
Abstract
Difficulty getting to sleep is a frequent problem in society with a range of consequences for both physical and mental health. Listening to music before sleep has been shown to provide the potential to help improve sleep quality. However, the familiarity of the music and the presence of lyrics have the potential to alter the effectiveness of pre-sleep music, but remain largely unexplored to date. 169 participants were randomly assigned to one of four conditions: familiar music with lyrics, familiar music without lyrics, unfamiliar music with lyrics, and unfamiliar music without lyrics. In each condition participants were required to listen to this music for seven consecutive nights while they fell asleep. At the beginning and the end of the study, participants completed two self-report questionaries that measured their quality of sleep (PSQI) and insomnia (ISI). As expected, sleep quality and insomnia severity generally improved after 7 days of listening to music. Findings suggest that familiar music improved sleep quality (but not insomnia) more without lyrics, while unfamiliar music improves sleep quality more if lyrics are present. These findings contribute to an enhanced understanding of how to use music for aiding sleep in a more effective way.
Introduction
Sleep problems are a frequent and ever-increasing concern in modern society (Calem et al., 2012; Cappuccio et al., 2010), often resulting in poor sleep quality (Loewy, 2020). Healthy sleep in adults is characterised by a duration of 7 to 9 hours (Hirshkowitz et al., 2015), regularity and the absence of sleep disorders (N. F. Watson et al., 2015). It is estimated that 1 in 4 individuals from the Netherlands, the United States, and the United Kingdom get less sleep than their age specific recommendations (Kocevska et al., 2021). Listening to music has been shown to provide potential to improve sleep quality or reduce sleep onset latency (De Niet and collegeaus, 2009; Harmat et al., 2008; Ryu et al., 2012) and is low cost and low risk in comparison to some other treatments for insomnia. However, more research is needed about how music should be used, with factors such as the familiarity of music and the presence of lyrics potentially influencing the effectiveness of music played at bedtime, but so far not investigated in the literature. The exploration of these two factors, and how they might interact, is the purpose of the current study.
Increasing knowledge on treating poor sleep is important not only for people to feel less tired and more alert during the day, but also to improve physical and mental health outcomes for society in general. Short-term effects of poor sleep can include increased stress responsiveness, mood disorders, somatic pain (Luntamo et al., 2012), and cognitive and memory deficits. Long-term effects of poor sleep can include hypertension, increased risk of heart attacks (Meisinger et al., 2007), metabolic syndrome, and type 2 diabetes (Medic et al., 2017). Moreover, a bi-directional relationship between sleep disturbances and mental health conditions has been proposed (Freeman et al., 2020). For example, poor sleep is one of the main causes of depression (Meerlo et al., 2015) and depression also causes sleep disturbances (Goldberg, 2011).
Factors influencing sleep and treatment methods
A combination of factors influence sleep quality and can contribute to the potential development of insomnia. These factors exist within the environmental, behavioural, psychological, and physiological domains of a person and affect their sleep patterns (Troynikov et al., 2018). Of these, environmental and psychological factors in particular may benefit from music at bedtime.
The environment in which an individual sleeps, for example, the temperature of the room (Lan et al., 2014), how noisy (World Health Organization, 2009) or light it is (Cho et al., 2013), can lead to poor sleep quality and the development of sleep problems such as insomnia. Excessive light can be blocked out using eye masks (Babaii et al., 2015) and temperature can be adjusted by altering layers of clothing (Joshi et al., 2016). Noise levels ideally should not exceed 40 dBA in a bedroom (Caddick et al., 2018). If this is the case, environmental noise can be blocked out using earplugs (Le Guen et al., 2014). However, music is a viable alternative in this scenario and blocking external noise has been cited as one reason people listen to music at night (Trahan et al., 2018).
Psychological factors, such as worrying about not being able to sleep, can contribute to the development of insomnia and poor sleep quality (Talamini et al., 2013). This is further explained by a two-level metacognitive model, proposed to explain the development of insomnia (Ong et al., 2012), which suggests both primary (direct cognition) and secondary (physiological correlates of that cognition) arousal influence sleep quality. The psychological factors highlighted by the metacognitive model can be addressed and treated using mindfulness (Ong et al., 2012) and cognitive behavioural therapy for insomnia (CBT-I; Taylor & Pruiksma, 2014). Music can also be of benefit here, with people using music to help block out intrusive thoughts and to reduce their arousal (Trahan et al., 2018).
Sleep disturbances resulting from primary physiological sleep disorders are regularly treated with drugs such as benzodiazepines and Z-drugs. Benzodiazepines such as temazepam (Drummer, 2002) and nitrazepam (Donoghue & Lader, 2010), can be used to improve sleep quality (de Mendonça et al., 2023), as a short-term treatment (Lader, 2011). However, they produce several undesirable side effects such as impairing the formation and consolidation of new memories (Beracochea, 2006), an increased risk of cognitive decline in the elderly (Paterniti et al., 2002) and impaired motor function (Lader, 2014). Z-drugs, such as zopiclone and zolpidem are often prescribed as an alternative to benzodiazepines, as they are assumed to be safer (Siriwardena et al., 2010). However, Z-drugs can cause drowsiness, dizziness, and increase the risk of falls and therefore fractures in the elderly (Hoffmann, 2013). While Z-drugs may arguably carry less of a risk than benzodiazepines, they are not suitable for all populations or long-term use, making their application limited (Richardson et al., 2020).
