
Abstract
This study compares the healthcare management systems for cholera epidemics in Italy before and after the Crispi-Pagliani Health Reform of 1888. Specifically, we compare the monitoring, accounting, and reporting systems of deaths and infections during the 1884 and 1893 epidemics. Based on an econometric analysis of data from the Italian National Statistical Institute, we demonstrate that the post-reform system was more effective in reducing deaths by optimising medical personnel allocation in areas with higher epidemic intensity. From a Foucauldian perspective, we provide insights into the role of accounting in supporting noso-politics, bio-politics, and bio-power. Further, this study advances our understanding of reporting systems and the dynamics that governments trigger as part of strategies for preventing or containing contagion during epidemics. Finally, this study supports the use of econometrics in accounting history.
Introduction
The COVID-19 pandemic prompted governments to make rapid decisions regarding policy interventions to contain the contagion and its consequences. These interventions were based on weighing the effects of the pandemic and related health measures. Social distancing rules, lockdowns, and curfews may save lives during a health emergency. However, an appropriate reporting system for infections and deaths is equally crucial in managing health emergencies. Crucially, it allows governments to adopt the most forward-looking choices to manage the pernicious effects of a disease.
Our understanding of the role of accounting in a health emergency is still limited, despite the contemporary literature on the impact of the COVID-19 pandemic on accounting, accountability, and management practices (Leoni et al., 2021a). Such practices have helped in managing the pandemic; however, they have been misused in some cases or have generated negative social outcomes (Leoni et al., 2021b). Accounting and accountability play a role in exceptional decision-making in various organisations, including businesses, not-for-profit organisations, and charities (Carungu et al., 2021; Delfino and van der Kolk, 2021; Huber et al., 2021; Kober and Thamber, 2021; Passetti et al., 2021; Sargiacomo, Corazza et al., 2021; Velayutham et al., 2021). Some scholars focus on accounting's role in exceptional decision-making at the government and country levels, exploring the ways in which governments use it while managing the pandemic (Ahmad et al., 2021; Ahn and Wickramasinghe, 2021; Ahrens and Ferry, 2021; Mitchell et al., 2021). Concerning historical investigations, Manetti et al. (2017) portray how the government used the accounting systems of a charity organisation as a control mechanism for the plague during the Renaissance in Florence. Among studies on the long-term effects on governments, scholars have focused on budgetary responses (Grossi et al., 2020) or the need to reconsider calculative practices to support budgeting (Anessi-Pessina et al., 2020). Sargiacomo, Servalli et al. (2021) have recently highlighted that the literature on natural disasters, including health emergencies, remains underdeveloped.
This study adopts a Foucauldian perspective to explore how accounting related to health emergencies supports noso-politics, bio-politics, and bio-power, and examines which aspects make one reporting system more effective than another in saving lives during an epidemic. Specifically, we compare the monitoring, accounting, and reporting systems (MARS) of deaths and infections used during the two cholera epidemics that affected Italy in 1884 and 1893. These two epidemics occurred immediately before and soon after the Crispi-Pagliani Reform of 1888, which is the most important health reform in Italian history that modified the reporting system for epidemic emergencies. Relying on secondary and primary sources kept at the State Archive of Naples, we applied econometric analysis to historical data collected from the Annals of Statistics published in the Italian National Statistical Institute's (ISTAT) Digital Library. Running a quantitative analysis allows us to explore how innovations in the new reporting and accounting system helped reduce deaths from cholera. The resulting insights can highlight the qualities that a reporting and accounting system for an epidemic emergency must possess to reduce the epidemic's impacts.
This study contributes to the accounting (history) literature in three ways. First, this work enhances our understanding of how accounting supports noso-political and bio-political strategies for exercising biopower. Second, we contribute to the knowledge of the reporting systems and dynamics used by governments as part of the strategies for preventing or containing contagion during health emergencies. Third, our work supports the use of econometrics, which is rare in accounting history (McDonald, 2006; Richardson, 2006; Walker, 2008). Accounting history studies, which are predominantly qualitative, typically identify death as a transactional phenomenon used in calculative practices, or a consequence of organisational or institutional activity that gives rise to demands for accountability (Fleishman et al., 2004; Sargiacomo et al., 2012). Here, we apply econometrics to the data on deaths and infections to assess the effectiveness of a reporting system.
The remainder of this article is organised as follows. First, we present the theoretical framework of the study, and Foucauldian notions of noso-politics, bio-politics and bio-power. We then describe the Italian public health scenario until its reform and reconstruct the reporting systems used for epidemic emergencies before and after the 1888 Reform. Subsequently, we apply the difference-in-differences (DID) method and present the results. The final section presents the conclusions of this study.
Noso-politics, bio-politics and bio-power
We consider the problematisation of the health of a population within the context of an epidemic. ‘Problematisation is the central philosophical device in Michel Foucault's work’ (Koopman, 2011: 537). According to Foucault (2019a: 118), the point of problematisation is ‘this development of a given into a question, this transformation of a group of obstacles and difficulties into problems to which the diverse solutions will attempt to produce a response’. Foucault (1984: 274) explicitly deals with the problematisation of the health of a population in political terms: ‘Health and sickness, as characteristics of a group, a population, are problematised in the eighteenth century through the initiatives of multiple social instances, to which the state itself plays various different roles’.
Specifically, around the eighteenth century, pastoral power started to take a new form: ‘It was no longer a question of leading people to their salvation in the next world but rather ensuring it in this world. And in this context, the word “salvation” takes on different meanings: health, well-being (i.e., sufficient wealth, the standard of living), security, [and] protection against accidents’ (Foucault, 1982: 784). In his comparative discussions of three episodes of illness (leprosy in the Middle Ages, plague at the end of the Middle Ages, and smallpox in the context of eighteenth-century practices of inoculation), Foucault (2007: 10) identifies an evolution of the ways of problematising: ‘In short, it will no longer be the problem of exclusion, as with leprosy, or of quarantine, as with the plague, but of epidemics and the medical campaigns that try to halt epidemic or endemic phenomena’. The new form of problematisation entails a ‘shift from the narrow context of charitable aid to the more general form of medical police, imposing its constraints and dispensing its services’ (Foucault, 2019b: 95).
This marks the emergence of noso-politics, where ‘the problem of the health of all is a priority for all and the state of health of a population is a general objective of policy’ (Foucault, 2019b: 92). Noso-politics also includes the ‘set of systems and processes for the administering and administration of medicine: data collection, statistics gathering and comparison, in a word the “scientification” and “mathematisation” qua “statistification” of knowledge about both health and disease’ (Foucault, 1994: 50–51, cited in Mendieta, 2014).
Noso-politics is only a component of the bio-politics of the population regulating the biological processes of ‘propagation, births, mortality, the level of health, life expectancy and longevity’ (Foucault, 1990: 139). Bio-politics generates bio-power through its dispositifs: sexuality, race, productivity, health, mortality, fertility, and so on. The concept of bio-power also includes ‘strategies for intervention upon collective existence in the name of life and health’ (Rabinow and Rose, 2006: 197). Essentially, bio-politics is the modality of producing, circulating, and enacting bio-power that subjects and governs individuals through a set of disciplines that normalise bodies. It produces political effects through new forms of power knowledge and corresponding dispositifs (apparatuses) (Mendieta, 2014).
In the ‘area of bio-power’ (Foucault, 1990: 140), ‘life and its mechanisms’, including death, have been brought into the ‘realm of explicit calculation and made knowledge-power an agent of transformation of human life’ (1990: 143). Now, ‘processes of birth rates, mortality rate, longevity’, for example, are measured in ‘statistical terms’ (Foucault, 2003: 243). These calculations concerning life, disease, and death are considered forms of accounting, or ‘documents of any kind which typically use text and numbers in structured or unstructured ways to provide records of commitments and transactions between named and unnamed parties’ (Sargiacomo et al., 2012: 396). In particular, the latest accounting history literature (Moerman and van der Laan, 2022) identifies opportunities to investigate the intersection between accounting and death by understanding how it has been conceptualised and mobilised in the past.
The problematisation of the health of the Italian population and the Crispi-Pagliani Reform
The epidemic waves of cholera in nineteenth-century Italy
In the nineteenth century, Italy was severely affected by cholera. The first wave occurred in 1835–1837, followed by 1854–1855. The next epidemic in 1865–1867 was especially vicious, with a devastating toll of over 160,000 deaths (Sabbatani and Piro, 1998). The means to combat cholera were limited, given that the country was predominantly agricultural and economically strained (Snowden, 1995). A long debate concerning cholera began in pre-unification Italy (before 1861) involving men of science, politicians, and intellectuals, with significant confusion about the nature and modality of the contagion (Snowden, 1995).
This disease was not just a biological phenomenon, but also a social one (Evans, 1988; Rosenberg, 1966) because it highlighted the weaknesses of the health management systems and prevailing poverty. These factors made cities key locations for contagion and disorder (Snow, 1849). Indeed, the epidemic primarily affected the economically poorest regions in southern Italy, with Naples, the most populated city in the Kingdom of Italy, being the hardest hit (Snowden, 1995).
The 1884 epidemic was a major transformative event in Italian history with lasting consequences (Snowden, 1991). Its dramatic aftermath underscored the inadequacy of public hygiene defences and outdated methods of accounting for deaths that were scientifically unreliable. The preventive and therapeutic measures implemented by Italian medical and public health authorities proved to be unsuccessful (Tagarelli et al., 2000). Remarkably, data on the spread of cholera epidemics from 1884 to 1893 showed a decrease in the last waves (Table 1).
Cholera epidemics in Italy (1884–1894).
