
Abstract
Background:
Early antibiotic administration in sepsis improves patient survival. Treatment with antibiotics should cover potential pathogens and should avoid overusing broad-spectrum antibiotics. We have to identify patients who have high risks of infection with drug-resistant organisms.
Objectives:
A retrospective cohort study was conducted to identify potential risk factors associated with bloodstream infections with drug-resistant organisms to help the choice of empirical antibiotics in the emergency department.
Methods:
Adult patients with bloodstream infection diagnosed by blood culture in the emergency department in the period of 1 January 2020 to 31 December 2020 were included. Clinical features including chronic medical illnesses, clinical presentation and severity, and patients’ outcomes were identified in the electronic medical records. Bloodstream infection with drug-resistant organisms is defined as positive blood culture with bacteria resistant to either (1) amoxicillin/ clavulanic acid AND ceftriaxone or (2) amoxicillin/ clavulanic acid or ceftriaxone PLUS amikacin or levofloxacin. Univariate and multivariate analyses were conducted to identify risk factors associated with the study outcome.
Results:
Among 105 patients with bloodstream infection, 17% were caused by drug-resistant organisms. Multivariate analysis showed that age is a risk factor associated with bloodstream infection with drug-resistant organisms (odds ratio: 1.04, 95% confidence interval: 1.0–1.08, p = 0.03).
Conclusion:
In conclusion, age is a significant risk factor for drug-resistant bloodstream infection in emergency department patients. Further research may be needed to find out the relationship between frailty and infection with drug-resistant organisms.
Introduction
Many patients present to emergency department with sepsis. Early administration of antibiotics reduces mortality in sepsis patients.1,2 So, patients with sepsis often receive their first dose of antibiotics in the emergency department after blood culture is taken.
As microbiological workup takes time, emergency physicians have to decide the choice of empirical antibiotics based on limited information at presentation. The antibiotic chosen should cover potential pathogens, but overuse of broad-spectrum antibiotic should be avoided. The choice of antibiotic depends on the likely source of infection and the likelihood of drug-resistant bacterial infection. Doctors can often identify the likely source of infection with history and physical examination, while determining the likelihood of infection with drug-resistant organism is difficult at the emergency department.
Previous studies have identified risk factors associated with infection of multidrug-resistant organisms, including advanced age, diabetes mellitus, immunosuppression, and recent antibiotic use.3 –5 These studies include inpatient cases or only focus on a particular source of infection, and may not reflect the wide spectrum of patients encountered in the emergency department.
This study aims to evaluate the risk factors associated with bloodstream infection with drug-resistant organisms in emergency department. The secondary objective of this study is to describe the clinical and microbiological features in patients with bloodstream infection in emergency department.
Methodology
It is a retrospective chart review for the period 1 January 2020 to December 2020 conducted in an emergency department in Hong Kong.
Subject identification and data collection
Study subjects include adult patients with suspected sepsis and had bloodstream infection diagnosed by blood culture taken at the emergency department.
Patients who were suspected to suffer from sepsis by doctors in emergency department received antibiotic treatment after blood culture in the emergency department. Blood cultures were taken by doctors in the emergency department or phlebotomists with special training in aseptic technique for blood culture. Patients were identified in the electronic medical records, and the following clinical information was retrieved: patients’ age, sex, chronic illnesses (hypertension, diabetes, cerebrovascular accident, chronic obstructive pulmonary disease, cirrhosis), use of immunosuppressants (intravenous or oral chemotherapy, targeted therapy, disease-modifying agents, biological agents, long-term steroid usage equivalent to >0.2 mg/kg/day of prednisolone), active cancer (under active treatment or palliative care), hospital admission within previous 30 days, residence in nursing homes; clinical presentation: blood pressure and pulse at emergency department triage, need for oxygen therapy, the use of vasopressors in emergency department, the admission diagnosis and presumed source of sepsis, first dose of antibiotics given at emergency department; patient outcome: presence of neutropenia on admission, microbiological results of blood culture including organism isolated and antibiotic susceptibility, intensive care unit (ICU) admission, 30-day mortality, and inpatient mortality. Patients were excluded if the blood culture results were treated as contaminants by the inpatient medical team. Written informed consent was not necessary because no patient identifier has been included in the article, and it was waived by the research ethics committee.