Due to the side effects of the drugs outline above, psychological and behavioural treatments such as sleep hygiene and mindfulness, have recently become more popular as treatments for insomnia. Amongst these non-pharmaceutical options, cognitive behavioural therapy for insomnia (CBT-I) has been widely tested and applied and is now the first-line recommended treatment in many countries. These non-drug treatments have some benefits over drug treatments but are not without their own limitations. For example, while CBT-I is safer and with longer lasting benefits than drug treatments (M. D. Mitchell et al., 2012), it requires practitioners to have sufficient training (Halson, 2019), and has relatively low availability to date, limiting its application as a treatment. The same issue applies to mindfulness for insomnia, as mindfulness therapists are required to be specially trained (Shallcross et al., 2019), limiting its accessibility. Moreover, while sleep hygiene techniques have been found to be effective at reducing some sleep difficulties (Bogdanov et al., 2017), it is argued these techniques are vague (e.g. regular exercise is a suggestion but it is not stated what type of exercise and how long this should be done for) and with very limited overall effectiveness (Irish et al., 2015).
Music listening for improving sleep
The problems with drug treatments and the limitations of non-drug treatments for insomnia have given rise to alternative approaches, such as listening to music. De Niet and collegeaus (2009) examined 16 systematic reviews on non-pharmacological interventions to improve sleep quality in insomnia and found a moderate effect for music-assisted relaxation, making it more successful than any of the other interventions studied (for which no effect or a small effect was found). A more recent Cochrane review on music for insomnia specifically (Jespersen et al., 2015) looked at six studies and confirmed the presence of moderate benefit of music for sleep quality. The benefit of music for sleep quality in clinical settings was confirmed with self-report and polysomnography in a meta-analysis of ten studies (Wang et al., 2014). Indeed, music has the additional benefits of reducing heart rate, systolic, and diastolic blood pressure (Loomba et al., 2012) making it suitable for the use of improving sleep in medical settings, such as in cardiac units (Cheraghi et al., 2015; Ryu et al., 2012). A meta-analysis of six studies also showed the efficacy of music interventions on sleep quality among elderly people. The benefit of music for sleep quality in individuals even without diagnosed sleep disorders has also been shown in a meta-analysis of six studies by Tang et al (2022).
A sample of individuals that use music listening to help them sleep were asked to suggest why it aids their sleep. A variety of reasons were suggested, such as, music offering unique properties that stimulate sleep, it being part of a normal sleep routine, it induces a physical or mental state conducive to sleep, and it is masking external stimuli that disrupt sleep (Trahan et al., 2018). A later literature review examined the effectiveness of different psychological approaches for using music to improve sleep quality and sleep onset. Findings of this review indicated clear support for music to help sleep and confirmed the mechanisms outlined in Trahan et al (2018) including distraction, relaxation and enjoyment (see Dickson & Schubert, 2019 for more information). These findings are in line with evidence that music is more effective in improving sleep quality in students than listening to audiobooks and therefore does not just mask sounds (Harmat et al., 2008).
The type of music used for treating insomnia is important. Shum et al. (2014) found sleep quality to improve when participants listened to pieces of soft instrumental music of different genres which were roughly 60–80 beats per minute, compared to a control group where no instructions were provided on what to do before sleep. Instrumental music has similarly been shown to improve sleep quality in coronary care patients, when compared to a control group (Cheraghi et al., 2015). Instrumental music may have an advantage over lyrical music when listened to at bedtime, as the lyrics may stimulate intrusive thoughts, require concentration or if familiar, even provoke an urge to sing alone (Van den Tol & Giner-Sorolla, 2016, 2022). However, Cheraghi et al. (2015), did not test the effect of instrumental (non-lyrical) music against music with lyrics and this remains an area in need of further research.
Another key parameter is whether or not the music is familiar to the listener. On one hand, familiar music may be comforting and promote stress reduction which might help sleep, with a meta-analysis of 22 studies showing that familiar music has been found to decrease stress and therefore arousal (Pelletier, 2004). On the other hand, it may draw greater attention from the listener and distract from the attempt to fall asleep. One study explored the effect of participant-preferred music compared to researcher-selected music, but no difference was found between the sleep quality of the two groups (Chang et al., 2012). However, the study was underpowered (with just 10 participants in one of the groups) and participants were not asked to rate the researcher-selected music in terms of their preference, limiting the usefulness of these findings. Our study will overcome both of these limitations.
The current research
It is well established that music improves sleep quality and reduces insomnia severity but the most effective type of music for aiding sleep is not yet known. Therefore, the present study aims to explore if (a) familiarity with the music and (b) the presence of lyrics affect music’s ability to aid sleep and if these two interact in this effect. This research is guided by the following four hypotheses (which were grounded in previous research; Cheraghi et al., 2015; Harmat et al., 2008; Pelletier, 2004; Shum et al., 2014; Wang et al., 2014):
Listening to music will increase sleep quality and decrease insomnia compared to baseline levels.
Listening to music without lyrics before sleep will increase sleep quality and decrease insomnia severity more than listening to music with lyrics.
Listening to familiar music before sleep will increase sleep quality and decrease insomnia severity more than listening to unfamiliar music.
The effect of lyrics on sleep quality and insomnia severity will vary depending on the familiarity of the music.
To test these hypotheses, participants are asked to listen to music while they fall asleep, every night for seven nights. There are four conditions: familiar songs with lyrics, familiar songs without lyrics, unfamiliar songs with lyrics and unfamiliar songs without lyrics. Sleep quality and insomnia severity will be measured before and at the end the experiment and compared across these groups.
Method
Participants
An opportunity sample of 169 participants was recruited over 4 months, through a combination of social media, the SONA website (a system where students are awarded points for participating in other students’ studies) of the School of Psychology, Sport Science & Wellbeing, at the University of Lincoln, and through word of mouth. Participants were required to be aged 18 years and over, have normal or corrected-to-normal hearing and competence in written English. 15 participants were excluded from the final sample, as they had not completed the study to 100%, making the final number of participants in the sample 154. 30 participants were male, 121 were female, and 3 non-binary, with ages varying between 18 and 57 years (M = 21, SD = 6.50).