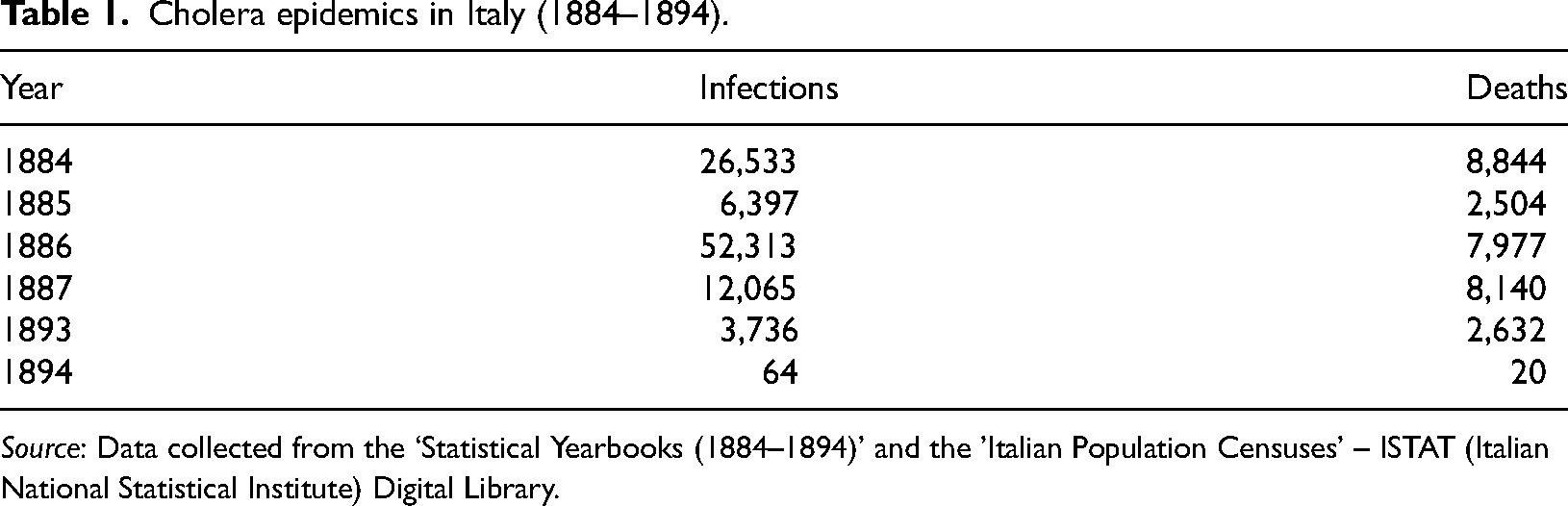
Source: Data collected from the ‘Statistical Yearbooks (1884–1894)' and the 'Italian Population Censuses’ – ISTAT (Italian National Statistical Institute) Digital Library.
The 1884 wave and regional discrepancies
In the last decades of the nineteenth century, the Kingdom of Italy's administration was divided into 16 compartimenti (territorial compartments) 1 and 69 provinces. This was a strongly hierarchical and centralist structure in which provinces were conceived as intermediate entities between the state and municipalities. Through the prefect located in each province as the local representative of the government, the central government could ensure that provincial and municipal politics adhered to that of the centre (ISTAT, Annals of Statistics, 2018; Pavone, 1964). The provinces were divided into distretti or circondari, governed by sub-prefects. The circondari were divided into mandamenti. The municipality, regardless of size, was the terminal link of central power. It was governed by the mayor, who was a ‘hybrid’ figure. The mayor, being both the ‘head of the municipal administration’ and ‘an officer of the government’, was the delegate of the central government (Pavone, 1964).
The cholera outbreak of 1884 caused approximately 780,361 deaths in Italy. For an estimated population of 29,010,652 as of 31 December 1883, this implies approximately 26.9 deaths per 1000 inhabitants (ISTAT, Annals of Statistics for Deaths, 1885, 1886). This wave also had significant regional discrepancies. First, it mainly hit Naples, Milan, and Rome, the most populated cities (see Table 2).
Population of the 10 largest Italian cities (excluding their provinces) in 1884.
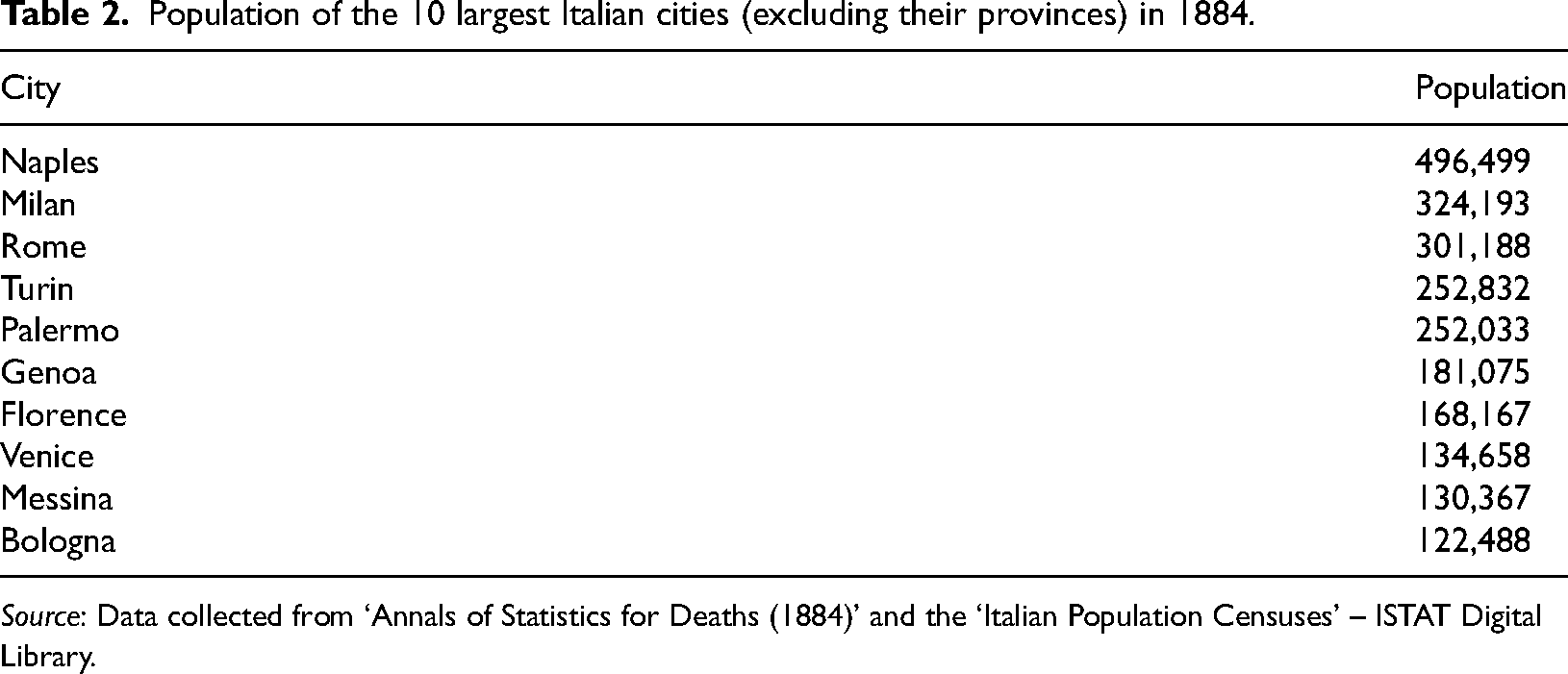
Source: Data collected from ‘Annals of Statistics for Deaths (1884)’ and the ‘Italian Population Censuses’ – ISTAT Digital Library.
Second, the northern regions with adequate hospital infrastructure experienced lower mortality rates than the southern regions (see Table 3).
Number of cholera deaths in Italian regions in 1884.
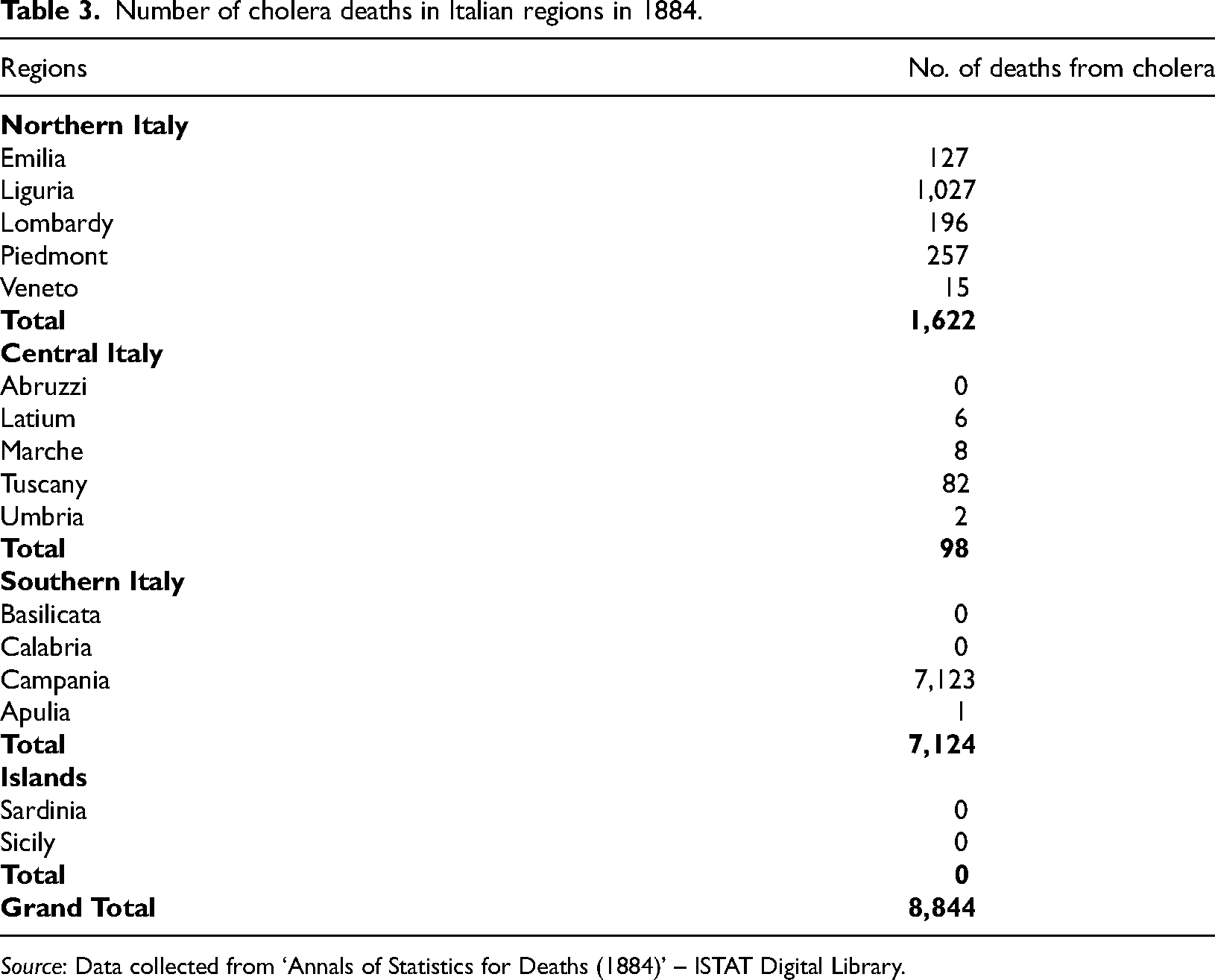
Source: Data collected from ‘Annals of Statistics for Deaths (1884)’ – ISTAT Digital Library.