Definition of outcome
Several antibiotics are stocked in our emergency department for urgent use. They are divided into broad-spectrum “big gun” antibiotics and non-“big gun” antibiotics. “Big gun” antibiotics is defined by the hospital antibiotic stewardship program, and the use of these antibiotics is audited. These “big gun” antibiotics include cefoperazone/ sulbactam (sulperazon), piperacillin/ tazobactam (tazocin), meropenem, and vancomycin. Non-“big gun” antibiotics include other intravenous antibiotics stocked in the emergency department: amikacin, amoxicillin/ clavulanic acid (augmentin), ceftriaxone, clindamycin, levofloxacin, and metronidazole.
The Centers for Disease Control and Prevention (CDC) defines multidrug-resistant organisms as “micro-organisms that are resistant to one or more classes of antimicrobial agents.” 6
The aim of the study was the identification of bacteremia requiring the use of “big gun” antibiotics in emergency department, so bacteremia with drug-resistant organisms is pragmatically defined as positive blood culture with microorganism that is resistant to either (1) amoxicillin/ clavulanic acid AND ceftriaxone or (2) amoxicillin/ clavulanic acid or ceftriaxone PLUS amikacin or levofloxacin, as these organisms likely require the use of “big gun” antibiotics.
Sample size calculation
We estimated that around 50% of the patients with bacteremia are nursing home residents. The incidence of drug-resistant organism carriage in these patients is estimated to be 0.4 from previous study and local experience. 7 With an alpha of 0.05 and beta of 0.2, the estimated sample size is 107 according to the formula proposed by Hsieh et al. 8
Statistical analysis
Statistical analysis was performed using R statistical software (version 4.1.1). Continuous data were presented as mean with standard deviation, and categorical data were presented as percentage. Univariate analysis and multivariate analysis with logistic regression were performed for the identification of risk factors associated with bloodstream infection with drug-resistant organisms. All factors with potential association with the outcome were included in the univariate analysis. In addition, 95% confidence interval (CI) was calculated for the variables, and two-tailed p-value of less than 0.05 is deemed statistically significant. Fisher’s exact test was used to compare categorical variables where appropriate.
Results
During the study period, 913 patients had blood culture taken at the emergency department, and 105 patients with bloodstream infection were identified, as detailed in the study flowchart (Figure 1).
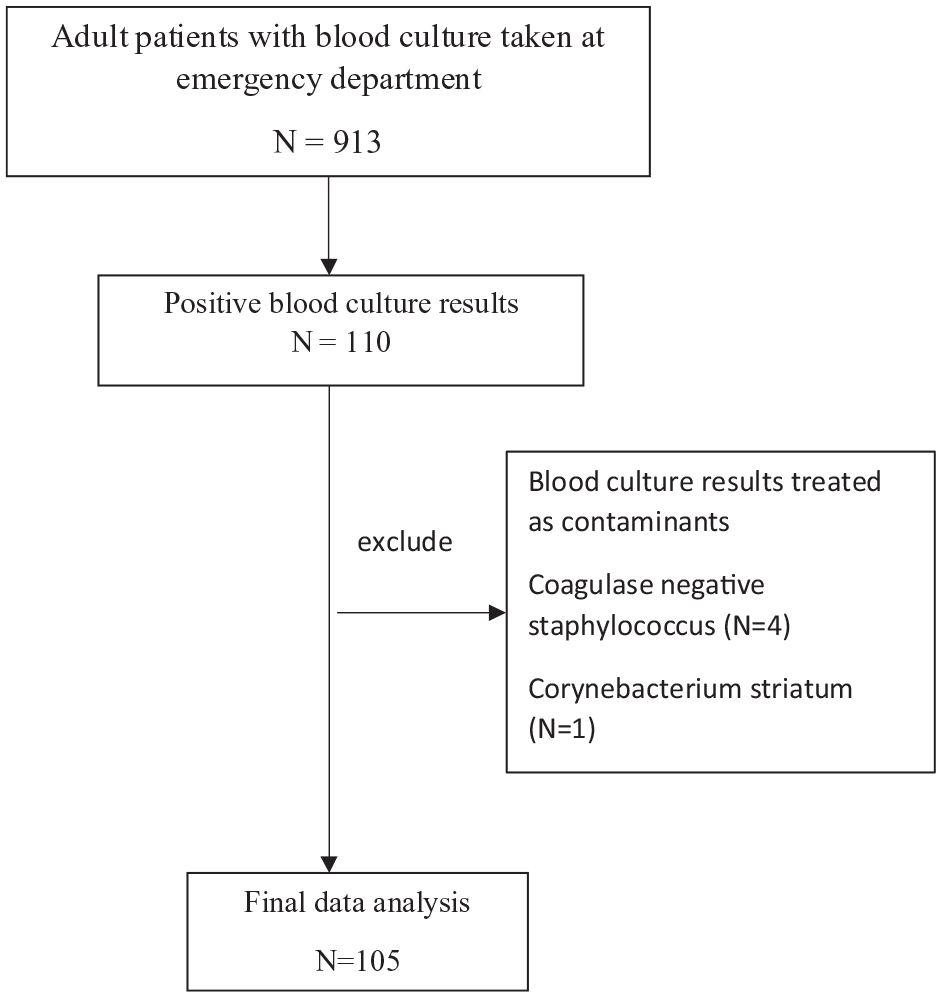
Study flowchart.