Materials
Sleep questionnaires
Participants completed both the Pittsburgh Sleep Quality Index (PSQI; Buysse et al., 1989) and the Insomnia Severity Index (ISI; Morin et al., 2011). The PSQI is the most widely used questionnaire in sleep research and consists of 19 self-report questions to determine the participant’s sleep quality. Items are score on a 0 (no difficulty at all) to 3 (severe difficulty) Likert scale. The items of this questionnaire combine to form the seven component scores of sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, sleep medicines and daytime dysfunction. These seven scores are then combined to form the global score, which determines the participant’s sleep quality in a range of 0 to 21 (the higher the score the worse the sleep quality). A score from 0 to 4 indicates ‘good’ sleep quality; a score of 5 or above indicates a poor sleep quality. Examples of questions in the PSQI include ‘What time have you usually gone to bed?’ and ‘During the past month, how much of a problem has it been for you to keep up enthusiasm to get things done?’. The test-retest reliability of the PSQI is 0.99 and the overall Cronbach’s alpha coefficient is 0.85 (Backhaus et al., 2002), making it reliable when measuring sleep quality. In the default version of the PSQI the questions ask about the previous month; however, it is widely adapted to shorter time periods, and in our study was adapted to ask about the previous week in order to avoid overlapping time periods in the pre- and post-intervention questionnaires.
The ISI consists of seven self-report Likert scale questions to determine insomnia severity across the previous two weeks. Items are scored on 0 (none) to 4 (very) Likert scale. The scores for all seven items are combined to create an overall insomnia severity score. Scores can range from 0 to 28. There are four total score categories which place participants into no clinically significant insomnia (a score of 0–7), subthreshold insomnia (a score of 8–14), clinical insomnia of moderate severity (a score of 15–21) and severe clinical insomnia (a score of 22–28). Examples of questions include, ‘How satisfied/dissatisfied are you with your current sleep pattern?’ and ‘How noticeable to others do you think your sleeping problem is in terms of impairing your quality of life?’. The overall Cronbach’s alpha coefficient of the ISI is around .90 (Morin et al., 2011) and the ISI has a test-retest reliability between .72 and .80 (Chung et al., 2011). The ISI is widely used in insomnia research and, like the PSQI, the time period covered is considered adaptable from the default of two weeks, and was again adapted to 1 week in the current study.
Songs
The list of 82 songs that participants had to indicate as familiar or not, was formed of the 1st and 100th song from every year. These songs were used because number one songs in any given year would be a lot more familiar than songs that were number one hundred (with songs less popular than that not being on the billboard). This would therefore provide likely varying levels of familiarity for participants. These songs were found on the website Billboard (2019) where a list can be found of each year’s most popular 100 songs. The current study uses the songs from 1970 to 2019, excluding the years where the non-lyric versions were not available. The principal genre of the songs was found through a google search, with 35.3% of songs pop, 28% R&B, 11.0% rap/hip hop, 9.8% rock, 4.9% dance, 4.9% country, 4.9% indie, and 1.2% gospel. Instrumental versions of the songs in the list were used for the non-lyric conditions. For most songs the instrumental version was released by the artists themselves. The remainder had been created by other artists based on the originals. For this latter group, the songs were checked to ensure that they did not deviate from the original pieces on anything but the lyrics. The complete list of songs used – and links to the lyrics and non-lyrics versions of them – can be found in Supplementary Information S1.
Design and assignment to conditions
The study used a factorial 2 × 2 between-subjects design with factors lyrics (lyrics, no lyrics) and familiarity (familiar, unfamiliar). Participants were allocated to one of four groups using simple random sampling based on the order in which they chose to sign up to the study, with each participant being assigned to the next group from the previous one, wrapping around to the first group every fourth participant. This ensured that experimenters were not involved in the allocation beyond the simple application of a fixed rule and could not bias the sample towards any particular group. The four groups represented the 2 × 2 combination of familiarity and lyrics factors: familiar music with lyrics, familiar music without lyrics, unfamiliar music with lyrics, and unfamiliar music without lyrics group.
Participants were asked to indicate if they were familiar or not with a list of songs provided at the beginning of the study. On the basis of this, personalised playlists were developed for each participant. For example, if someone was assigned to unfamiliar songs with no lyrics, their playlist would consist of the non-lyric versions of the songs they had indicated as unfamiliar. The playlists were made available on YouTube and capped at 30 minutes duration (approx. 8 songs).
Procedure
After initial interest was expressed, potential participants were directed to the study on the Qualtrics survey platform (either by a link shared with them via email, social media, or SONA). Before the study began participants were presented with the participant information sheet and were asked to consent to participating in the study by ticking a box. The study began by asking participants to answer demographic questions (age and gender) and to provide an email address for the playlist to be sent to. They were then asked to fill in the PSQI and ISI. After this, they were presented with a list of 82 songs and asked to indicate if they were familiar with them or not. Upon completion of this initial phase participants were made aware that they would be contacted and provided with a playlist that they could then use for the sleep study and would be given further instructions.
Participants were then assigned to one of the four conditions and emailed a link by the researchers to their personalized YouTube playlist. Participants were directed to listen to their playlist on shuffle while they fell asleep, each night for seven consecutive nights, at a volume where they could hear the music but not hinder their sleep quality. After the week was complete, participants were emailed another link and asked to complete the PSQI and the ISI again. They were then debriefed via the Qualtrics study link and thanked for their participation, which concluded the study. Ethical approval was granted for this procedure by the University of *** (anonymised for review) Ethics Committee and given the approval code 2022_10682.