Specifically, Campania in the south was the most devastated, with its death rates contrasting sharply with those of other Italian regions. This disparity largely stems from substandard sanitary conditions and an acute shortage of medical professionals, especially in Naples (Snowden, 1995). This situation served as an urgent call for the central government to enforce new preventive strategies to curb the number of deaths and infections, with an emphasis on aiding the most vulnerable regions (Taroni, 2021).
The Crispi-Pagliani Reform
In this situation, Italian Prime Minister Francesco Crispi realised the urgent need to overhaul the Italian health administration (Taroni, 2021). The literature back then noted that the sharp rise in cholera infections and deaths was largely attributed to inefficiencies within the health system and the misallocation of medical resources in underserved regions (Maino, 1999). In response, Crispi enacted the Kingdom of Italy's inaugural public health law, thereby creating the General Directorate for Public Health and augmenting the medical workforce to counteract the disease's spread (Snowden, 1995). The Parliament ratified the law in December 1888 (Law No. 5849 of 22 December) under the title, ‘On the protection of hygiene and public health’. It is historically recognised as the Crispi-Pagliani Reform, as it was ideated and co-authored by Prime Minister Crispi and Luigi Pagliani. The latter was Italy's first Professor of Hygiene, and founder of the Italian Society of Hygiene, Preventive Medicine, and Public Health in 1878. This reform is a cornerstone in the annals of Italian health institutions and its core tenets remained operational even until the late twentieth century.
The MARS for epidemics before and after the Crispi-Pagliani Reform (1888)
The Crispi-Pagliani Reform significantly highlighted the role of medical doctors in Italy, drawing politicians’ attention to public healthcare. It sought to foster better communication and cooperation in coordinating efforts to combat epidemics and infectious diseases. Its influence was particularly evident in the reporting systems for epidemics and corresponding accounting methods used to record infections or deaths in Italy during the late nineteenth century (Figure 1).
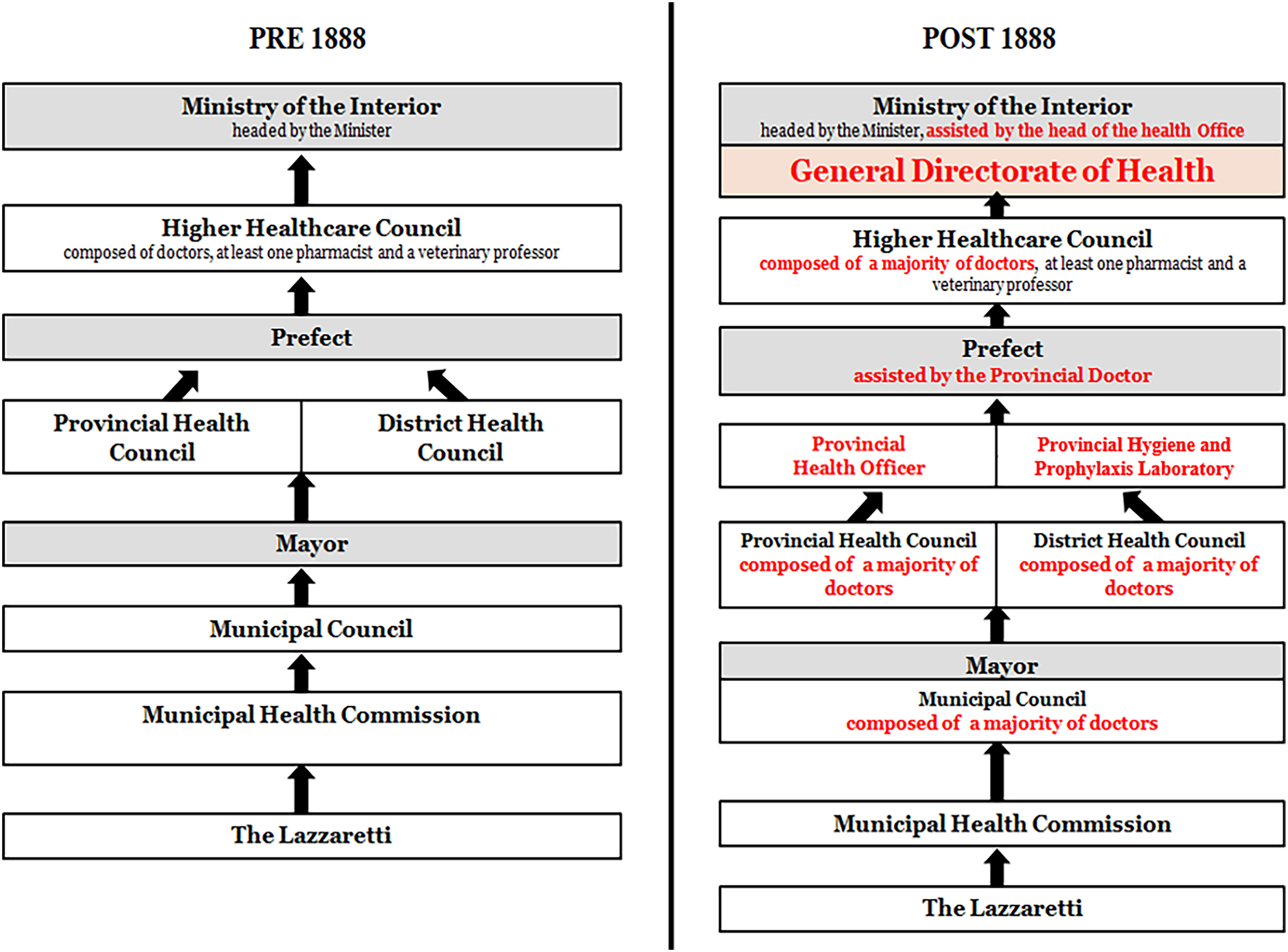
Comparison of the Italian management and reporting system for epidemics before and after the Crispi-Pagliani Reform (1888).
The MARS for epidemics in Italy before 1888
Before the reform, Italy's health system was decentralised and centred on local authorities and sanitary police. Health reporting bodies were almost entirely comprised of administrative staff without medical expertise.
At the local level, the main actor was the ‘medico condotto’, a medical officer who provided health and care services in the city or district community, and whose remuneration largely depended on the local economic resources. During the first epidemic waves of the nineteenth century (before 1888), these medical officers primarily operated in local hospitals and ‘lazzaretti’, which were specialised hospitals designed for isolating incurable patients or those with contagious diseases (Caddeo, 2020). At the government's request, these officers became primary data sources on infections/deaths, as they were uniquely positioned to diagnose the disease and assess its impact (Bassetti et al., 2011).
After the reform, the new regulations put the primary responsibility for tracking epidemics on mayors and Municipal Councils, aided by the Municipal Health Commission. This involved collating data from the lazzaretti, the starting point of the reporting system. Here, medical officers worked alongside friars and nurses, keeping records of patient admissions and discharges to track the epidemic's progress in the city, and detailing patient outcomes (e.g., whether they recovered or succumbed to the disease) (Figure 2).
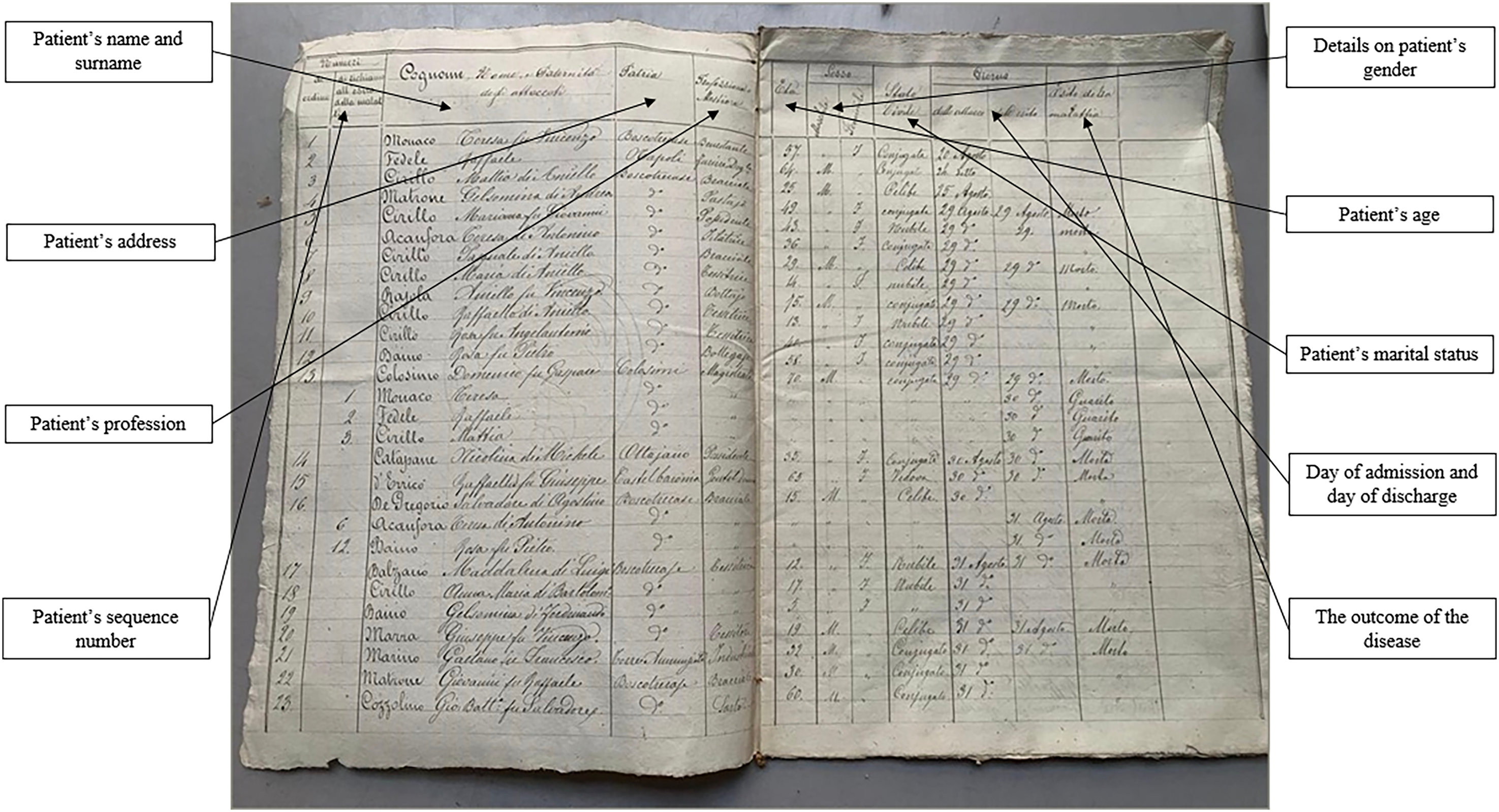
Daily register of infected and recovered patients in the lazzaretti.