Table 1 shows the patients’ characteristics. A significant proportion of them were nursing home residents (28.6%), and around one-third of them had been hospitalized in the previous 30 days, and 29.5% of patients had diabetes mellitus. Furthermore, 20.9% of these patients suffered from septic shock, requiring the use of vasopressors in the emergency department. Only 1.9% of patients were neutropenic. Drug-resistant organisms were found in 17% of the cases, and 30-day mortality rate was 15%.
Characteristics and clinical features of patients.
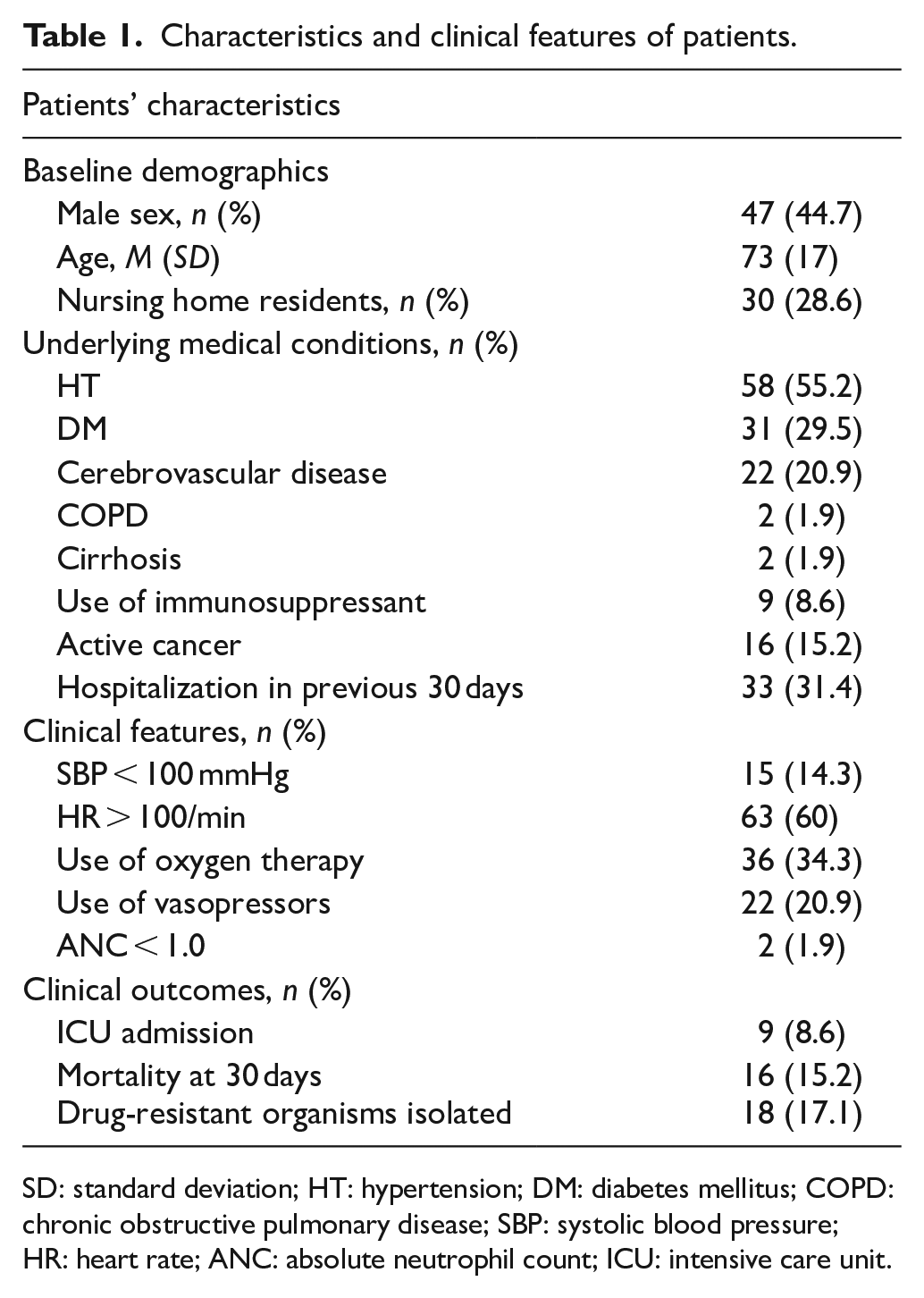
SD: standard deviation; HT: hypertension; DM: diabetes mellitus; COPD: chronic obstructive pulmonary disease; SBP: systolic blood pressure; HR: heart rate; ANC: absolute neutrophil count; ICU: intensive care unit.