Data analysis
The data was analysed using IBM SPSS Statistics 28. Preliminary analysis focused on compliance monitoring using YouTube analytics, distribution testing and descriptive statistics. The difference in sleep quality and insomnia severity before and after the week of listening to music was calculated using the pre-post difference scores for the PSQI and ISI, representing the change over time (with higher scores showing a greater improvement). The effect of two factors on changes to sleep–the familiarity of music (familiar and unfamiliar) and the presence of lyrics (lyrics and no lyrics) – was determined by a MANOVA and univariate ANOVAs.
Results
Playlist compliance
To establish if participants were listening to the playlists they were given, YouTube analytics were explored. While not an exact tool, this was intended to give us some indication of compliance by participants. Across the 154 participants who completed the study, playlists were played an average of 14.79 times, which suggests that non-compliance was not a significant problem. However, the data appeared to be somewhat unreliable, with three playlists showing more than 100 views and a several others with none, even when that list was verified as having been played during a test session. Some participants also reported copying the playlist to their own list, which inadvertently prevented us from accessing the viewing figures. As such, no further analysis is presented here.
Data preprocessing
Normality of the data was confirmed through visual inspection of Q-Q plots with the data not varying in distribution across the four groups (KS-test, all p > .05). Outliers were calculated using the median and interquartile range (IQR), with values above the recommended value of 1.5 excluded as outliers (Tukey, 1977). A total of six participants were excluded as outliers on a case-wise basis using this procedure. This left data from 148 participants included in the final analysis. A post hoc test carried out in G*Power (Faul et al., 2009) and based on the main MANOVA analysis revealed that with this sample the power to achieve a medium effect size of f = 0.25 was 94.6% (with an effect size of f = 0.253 detectable at 95% power).
Age was examined as a potential covariate, but Pearson’s correlation tests revealed no significant association with either the PSQI difference score, r(148) = −.022, p = .79, or the ISI difference score, r(148) = −.003, p = .97, so this was not included in further analyses. Similarly, gender was examined as a potential factor (comparing male with female with a t-test; three non-binary participants are excluded from this analysis due to insufficient numbers) but showed no significant effect on the PSQI difference score, t(145) = .372, p = .71, or the ISI difference score, t(145) = −.017, p = .99, and so also not included in further analyses.
Descriptive statistics
Table 1 shows the descriptive statistics for all four conditions for the before, after and difference scores for ISI and PSQI. This shows the mean change in ISI and PSQI scores as well as the difference to show the change after listening to music. While participants were randomised into the different groups, some minor differences were observed between the groups prior to the intervention in ISI score, F(1, 144) = 2.891, p = .038, η2 p = .057, where participants in the familiar without lyrics group had somewhat lower symptoms of insomnia. Similarly, participants in the unfamiliar with lyrics group showed somewhat poorer sleep quality than the other groups, F(1, 144) = 3.208, p = .025, η2 p = .063. It is important to note that these differences do not explain our reported findings, which were based on difference scores accounting for this initial variability and showed a pattern that involved all four groups (in an interaction effect). Violin plots showing the distribution of the scores in each group before and after the data are presented in Figure 1.
Descriptive statistics.
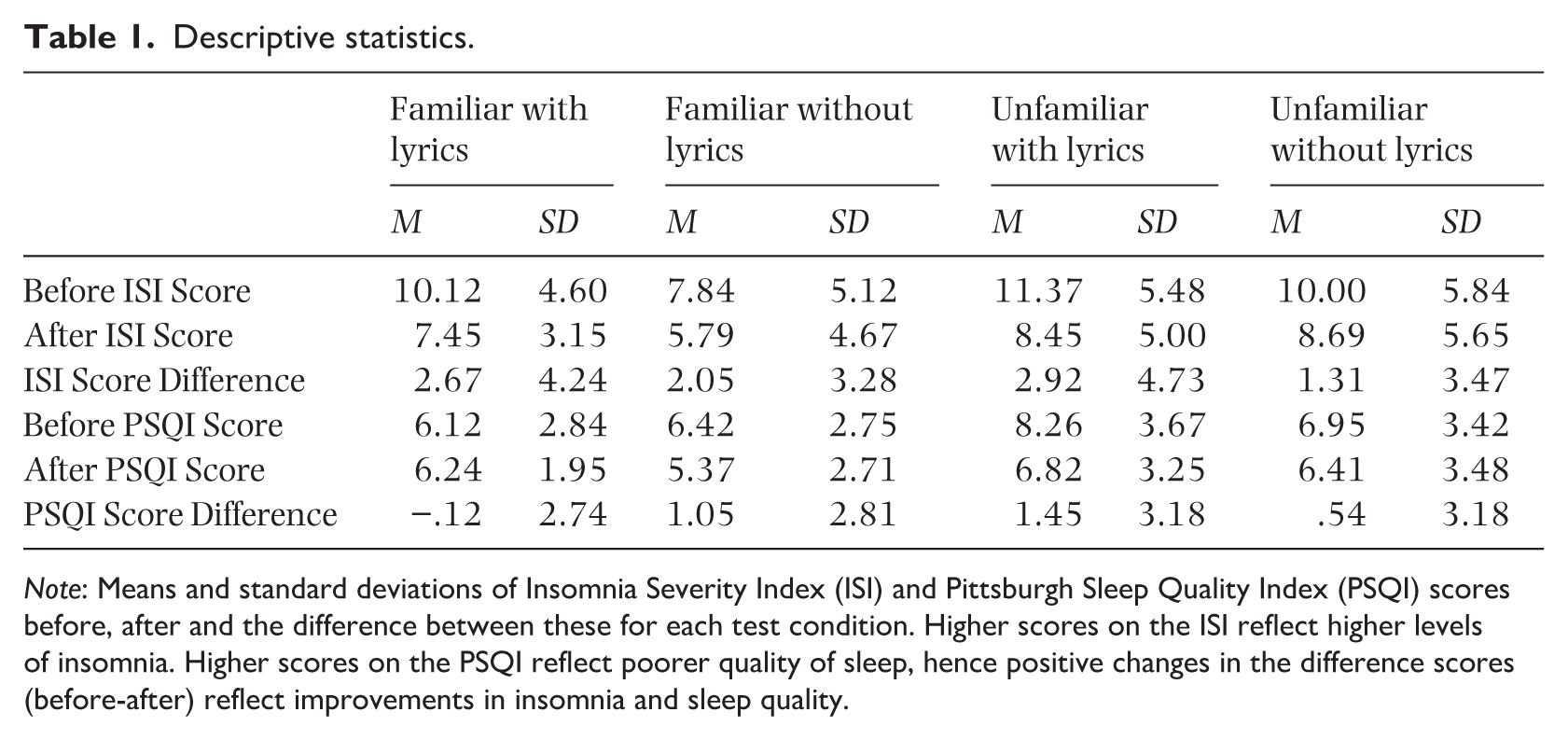
Note: Means and standard deviations of Insomnia Severity Index (ISI) and Pittsburgh Sleep Quality Index (PSQI) scores before, after and the difference between these for each test condition. Higher scores on the ISI reflect higher levels of insomnia. Higher scores on the PSQI reflect poorer quality of sleep, hence positive changes in the difference scores (before-after) reflect improvements in insomnia and sleep quality.