These data were summarised using data collected from home-to-home visits, which were almost entirely entrusted to the sanitary police. However, in many cases, these collected data were not validated by doctors who could recognise the symptoms and disease characteristics of the patients (Forti Messina, 1976). The combined figures from the lazzaretti and home-to-home visits were relayed to the Municipal Health Commission and subsequently to the Municipal Council. The council then prepared a health bulletin detailing infections and deaths to monitor the epidemic trend (Figure 3).
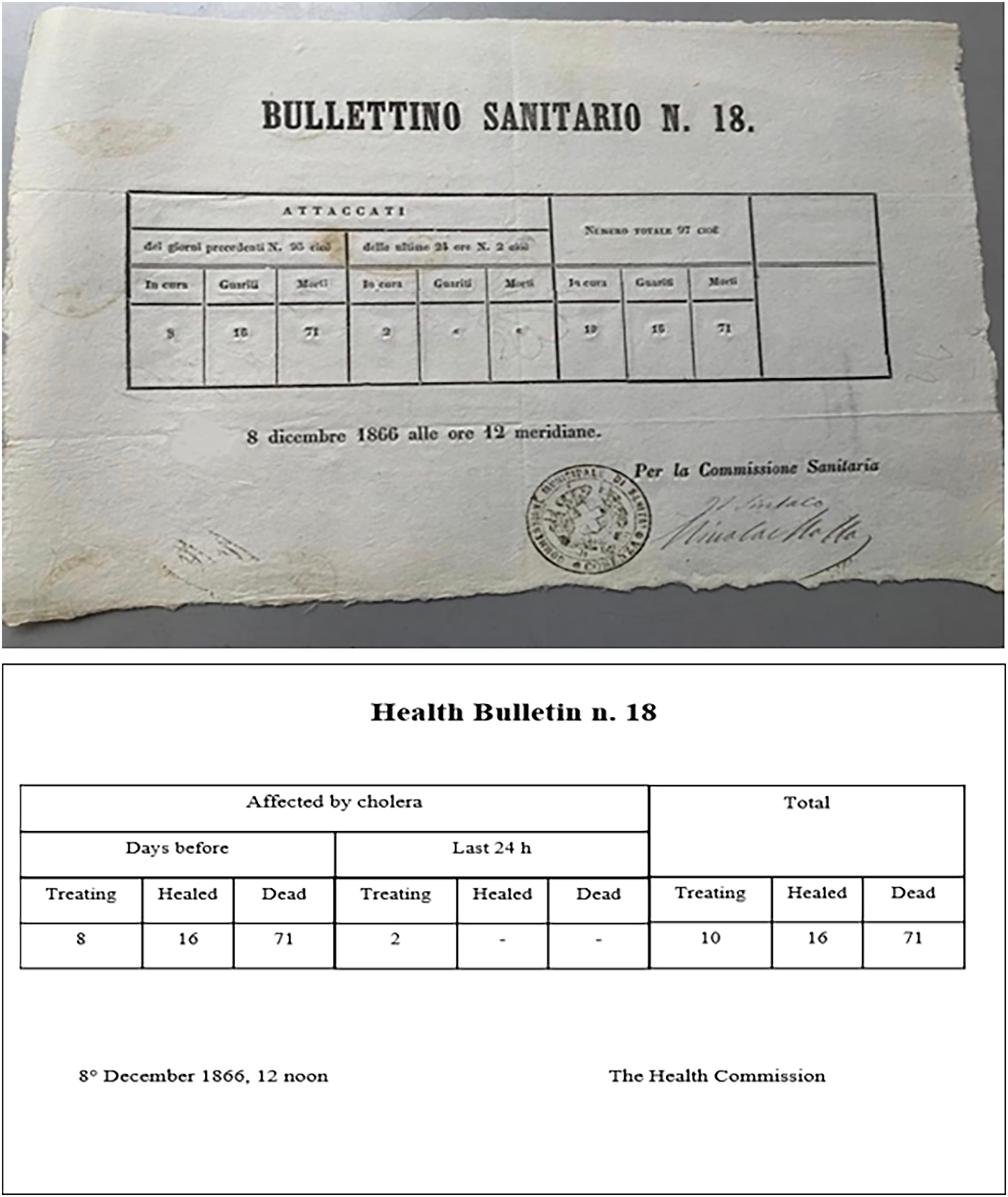
Bulletin of the Municipal Health Commission on cholera cases in Naples.
The mayor then reported all gathered cholera cases to the Provincial Health Council. Next, the prefect sent the verified final results to the Higher Healthcare Council, which comprised medical professionals. This council provided the Ministry of the Interior with a comprehensive report on epidemics across all Italian regions (articles 17–20 of regulation of 8 June 1865, no. 2322). The Ministry compiled these data into a detailed national overview segmented by region and city (Figure 4).
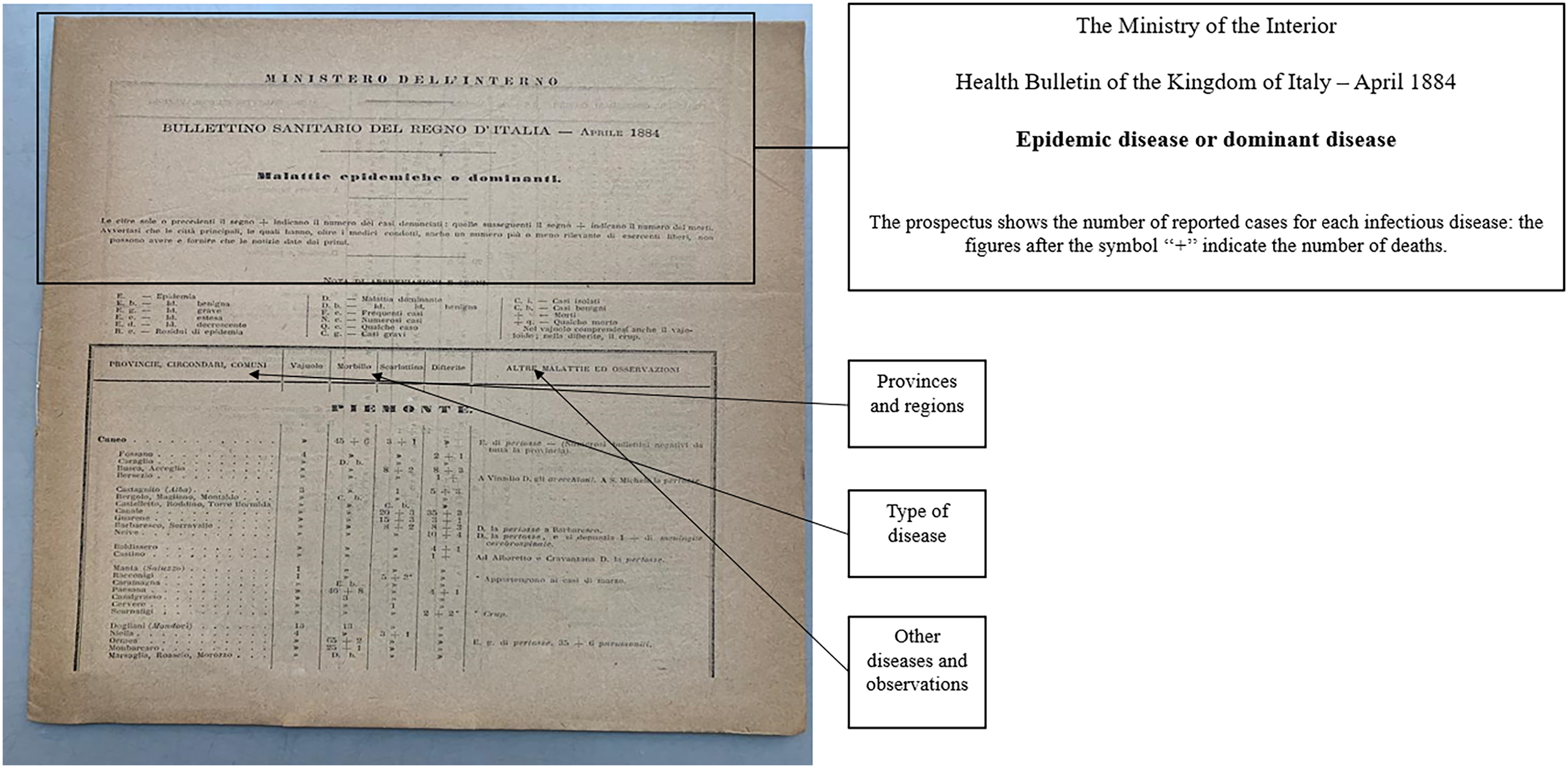
National summary prospectus provided by the Ministry of the Interior.
In this reporting system, the Higher Health Council was the sole body composed entirely of medical professionals (doctors, at least one pharmacist, and a veterinary professor). In contrast, most members of Provincial and Municipal Health Councils were part of the administrative apparatus, with medical professionals (doctors and veterinarians) constituting only one-fifth of members in Provincial Councils and three-sevenths in Municipal Councils (Bassetti et al., 2011). This was the primary limitation of the pre-1888 epidemic reporting system because it adversely affected the accurate accounting of cholera infections and deaths, especially in remote areas (Forti Messina, 1976). Moreover, the majority of administrative staff tasked with managing epidemics lacked the medical expertise required to validate infection and death data at the peripheral level. Most cholera reports did not include essential ‘medical observations’ vital for determining patients’ conditions and whether they had the disease. In particular, data from home-to-home visits, which were primarily handled by the sanitary police, lacked comprehensive verification by medical personnel. Hence, members of the medical community believed that the official death count did not genuinely represent the severity of the situation (De Renzi, 1854). Similarly, mainstream historians argue that data from major Italian cities and towns suffered from reporting inconsistencies (Imperato et al., 2015). Furthermore, information on cholera cases before the Crispi-Pagliani Reform was markedly imperfect, leading to significant underreporting (Forti Messina, 1976).
