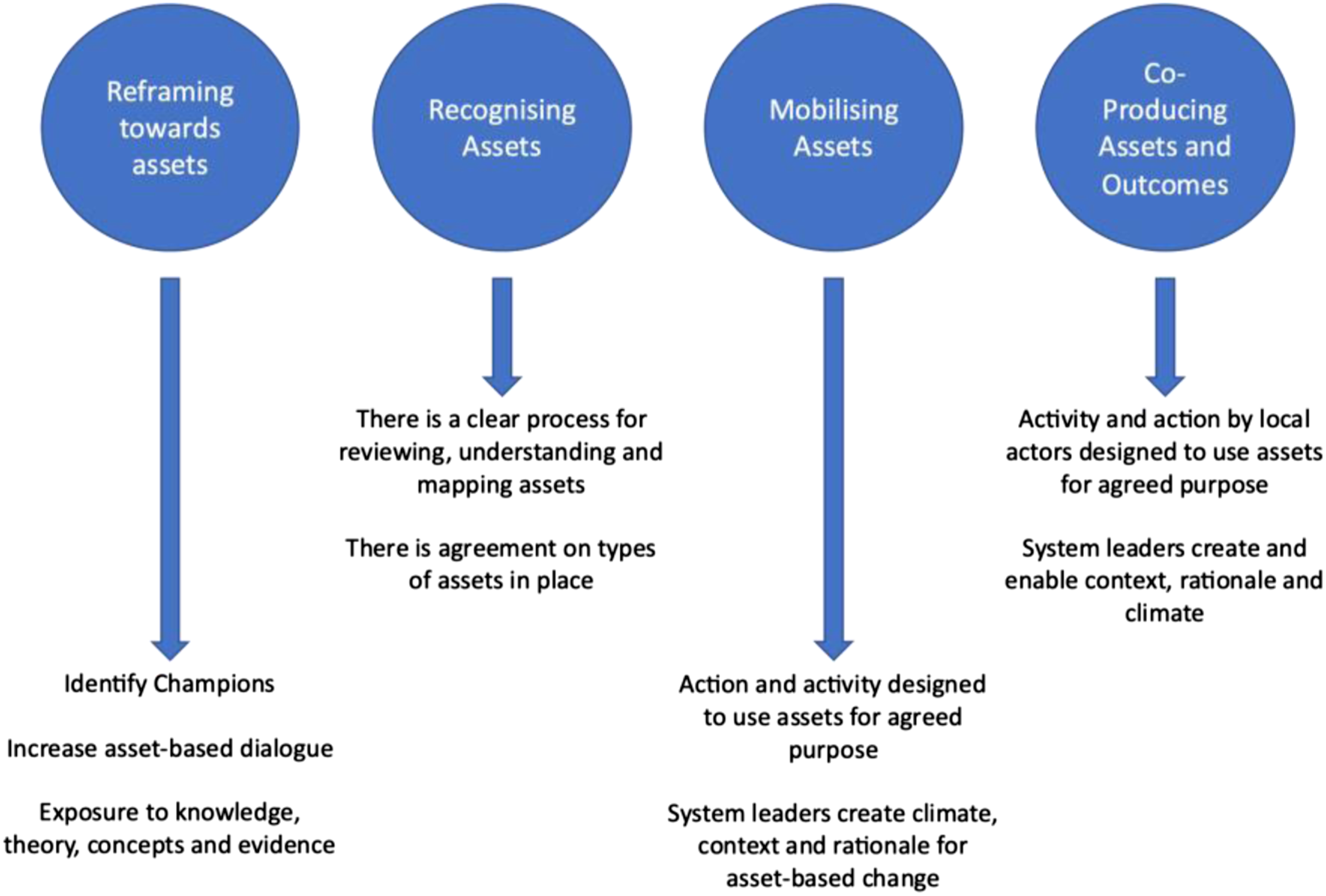
Applying an asset model approach to health services
Primary care is central to maintaining health and wellbeing within a community (van Weel & Kidd, 2018). It is acknowledged to be the point within the health system where universal coverage can be achieved. Given the important role of primary care within a community (Art et al., 2007), it is vital to ensure that practices are monitored to ensure high quality provision of service. It has been recognised that, in order to strengthen primary care, there is a need to shift the focus of delivery from one that is focused on disease-based treatment to one that addresses the health and wellbeing of individuals and the community (van Weel & Kidd, 2018). This presents a more strength-based approach.
Internationally, asset-based approaches have been successfully applied to national health care services, as a way to prevent problems, rather than reacting to them (Glasgow Centre for Population Health, 2014). For example, in Scotland, policy and legislation have been created to support the use of an asset-based healthcare system (McLean, 2022). An asset-based, co-production approach has been implemented by the Glasgow Centre for Population Health and has led to ‘a focus on co-creating appropriate community-led responses to addressing local priorities with local people’ (McLean, 2022).
Similar systems have also been implemented within Aotearoa New Zealand on a smaller scale. For example, while not specifically based on the asset model, the Kāpiti Youth Service (KYS) in Paraparaumu, developed their own strengths-based model to evaluate their service (Bailey et al., 2013). The purpose of the model was to ‘identify the changes experienced by young people and to identify the contribution KYS made to those changes’ (p. 2). Approaching the evaluation from a strengths-based lens led to information around where KYS was providing, and therefore could continue to provide, services effecting positive change for vulnerable youth.