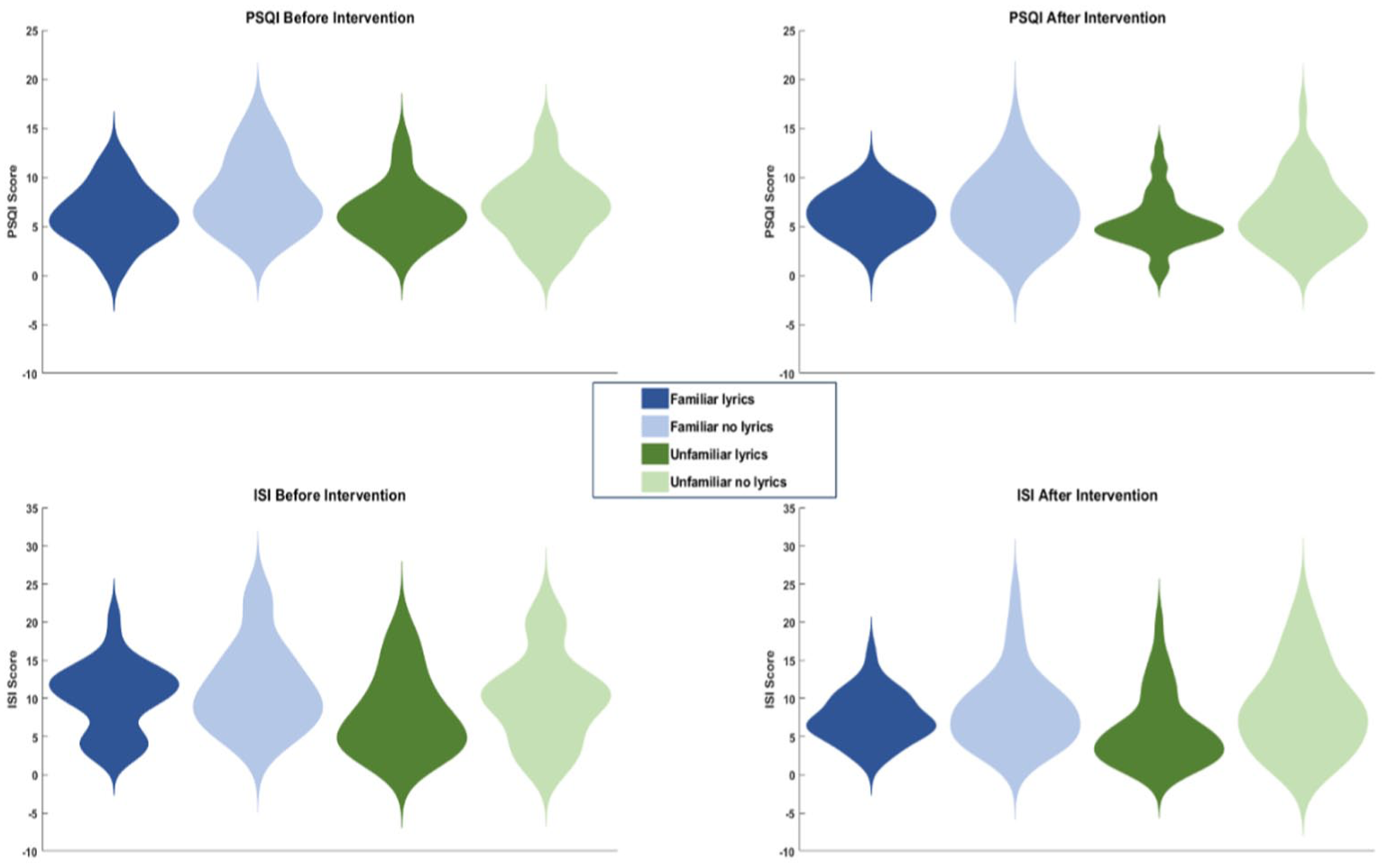
This figure shows distributions of scores in each group before and after the intervention, for both PSQI (top row) and ISI (bottom row). Kernel density estimation is used for each plot; note that this can lead to tails of the distributions showing unobtainable values (below zero).