The MARS for epidemics in Italy after 1888
Errors in estimating deaths and infections prevented the government from appropriately allocating medical resources and promptly addressing the epidemics (Forti Messina, 1976; Imperato et al., 2015). Hence, in 1888, Crispi and Pagliani increased the number of medical professionals and enhanced their roles in epidemic-related administrative tasks.
The reform introduced a pyramidal organisational structure that centralised the health system (see Figure 1). At the apex of the administrative health system, the General Directorate of Health combined institutional authority with scientific expertise. It was responsible for regulating both Italian administrative and sanitation needs and supervising the revamped health-administrative framework. At the provincial level, the provincial health officer, and the Provincial Hygiene and Prophylaxis Laboratory assisted the prefect in scientifically vetting medical reports. The reform abolished the sanitary police, decreeing that qualified medical professionals should conduct health inspections and home-to-home visits.
The reform introduced municipal doctors who reported directly to the mayors and oversaw medical officers. They functioned as state officials operating across the nation and aided administrative authorities in tracking and monitoring epidemic trends. The reform mandated their participation in the Municipal Council, which had a majority of its members from the medical profession after 1888. Their role was to oversee the initial epidemic data gathered from home-to-home visits and lazzaretti by medical officers (medici condotti) (AP, Letter n. 258; AP, Reunion of 1890). Every municipality was obliged to compile case statistics (Figure 5) using a designated form. This form, validated by the municipal doctor's signature, was designed to swiftly identify disease outbreaks and was accompanied by a document format used prior to the reform. The government cannot be content with fragmented and incomplete information; it is bound to scrutinise facts comprehensively. Mere anecdotes, incidents, and exceptions are insufficient - robust statistics are imperative. These statistics must precisely delineate phenomena, quantifying both the applied methods and their outcomes (Reale Società Italiana d’Igiene, 1891).
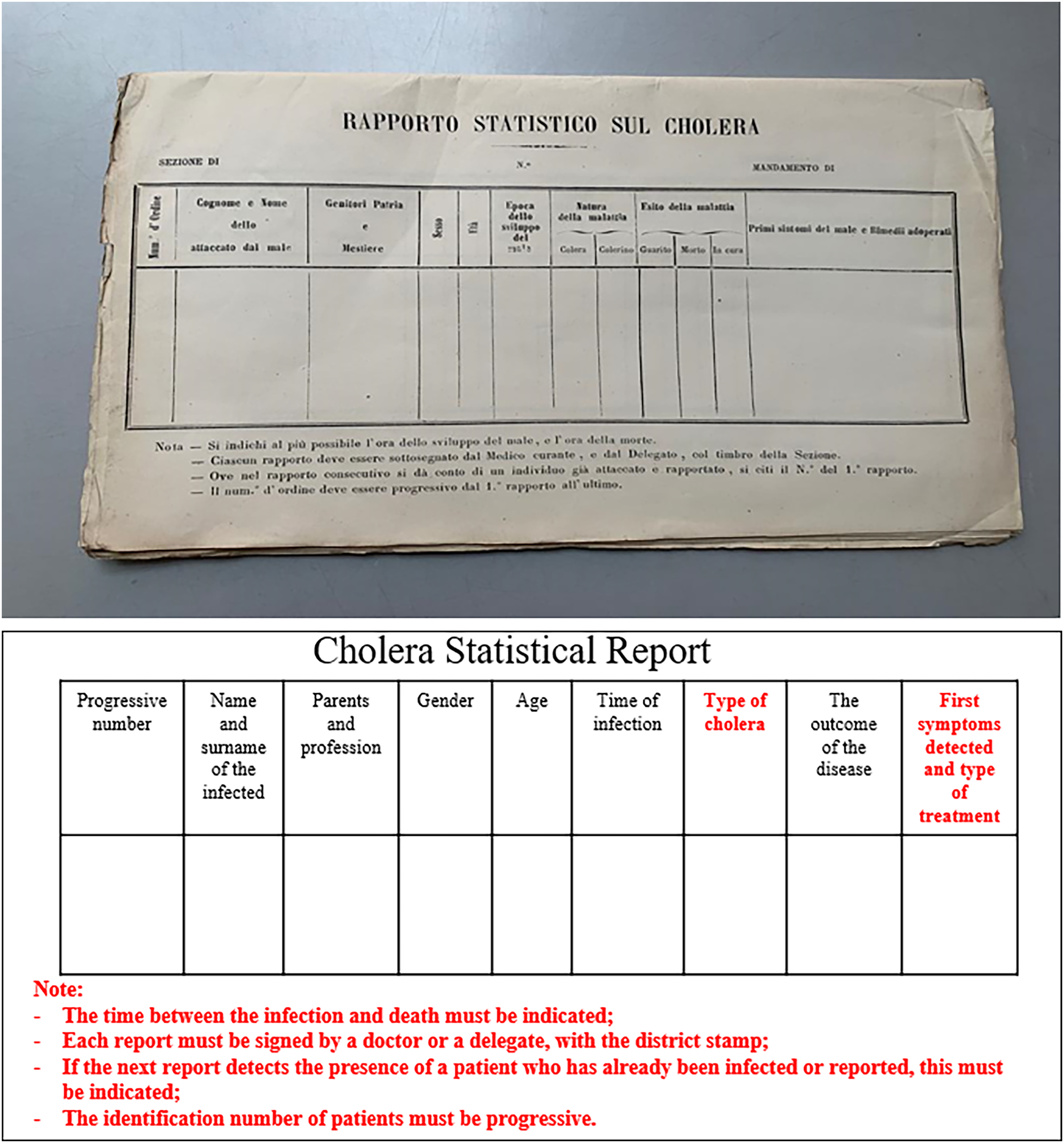
Example of a cholera statistical report produced by Italian municipalities post-1888 Reform.
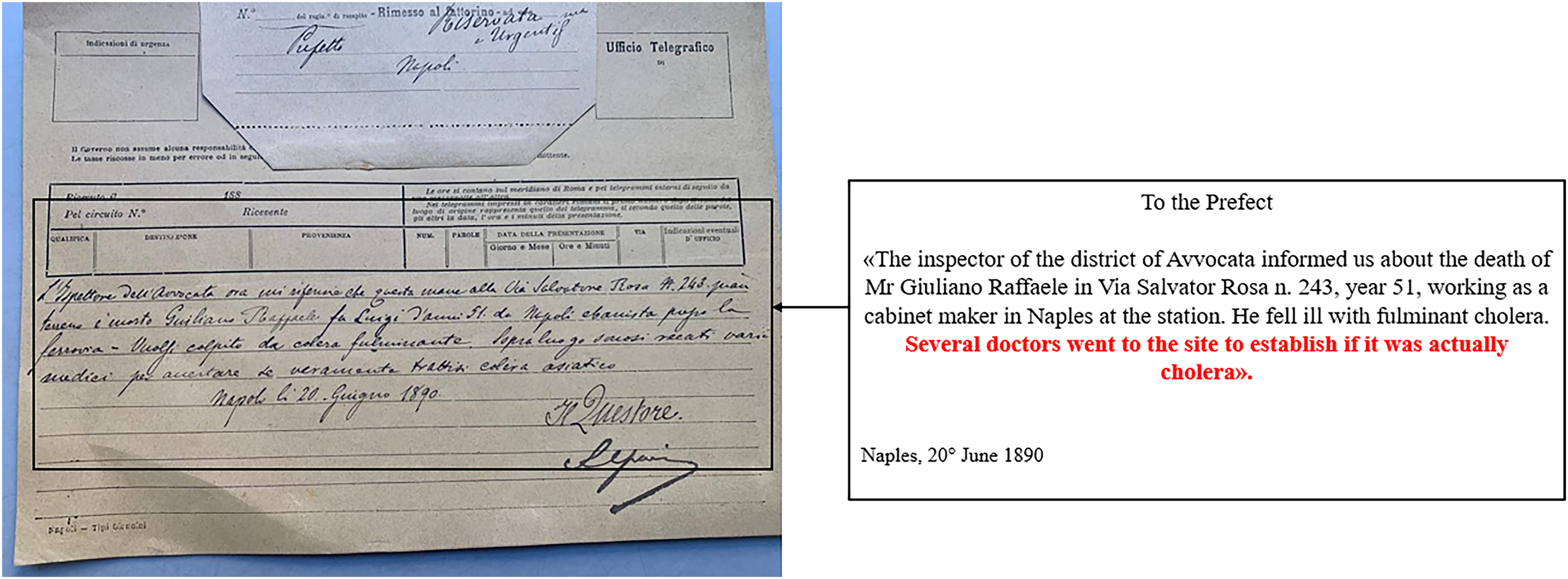
Under the guidance of municipal doctors, medical officers were now mandated to inform the mayor about the disease causing any deaths, supplementing their reports with their clinical and pathological observations. This procedural change also empowered medical professionals to verify the authenticity and accuracy of data regarding cholera deaths and infections from the local to centralised levels.
By scrutinising these reports and further assessing medical clinical notes from lazzaretti and home visits, the state could now gain a more in-depth and accurate understanding of the epidemic trends. The reform also specified that these supplementary medical reports must include (refer to Figure 5): initial symptoms and treatments administered, duration from infection to death, final doctor verification, and historical infection data of the patient. This helped in creating comprehensive and accurate records (AP, Letter n. 48548). Cholera-type identification, a pivotal advancement since nineteenth-century Europe, witnessed multiple cholera strains that required distinct treatments (Della Peruta, 1980; Snowden, 1995).
The replacement of administrative staff with medical professionals within the epidemic management apparatus, along with a subsequent increase in qualified medical personnel in hospitals and lazzaretti, enabled swift identification and reporting of cholera cases. Their expertise facilitated the precise differentiation of symptoms and timely identification of epidemic outbreaks (Della Peruta, 1980).