Furthermore, an asset-based approach has successfully been used to develop an augmented Māori maternal care programme in a North Island, East Coast, rural region (Adcock et al., 2019; Lawton et al., 2021). Adcock and colleagues report that the asset model approach ‘aligns with Kaupapa Māori Research and “Whānau Ora” (Māori family wellness) – an approach that places whānau [family], hapū [subtribe], Iwi [tribe] in the centre of decision-making and promotes self-determination’ (p. 510). This sits with other strengths-based research that has been carried out in Aotearoa New Zealand (e.g. appreciative inquiry), which have been demonstrated to align with Te Ao Māori (the Māori world view) (Cram, 2010).
A benefit of using a strengths-based approach to health-related evaluation is the wider encompassing of indigenous values (Thurber et al., 2020). Rather than focussing specifically on the bio-medical factors, which have been noted to devalue indigenous culture, there is room to incorporate a holistic approach, which includes the cultural, emotional and social wellbeing of everybody within the community (Durie, 2004; Thurber et al., 2020). This has been demonstrated in work by Williams and colleagues (Williams, 2018), who developed the Ngaa-bi-nya evaluation framework to ensure contextual and cultural components of the Wiradjuri peoples from central New South Wales, Australia, were ‘consciously collected, analysed, and reported’ (p. 8). This evaluation framework is based on relationships and highlights the importance of avoiding the use of ‘success’ or ‘failure’ as concepts of evaluation, instead focussing on how to learn from opportunities for improvement in different areas of the service or programme.
Given the central role of primary care in community health and wellbeing (van Weel & Kidd, 2018), we believe that there is value in taking the larger Asset Model concept and applying it to the evaluation of a specific primary care organisation within a rural community, which has a high Māori population. In line with what is occurring in Scotland, this places the focus on a health organisation, encompassing the principals of person- and community-centred ownership of health, central to both the Asset Model and Māori world view (Adcock et al., 2019; Morgan & Ziglio, 2007). Firstly, it identifies the ‘primary building blocks’ (i.e. those located within the service) (McKnight & Kretzmann, 1990). As highlighted by McKnight and Kretzmann, people are the ultimate assets. Thus, this approach allows for the identification of strengths possessed by practitioners, patients and whānau in promoting positive health and wellbeing. In addition, it identifies financial, cultural, relational and business-related assets within the service. Secondly, it identifies the ‘secondary building blocks’ (i.e. those located within the area, but external to the service). These resources may include local hospitals, marae, iwi, non-profit organisations, and other health or social service agencies). Finally, it is possible to identify resources that are external to the service and community, but which contribute to the health and wellbeing of the population; for example, larger urban hospitals or services to which patients may be referred. The end result is a map that identifies the assets, as opposed to the deficits, of the rural health service and associated community.
Conceptualisation of an assets-based evaluation approach
We suggest that the use of an assets-based evaluation approach will be an effective and positive way to evaluate rural health services. To test this, we intend to clinically evaluate a recently established rural primary care service in Aotearoa New Zealand. This service is unique in that it is co-located with Emergency Department services, in-patient clinical services and residential care services. The clinic owners wish to understand the value and opportunities inherent in this novel co-location model.
We propose an evaluation of this novel rural health service using a mixed-methods approach. This includes both a standard clinical audit, using existing outcomes measures, including integrated and incentive performance, health targets, systems levels measures and health system indicators, in addition to an Asset Model approach. The purpose of adding the Asset Model framework is to identify factors contributing to positive health and wellbeing in Māori that may not be detected by a traditional service audit. This complementary approach will demonstrate (a) the assets the health service currently utilise that promote positive health outcomes; and (b) areas where there may have been asset-based gaps in service delivery and outcomes. This, in turn, will be used to identify potential assets that could be incorporated into future practice. The objective of an asset-based focus is to allow for further development of processes that may facilitate equity within the service and region.
Prioritising Māori voice
Like many other indigenous peoples around the world, Māori experience inequity in health outcomes (Adcock et al., 2019; Beazley, 2019; McMenamin, 2021; Willing et al., 2020). In Aotearoa New Zealand, Māori voice and world view have not been part of the historic design of New Zealand health systems. This has resulted in these communities having higher levels of unmet need, exclusion from services, and health inequity. Instead, health has tended to be approached from a Western world view, rather than a Māori world view; thus, standard approaches to health may not fit with Māori understanding of illness or health (Willing et al., 2020). Understanding patient experience is known to lead to better outcomes for patients (Jones et al., 2020). It is important, therefore, to understand the experience of indigenous patients, in order to reduce health-related inequities (Jones et al., 2020). For this reason, the current research intends to prioritise Māori voice in order to understand what is currently working well for Māori and areas were known assets of the evaluated service might benefit this group. The intent of this asset-based approach is to privilege Māori voice because designing services for Māori unmet need reflects designing services for those in Aotearoa New Zealand with the most need. In this regard, designing for Māori is designing for all. By privileging Māori voice, we are ensuring that Māori ideas, concepts and world view lead the review of services and ideas for future growth. This will be achieved by identifying the assets and strengths of patients, whānau, clinicians, the clinic and surrounding services that led to quality outcomes for Māori patients.
Research impact
Clinical evaluation of health services is usually approached from a traditional deficit-based clinical audit. This article provides an opportunity for commentary on an asset-based approach to rural general practice evaluation, which aims to supplement the traditional approach with a strengths-based perspective. It is proposed that using an asset-based approach to service evaluation will enhance equity for Māori who use the service and impact future patient care and service provision by the target rural health service. Identified assets will be incorporated more widely into every day service provision, as a way of ensuring all patients have access to resources that promote positive health outcomes. This approach, and the findings related to the clinic, will be presented to the Australasian rural health community, with the developed model being made available for use by other practices.