Descriptive statistics
Table 1 shows the descriptive statistics for all four conditions for the before, after and difference scores for ISI and PSQI. This shows the mean change in ISI and PSQI scores as well as the difference to show the change after listening to music. While participants were randomised into the different groups, some minor differences were observed between the groups prior to the intervention in ISI score, F(1, 144) = 2.891, p = .038, η2 p = .057, where participants in the familiar without lyrics group had somewhat lower symptoms of insomnia. Similarly, participants in the unfamiliar with lyrics group showed somewhat poorer sleep quality than the other groups, F(1, 144) = 3.208, p = .025, η2 p = .063. It is important to note that these differences do not explain our reported findings, which were based on difference scores accounting for this initial variability and showed a pattern that involved all four groups (in an interaction effect). Violin plots showing the distribution of the scores in each group before and after the data are presented in Figure 1.
Does music improve sleep?
ISI scores significantly decreased, t(147) = 6.79, p < .001, from before the music intervention (M = 9.82, SD = 5.41) to after it (M = 7.61, SD = 4.85), suggesting an improvement in insomnia severity. Similarly, PSQI scores also significantly decreased, t(147) = 3.05, p = .03, from before (M = 6.97, SD = 3.28) to after (M = 6.21, SD = 2.96) the music intervention, indicating an improvement in sleep quality. Together these results suggest that the music intervention improved both measured aspects of sleep.
The effect of familiarity and lyrics on PSQI and ISI
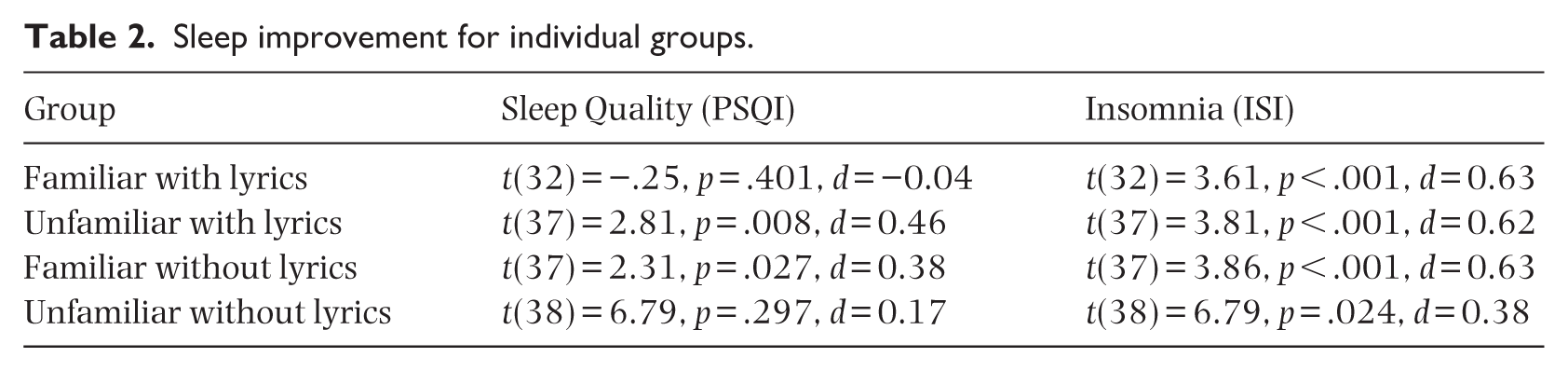
A two-way between-subjects MANOVA was conducted to assess the effect of familiarity and lyrics on the improvements seen in the PSQI and ISI scores. Homogeneity of error variances and covariances were confirmed by Levene’s and Box’s statistics respectively for both dependent variables (all p > .05). The MANOVA showed a significant interaction between familiarity and the presence of lyrics in the effect on PSQI difference score, F(1, 144) = 4.458, p = .036, η2 p = .030. This was driven by a notable improvement in sleep quality when listening to familiar music that did not use lyrics (vs little improvement when lyrics were present), whereas for unfamiliar music the presence of lyrics was actually helpful (see Figure 2(a)). There was no main effect of lyrics, F(1, 144) = .072, p = .789, η2 p = .001, or familiarity, F(1, 144) = 1.143, p = .287, η2 p = .008, on PSQI difference score. The ISI score did not show a main effect of familiarity, F(1, 144) = .141, p = .708, η2 p = .001, or lyrics, F(1, 144) = 2.914, p = .090, η2 p = .020, and no significant interaction was observed, F(1, 144) = .586, p = .445, η2 p = .004; see Figure 2(b). These results suggest that the effect of music on sleep quality depends on the particular combination of familiarity and lyrics (with either familiarity or lyrics most helpful, but not both or neither), while sleep insomnia severity does not seem to be significantly affected by either. The individual group results (see Table 2) support the interaction effect and confirm that the benefit of music on sleep quality (PSQI) depends on the presence of lyrics for unfamiliar music and the absence of lyrics in familiar music. Familiar music with lyrics, or unfamiliar music without lyrics, offered no significant benefit to sleep quality, with the weakest effect seen for familiar music with lyrics.