From 1889 onwards, data collection did not solely hinge on doctors but also on the synergy between health personnel and medical administrative machinery. At the provincial level, the reform introduced the role of provincial health officers. This officer, accountable to the prefects (affiliated with the Ministry of the Interior), provides the prefecture with executive and advisory services. The previous system allowed the Provincial Health Council to support the perfect in an advisory capacity. However, after the 1888 Reform, the provincial health officer was endowed with the autonomy and proficiency to tackle epidemics proactively. Despite limited archival data on the Provincial Health's activities, a vast amount of data relates to provincial health officers. This officer had the responsibility to stay abreast of cholera outbreaks across Italian provinces and provide consistent updates to the General Directorate of Health (Di Simone, 2002). The officers’ duties also encompassed on-ground inspections, enquiries, and validation of cholera-spread information, which was then conveyed to the General Directorate of Health and the Ministry of the Interior.
After 1888, both the Provincial and District Health Councils, which were pivotal links between central governance and the peripheries, were mandated to predominantly consist of medical experts. Their role was to scientifically ascertain the actual presence of epidemics, particularly in isolated or remote territories. The reform also provided the provincial health officer with supporting provincial hygiene and prophylaxis laboratories, which represented one of the most important scientific transformations of the new Italian health apparatus (AP, Letter n. 48548). This laboratory was the institutional body that scientifically validated data concerning deaths and infections from cholera. It strengthened the accounting system for epidemics, enabling the reporting of more accurate information to the prefect and then the central government to properly manage a health emergency (Figure 6). False alarms and incorrect data were supervised and reported by the laboratory (AP, Letter n. 48548).
Deaths from cholera were scientifically validated by the Laboratory of Hygiene and Prophylaxis, and reported to the General Directorate of Health post-1888 Reform.
It also coordinated information between the top and bottom of the administrative framework through continuous communication via telegrams with the Italian government. For each suspected or recognised infection or death in the peripheries (definitively proven by the laboratory), the government communicated with the prefects and then with the responsible mayor to plan the best strategy to contain the outbreak (Figure 7).
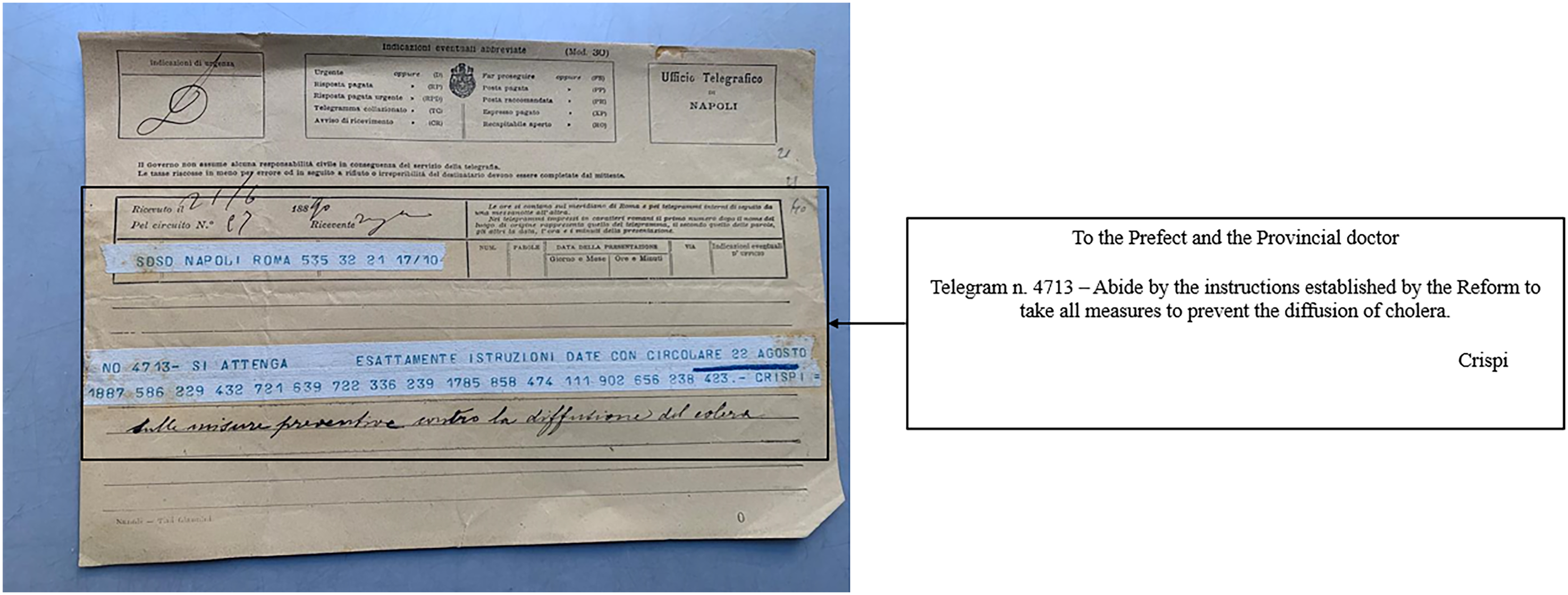
Sanitary directives from the General Directorate of Health for the affected provinces post-1888 Reform.
All doctors were required to follow the guidelines set by the 1888 Reform. The Higher Healthcare Council, which had a majority of doctors after 1888, gave final scientific approval to the information that came from the bottom of the administrative framework to assess the virulence of the disease in the country. At the top of the new health framework, the General Directorate of Health at the Ministry of the Interior was also dedicated to combining political power and technical-scientific knowledge.
The effectiveness of the reform: An econometric analysis
The Crispi-Pagliani Reform aimed to reduce the inefficiencies of the previous health system, which proved to be inefficient during the 1884 cholera wave, especially in the most populous cities (Della Peruta, 1980). Here, we aim to demonstrate that the reform allowed for better management of the 1893 cholera epidemic in Italy (with a reduction in mortality). Furthermore, we seek to ascertain how this reform had the most significant impacts on the areas hardest hit by the 1884 epidemic. Since the reform did not change the way the disease was treated, but rather how information about infections and deaths had to circulate through the state apparatus, the analysis allows us to assess the effectiveness of the new MARS compared to the previous one. We adopt an econometric methodology, the DID approach, to perform a multivariate analysis of the effect of the institutional shock (represented by the introduction of the Crispi-Pagliani Reform of 1888) on the allocation of health personnel and death from cholera in different regions.
Data
We utilised data from the ISTAT Statistical Yearbooks (1884 and 1893), detailing deaths and infections from cholera and other infectious diseases in Italy both before and after the 1888 Reform. We also collected data on the number of doctors deployed to address health emergencies and the total population of these provinces in the study years (ISTAT, Population Censuses). To provide an initial overall perspective, the descriptive statistics with provincial averages for each variable by region are reported in Table 4.
Descriptive statistics: Cholera outbreaks in Italy in 1884 and 1893, by region.
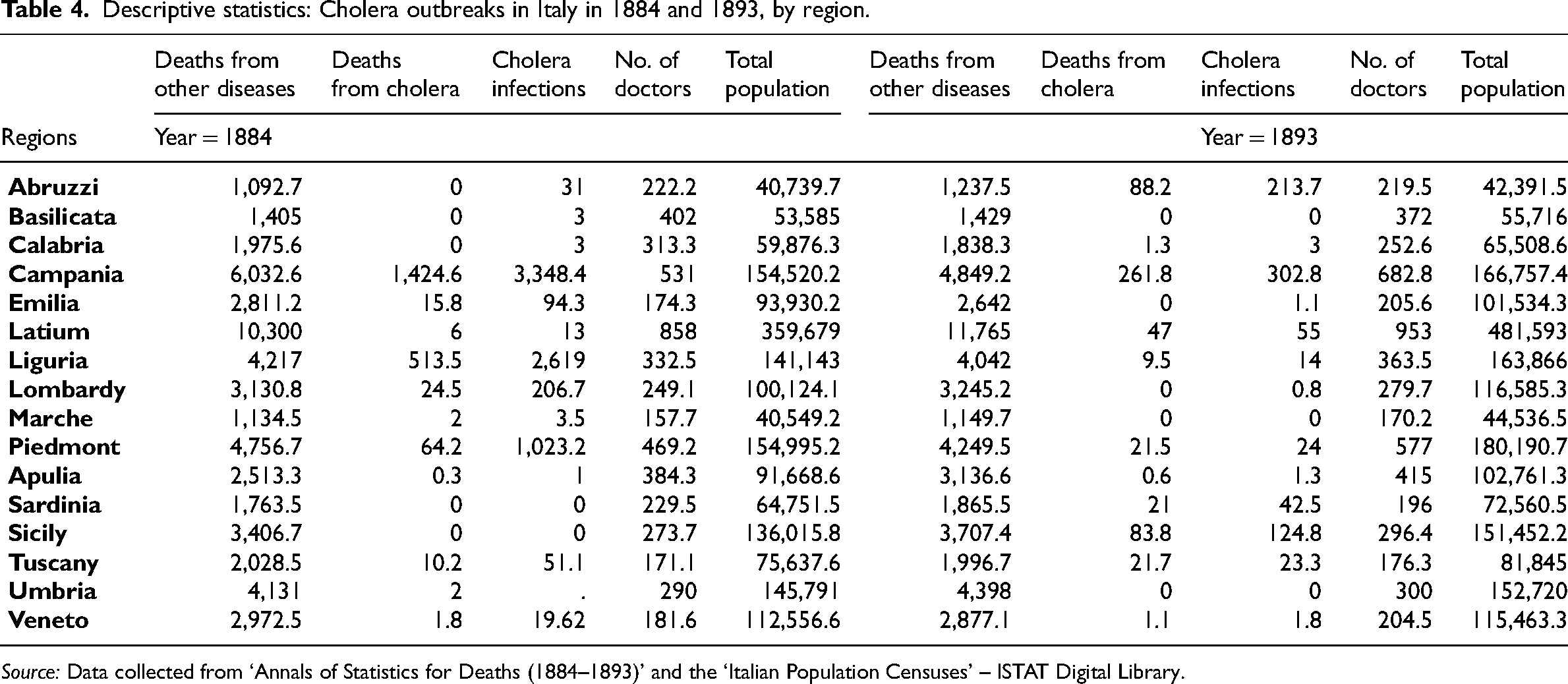
Source: Data collected from ‘Annals of Statistics for Deaths (1884–1893)’ and the ‘Italian Population Censuses’ – ISTAT Digital Library.
These descriptive statistics show a high degree of heterogeneity. In particular, the Italian regions with no recorded cholera cases in the 1884 wave (e.g., Abruzzi, Basilicata, Calabria, Sicily, and Sardinia) clearly show a reduction in the average number of doctors after 1888. Similarly, in Italian regions with more recorded cholera cases in 1884 (e.g., Campania, Emilia, and Liguria), the government allocated, on average, more doctors to these areas in 1893.