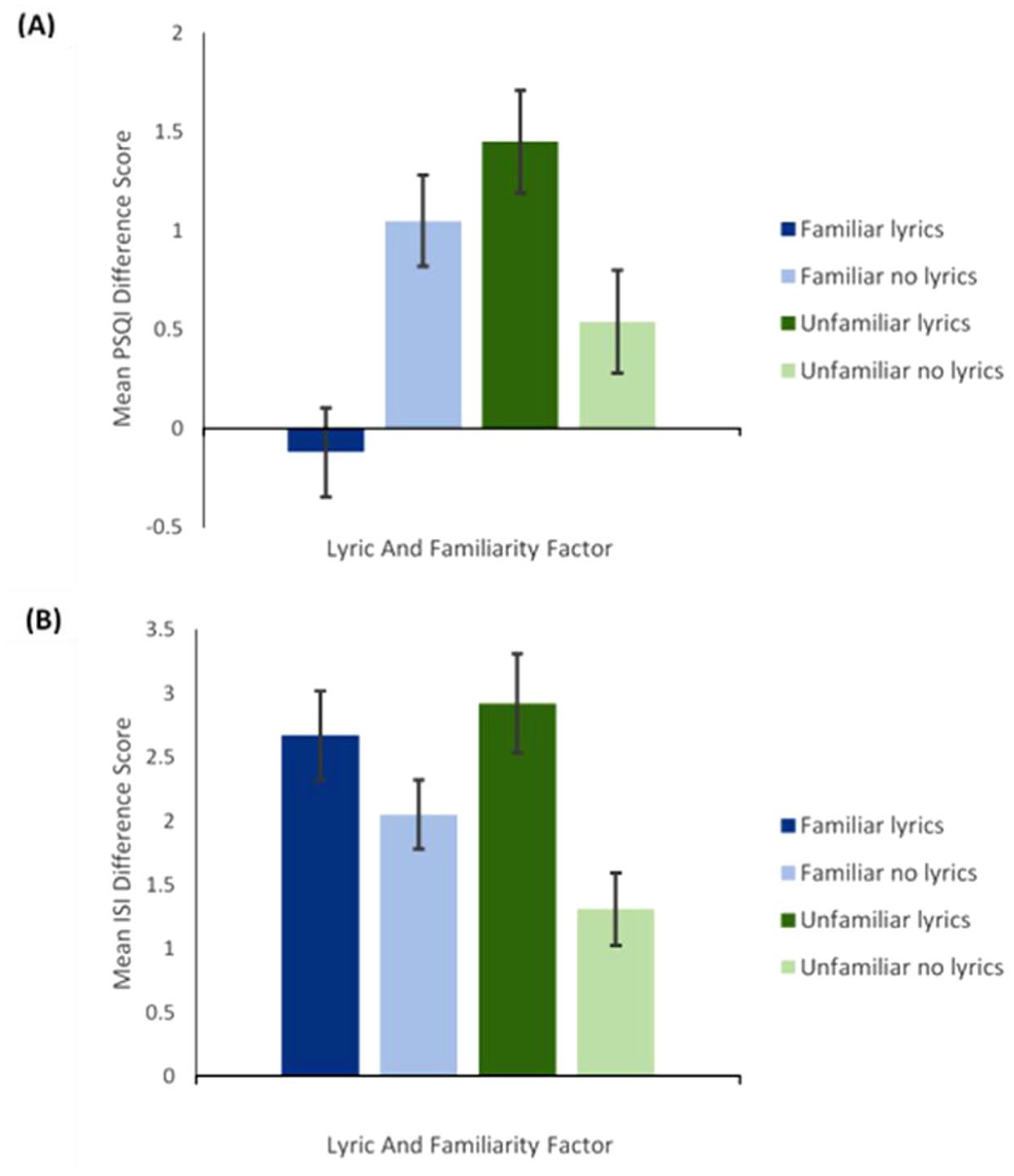
This figure shows the mean difference in (a) PSQI scores and (b) ISI scores, for all conditions. Error bars represent ±1SE.
Sleep improvement for individual groups.
Discussion
The principal objective of this study was to explore the effect of familiarity and lyrics on sleep quality and insomnia severity. This study was supported by four hypotheses. Results of this study indicated a significant effect of music on sleep quality and insomnia severity when comparing pre and post-test scores on the PSQI and ISI. This supports our first hypothesis and previous literature suggesting that music is an effective sleep aid by increasing sleep quality and decreasing insomnia severity (Harmat et al., 2008; Wang et al., 2014) and that music is therefore a viable treatment for sleep difficulties.
Familiar music and music without lyrics were expected to improve sleep quality and decrease insomnia severity the most, with a prediction that the effect of lyrics would depend on the familiarity of the music (our second and third hypotheses). We did not find evidence to support our hypothesis that familiar music would have a greater benefit than unfamiliar music in terms of sleep quality and insomnia severity. Similarly, we found no evidence to support the idea that overall music without lyrics would be more beneficial for sleep quality and insomnia severity. However, caution must be exercised when interpreting these null main effects as we did observe an interaction between the two factors on sleep quality, with the greatest benefit seen for familiar music without lyrics and unfamiliar music with lyrics. This interaction was not present for insomnia severity, however, which was unaffected by either factor. In other words, our fourth hypothesis, that the effect of lyrics on sleep quality and insomnia severity will vary depending on the familiarity of the music was confirmed only for sleep quality.
Our findings support previous literature suggesting music is an effective sleep aid by increasing sleep quality and decreasing insomnia severity (Harmat et al., 2008; Wang et al., 2014) and that music is therefore a viable treatment for sleep difficulties. Previous literature has concluded that instrumental music (Cheraghi et al., 2015; Shum et al., 2014) and familiar music (Pelletier, 2004) are effective in increasing sleep quality. We did however not find this as a main effect, but rather found an interaction effect between both variables. An important novelty in our work is not only the examination of these two factors together and how they might interact, but also the finding that as well as familiar music without lyrics, unfamiliar music with lyrics may also be beneficial, something not previously seen or discussed in the literature.
The divergent findings between sleep quality, where a significant familiarity-lyrics interaction was seen, and insomnia symptoms, where no such effect was observed, was an additional interesting finding. While the precise reasons for this cannot be ascertained in the current study, we suggest that one possible explanation is that they are measuring different things. Listening to familiar music without lyrics or unfamiliar music with lyrics may lead to improved sleep. By contrast, familiar music with lyrics may be too stimulating, and unfamiliar music without lyrics not beneficial enough, such that neither lead to the same benefit for sleep quality. This is quite different to the various reasons given for why music may help with insomnia symptoms or hasten sleep onset, such as blocking out intrusive thoughts or noises.
Implications
The combination of familiarity and lyrics in the effect of music on sleep quality has not been previously examined, so this significant finding is novel and suggests that both familiarity and the presence or not of lyrics are worthy of consideration in future studies which look at sleep quality. The findings of this study are important as they help to identify the most effective type of music to improve sleep quality, including specifically the combination of familiarity and lyrics. The findings of this study have potential implications for the general population (given the high proportion of individuals who listen to music at bedtime (Trahan et al., 2018), those with sleep and co morbid conditions (Blaty & DelRosso, 2022; Freeman et al., 2020; Ghosh et al., 2014; Goldberg, 2011; Meerlo et al., 2015; Penninx et al., 2013) and for clinical practice. The findings of this study could also be used in clinical environments such as hospital wards. Patients on hospital wards often have poor sleep due to raised noise levels (Aparício & Panin, 2020). Inadequate sleep in hospital patients can weaken the immune response, decrease the rate of wound healing, increase insulin resistance, and decrease pain tolerance (Bevan et al., 2019; Shaw, 2016). Music to aid sleep has been applied to hospitalised burn patients and found to improve their sleep quality and subsequently decrease the intensity of their pain (Ardabili et al., 2016). The findings of the present study also suggest that a broad range of music is effective in increasing sleep quality, making it easy to implement in hospitals, implying it is an accessible form of treatment. If the music is likely to be unfamiliar to patients, our study suggests that music with lyrics may be more effective in this context.
Strengths, limitations, and considerations for future research
The study has some key strengths as well as some limitations and opportunities for further research in this area. The first key strength is to combine familiarity and the presence or absence of lyrics in the same study. This is important because one has the potential to influence the benefit for sleep of the other and indeed this is exactly what we found in our results. This suggests that future studies looking to consider one of these factors should also pay attention to the other. The second key strength is that we first systematically selected the overall sample of songs to use (no. 1 and no. 100 in the charts for every year from 1970 to 2019); this is in contrast to the vast majority of studies looking at the effect of music on sleep where the music selection is relatively arbitrary or conforming to the researcher’s idea of calming music. Third, we created fully individualised playlists based on familiarity, while not simply allowing participants to choose their own music (with the difficulties for systematic comparison that this can create); to our knowledge we are the first study to do this. Finally, our sample size of 154 complete participations is one of the highest in this area (it is more than double the maximum sample size in any study in the Cochrane review of Jespersen et al., 2015, for example).
There are some limitations here as well. First, this was not a clinical trial and as such we did not have a non-music control group to evaluate the overall effect of music vs no music. This is partly because this has already been examined in a number of previous studies and meta-analyses and partly because this was not the aim of our study. As such, while our results show a clear improvement in sleep quality and insomnia symptoms across the intervention, we cannot be sure that this is due to the music. Second, although we were rigorous in the selection of our music and creation of the playlists used, we have not carried out any audio analyses of the songs used. That is again partly because this has been looked at in previous studies (such as Dickson & Schubert, 2022) and partly because it is beyond the scope of the current study and not central to our research questions. However, we have provided the list of and links to all the songs used in case researchers wish to investigate this in a future study.
These findings may additionally not generalise to music which has originally been created to be enjoyed without lyrics This research compared the effects of original tracks with lyrics, to the same tracks with lyrics removed. While this approach allows to illuminate cofounding variables for both types of music, there is a possibility that music which is originally composed to be enjoyed without lyrics, on average has different music features, hence having different effectiveness. In addition, the tracks in our songs may also be different in terms of them still prompting the listener to sing along. As pointed out in Scarratt et al. (2023), lyrics are found less commonly on the average music on a sleep music playlist. This is likely due the urge to sing along with music potentially keeping listeners from sleeping. Our findings suggest that familiar music improved sleep quality (but not insomnia) more without lyrics, while unfamiliar music improves sleep quality more if lyrics are present. These findings may likely occur due to non-familiar music not urging listeners to sing along, and removing lyrics from familiar music reducing the urge to sing along. Future research may want to explore this further.
Finally, there are inevitably many other variables that could potentially influence the findings that we have not been able to include. The use of API (application programming interface) is becoming a more popular method for pulling pre-calculated audio features (such as: loudness, energy, instrument choice, dance value, valance, tempo, liveness, and amount of speech) from music pieces in large datasets (by e.g. Kirk & Timmers, 2024; Scarratt et al., 2023) an could also provide valuable for future research to explore the role of musical factors into the effectiveness of the music for improving sleep quality. Exploring psychological motivations for music listening may also provide useful for furthering our understanding on how and why music can improve sleep quality, A listeners, music preference, connection with the music, or the perceived aesthetic value and novelty of a piece of music (Van den Tol & Edwards, 2013, 2014; Van den Tol & Giner-Sorolla, 2016, 2022) have all been found to predict how well people are able to down-regulating negative moods and arousal levels (Coulthard et al., 2023; Van den Tol & Giner-Sorolla, 2022; Van den Tol et al., 2016, 2020, 2022) by listening to music. Varying the length of days over which similar studies are conducted may also be important to establish if listening to music has a ceiling effect and if it is only effective for a certain period of time (Wang et al., 2014).
Concluding remarks
To conclude, the present study is the first of its kind to explore the effect of both familiarity of music and the presence of lyrics, on sleep quality and insomnia severity. The findings of this study suggest that music effectively improves sleep, yet familiar music improves sleep quality more without lyrics, while unfamiliar music improves sleep quality more if lyrics are present. These findings are novel and important for furthering our understanding of the use of music to help sleep.
Supplemental Material
sj-docx-1-msx-10.1177_10298649261422641 – Supplemental material for Do lyrics and familiarity of music listened to at night affect sleep quality and insomnia?
Supplemental material, sj-docx-1-msx-10.1177_10298649261422641 for Do lyrics and familiarity of music listened to at night affect sleep quality and insomnia? by Eleanor Stobart, Annemieke Van den Tol and Simon J. Durrant in Musicae Scientiae
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.