We test the effect of the Crispi-Pagliani Reform at the provincial level using a quasi-experimental analysis based on the DID technique, which is specifically used to control for external factors unrelated to the shock of interest (in our case, the introduction of the reform) (Angrist and Pischke, 2008).
Analysis
Our econometric analysis is carried out in two steps to test the following hypotheses. First, we aim to show how the new MARS, introduced by the reform to combat cholera health emergencies, guided the Italian central government's emergency responses in allocating medical personnel to territories where the epidemic was more acute. Specifically, we hypothesise: H1: Following the implementation of the Crispi-Pagliani Reform (1888), there is an increase in the number of doctors in the areas most affected by the 1884 cholera outbreak.
Second, we seek to quantify how these changes in doctor allocations directly affected the number of cholera victims. Specifically, we hypothesise: H2: There is a negative relationship between the increase in the number of doctors and a subsequent decrease in the number of cholera deaths.
However, we might observe an increase in cholera cases in areas with more doctors because of a more accurate reporting system. Furthermore, the increase in infections might lead to an increase in doctors in the most vulnerable areas. Because of these reasons, our estimates might be biased. Therefore, to address the causal impact of the Crispi-Pagliani Reform on cholera deaths, we exploit the local heterogeneity of cholera that occurred before the reform (in 1884) to measure its impact on the number of doctors allocated after 1888. Specifically, the reform increased the number of doctors, independent of the cholera outbreak, which did not occur between 1887 and 1892. Exploiting this, we conduct a quasi-experimental analysis using the DID technique, which allows us to control for possible sources of endogeneity by comparing the provinces most affected by cholera in the 1884 epidemic with those least affected in the same year. In this way, to assess the impact of the health policy on the distribution of doctors in Italian provinces most affected by cholera after the reform, we exclude potential confounding factors, such as ‘fixed differences between provinces’ and ‘intra-temporal differences due to historical events’, which could have affected one of the two years considered.
The ‘treated group’ consists of the Italian provinces that were more severely affected by cholera in 1884 (i.e., those with more than one infection per 1000 inhabitants), whereas the ‘control group’ includes the Italian provinces that were less affected by cholera in 1884 (i.e., those with one or fewer infections per 1000 inhabitants). We have structured the groups in this manner because our aim is to quantify the differential impact of the Crispi-Pagliani Reform between the areas more and less affected by the 1884 epidemic. Thus, although the Crispi-Pagliani Reform applied to all Italian regions, we intend to demonstrate that the magnitude of its impact in different regions was strongly influenced by the intensity with which the 1884 epidemic affected them.
We estimate the following DID specification to compare how medical doctors were allocated between these two groups of provinces:
Table 5 displays the results of our first regression, highlighting how the Crispi-Pagliani Reform differentially affected the distribution of doctors in provinces heavily affected by cholera.
Differential impact of the Crispi-Pagliani Reform on doctor allocation in Italian provinces (least affected and most affected by cholera).
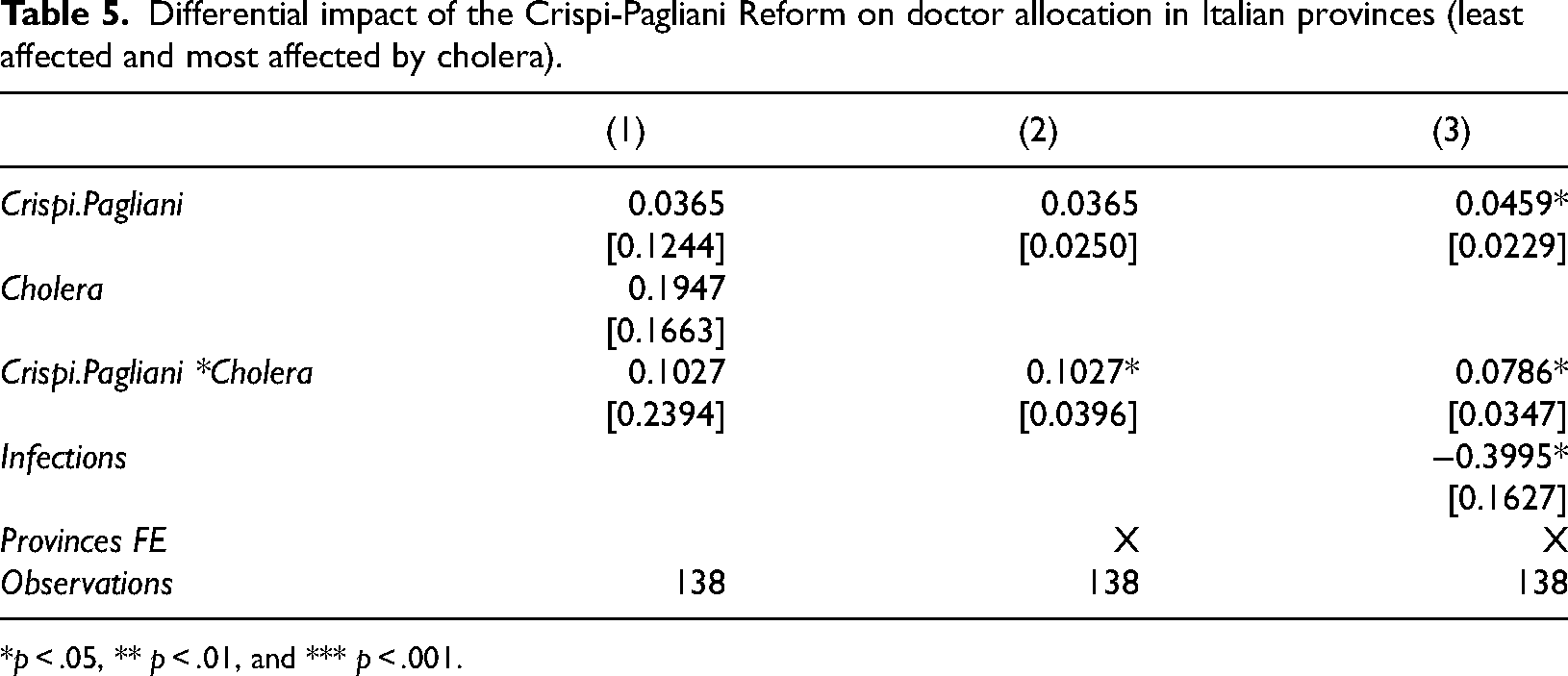
*p < .05, ** p < .01, and *** p < .001.
In columns (2) and (3), we have strengthened the validity of our estimates by including the ‘province fixed effect’ instead of the ‘
According to the DID specification in column (1), the difference in the allocation of doctors between the most cholera-affected and all other areas was not statistically significant. The statistical significance of our result is affected after dropping the ‘
Figure 8 graphically illustrates what is explicitly measured by the DID model. One of the fundamental assumptions of this model is parallel trends (Angrist and Pischke, 2008: 231), whose validity, unfortunately, cannot be verified with currently available statistical tools. 3
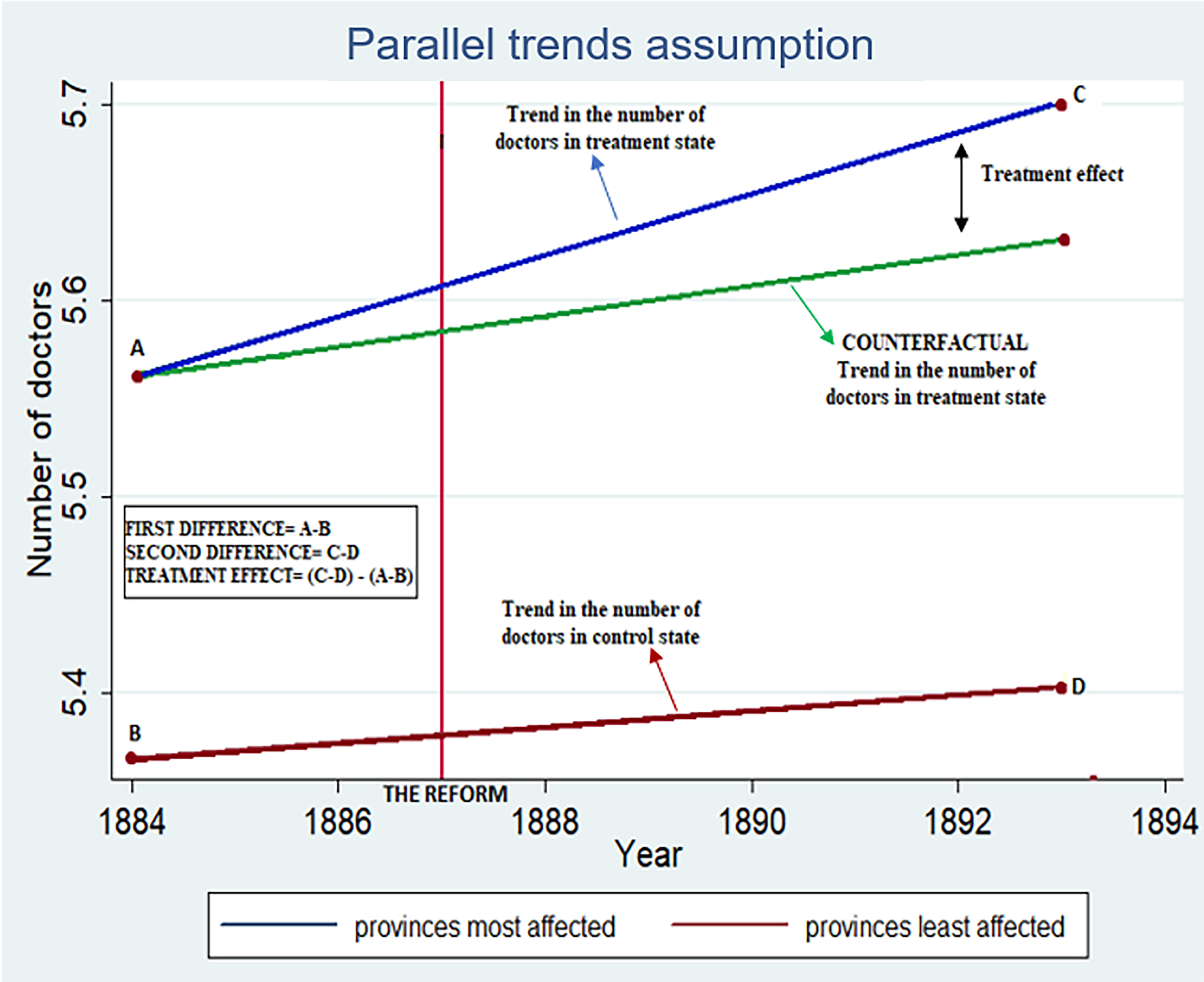
Parallel trends assumption in our DID model. DID: difference-in-differences.
In the second step of our econometric analysis, we aim to show that the increase in the number of doctors reduced the number of cholera deaths. As the number of cholera deaths could drive the allocation of medical staff in the provinces most affected by the disease, there may be a potential problem of reverse causality.
4
In addition, an increase in the number of doctors could improve the reporting of cholera cases, effectively increasing the number of reported cholera deaths without providing a clear indication of the effect. To address this causality issue, we use the variation in the number of doctors obtained in the previous step of the analysis, which is related to the change in doctors caused by the Crispi-Pagliani Reform in the provinces more affected by cholera. Specifically, we can assess the impact of the allocation of doctors by estimating the following instrumental variable regression model specification:
b: It is the estimated coefficient and represents the percentage change in cholera deaths per unit percentage change in doctor allocations.
The results of the second regression, summarised in Table 6, show the percentage impact (an increase of one percentage point in the number of doctors on cholera deaths). All columns presenting regression models include the ‘province fixed effect’; columns (2) and (3) also include the ‘
Impact of doctor allocation on the number of deaths due to cholera.
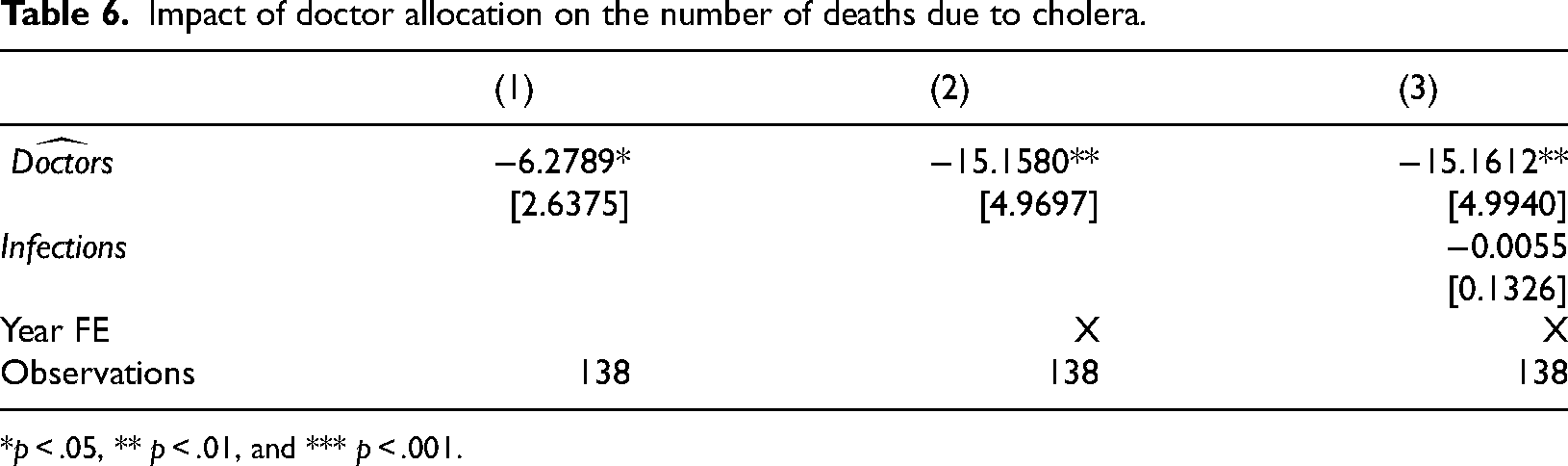
*p < .05, ** p < .01, and *** p < .001.
The coefficient in column (1) indicates a negative impact of −6.27 per cent for a one-percentage-point increase in the number of doctors. When we control for the differences between the two periods considered, the effect rises to −15.16 per cent and is statistically significant at the one per cent level. The result remains stable regardless of whether other types of infections are considered. This suggests that the increase in the number of doctors was effective in reducing cholera-related deaths.
Results
Two significant results emerge from our analysis. First, the allocation of medical personnel improved across the country following the Crispi-Pagliani Reform. In 1893, the number of medical staff increased in the areas most affected by cholera in 1884. Second, mortality decreased in these regions, which can be attributable to the increased number of medical professionals. The allocation of medical resources was guided by the new MARS: With Law No. 5849 of 22 December (On the protection of hygiene and public health), we have decided to increase the number of medical personnel employed to combat the disease. Please report to the General Directorate of Health the number of cholera victims in your territories and inform us if you need additional medical support! (AP, Il Nuovo Monitore degli Impiegati, 1890).
Second, the new MARS gave a central role to medical experts. Mainstream historians have highlighted that in 1893, the scientific and medical expertise of doctors, coordinated by the General Directorate of Health, represented the strength to combat epidemics (Della Peruta, 1980). Still, the role of the doctors was not confined to supporting the population but also consisted of replacing the administrative staff within the MARS. Their expertise allowed for clearer insights into epidemic trends. By validating the data, doctors ensured that the central government received reliable and accurate information. Consequently, epidemic hotspots in certain regions were identified effectively while sidestepping potential confusion with diseases exhibiting similar symptoms. Medical doctors also promoted a critical scientific rereading of clinical data collected during the 1884 wave by filtering out potential errors, underestimations, or overestimations, and providing a more accurate picture of the epidemic's progression (Della Peruta, 1980). By putting their expertise to the service of the ‘hierarchical observation’ of the subjects of bio-power (Foucault, 1995: 170), they supported the exercise of bio-power and allowed the central government to enact effective medical personnel allocation policies.
Conclusions
This study explored the effectiveness of Italy's Crispi-Pagliani Reform of 1888 in mitigating fatalities from the recurring cholera epidemic waves that affected the country in the nineteenth century. The reform introduced a new centralised surveillance apparatus for health emergencies staffed with specialised and qualified doctors. Further, it enhanced MARS to promptly inform authorities about the progression of the epidemic and enable the implementation of the most appropriate measures in the hardest-hit territories. We show that the innovations introduced in MARS allowed the government to allocate medical personnel more efficiently to areas experiencing more intense epidemic outbreaks. This optimisation significantly reduced epidemic-related mortality.
From the perspective of noso-politics, bio-politics, and bio-power, the reform shows how the health of the Italian population was problematised in terms of a new MARS, supported by the medical apparatus of knowledge. From the Foucauldian perspective, medicine is a bio-political strategy (Foucault, 2019b: 137). We demonstrate how accounting for the health, sickness, and death of the global mass representing the human species can make this strategy successful by informing noso-politics. Moerman and van der Laan (2021: 3) have argued that accounting related to death ‘serves multiple purposes including risk assessment, health policy formation and the allocation of healthcare resources’ and how ‘these calculative practices are mobilised as meaningful accounts involve human and non-human intermediaries’. In our case, we have both types of intermediaries. The reform acted as a non-human intermediary which helped MARS support the government's (bio-)power by reinforcing, controlling, monitoring, optimising, and organising the forces under it as ‘a power bent on generating forces, making them grow, and ordering them’ (Foucault, 1990: 136). Medical experts are human intermediaries used by political authorities to exercise bio-power, thanks to the role they can play within the (bio)power-knowledge nexus. Rose and Miller (1992) have raised the issue of experts’ role in the exercise of power. The authors highlight that experts are able to mediate between political objectives and the autonomous activities of actors thanks to the ‘constitutive role of expertise in problematising, inventing, and regulating particular domains of individual and collective behaviour’ (Miller and Rose, 1995: 592). In our case, medical experts were involved in two domains of knowledge: taking care of both the population and accounting information guiding the central government's bio-politics.
This study offers an overview of reporting systems for epidemics, which is scarcely explored in the accounting history literature (Manetti et al., 2017) providing insights into the dynamics between local and central governments (Gomes and Sargiacomo, 2013; Sargiacomo, Corazza et al., 2021).
Methodologically, this study adds to the recent literature which incorporates new econometric, cliometric, and statistical tools to evaluate accounting and reporting methodologies (Günther, 2017; MacDonald and Richardson, 2011; Masayoshi et al., 2021), and statistical information use in management accounting (Chandar and Miranti, 2009; Di Cimbrini, 2015; Talbot, 2010). Following Miller and Napier (1993), who advocate for contributions to the accounting history agenda by exploring alternative economic calculation methods beyond specific accounting processes, we adopt an econometric approach which Walker (2008: 311) notes is ‘unusual’ in the accounting history literature.
The study also contributes to the accounting literature in understanding how calculative practices help the governance of exceptional events and guide health emergency responses (Manetti et al., 2017; Sargiacomo, 2015; Shimizu and Fujimura, 2011). Two critical dimensions help increase MARS’ effectiveness: centralisation via a pyramidal structure and the involvement of medical expertise within the administrative machinery.
Finally, the benefit in 1893 due to the increased number of medical personnel in the territory underscores the necessity for national health systems to invest in community medicine. These are local medical services distinct from hospital-based care.
During the COVID-19 pandemic in Italy, the scarcity of community medicine frequently led hospitals to be quickly overwhelmed. We show that local medical services not only serve as immediate response units but also as guardians of the population's health because their medical-administrative knowledge ensures integration between primary healthcare and higher echelons of medical administration.
Footnotes
Acknowledgements
The authors gratefully acknowledge the anonymous reviewers for their insightful comments and suggestions, which have significantly strengthened the paper. The article is the result of a joint effort of the authors. The individual contributions are as follows: Tiziana Di Cimbrini wrote ‘Introduction’; ‘Noso-politics, bio-politics and bio-power’; and ‘Conclusions’; Alessio Maria Musella wrote ‘The problematisation of the health of the Italian population and the Crispi-Pagliani Reform’; ‘The MARS for epidemics before and after the Crispi-Pagliani Reform (1888)’. Concerning the ‘The effectiveness of the reform: an econometric analysis’ section, Alessio Maria Musella wrote the introductory part, ‘Data’ and ‘Results’ subsections; Giovanni Fosco wrote ‘Data’ and ‘Analysis’ subsections.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.