Univariate logistic regression for the risk factors associated with drug-resistant bacteremia shows that age is a significant risk factor; and every 1-year increase in age increases the risk by 4%. Being nursing home resident is another significant risk factor, with odds ratio of 3.1. Other factors, including the underlying medical conditions, severity of clinical presentation, and the source of sepsis, are not associated with drug-resistant bloodstream infection (Table 2). Chronic obstructive pulmonary disease, cirrhosis, and neutropenia were excluded in univariate analysis due to low prevalence. Multivariate logistic regression was performed, and risk factors with a p-value less than 0.3 were included. It found that age is the only risk factor associated with drug-resistant loodstream infection, with odds ratio of 1.04 (95% CI: 1.0–1.08, p = 0.03).
Univariate analysis associated with bacteremia with drug-resistant organisms.
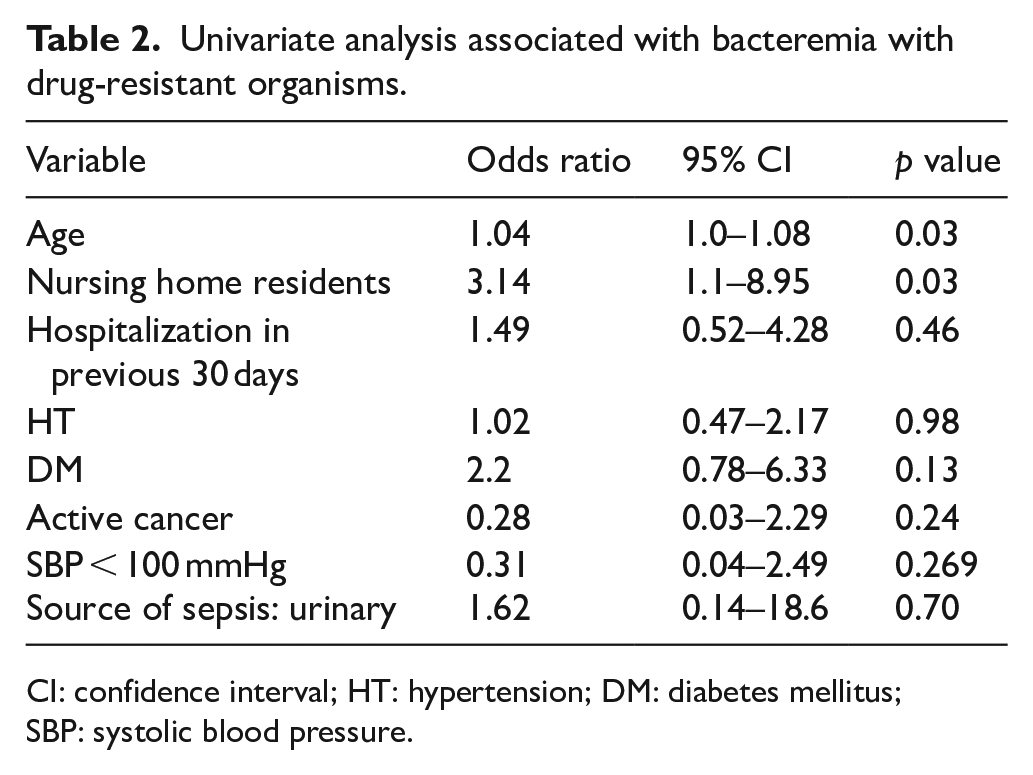
CI: confidence interval; HT: hypertension; DM: diabetes mellitus; SBP: systolic blood pressure.
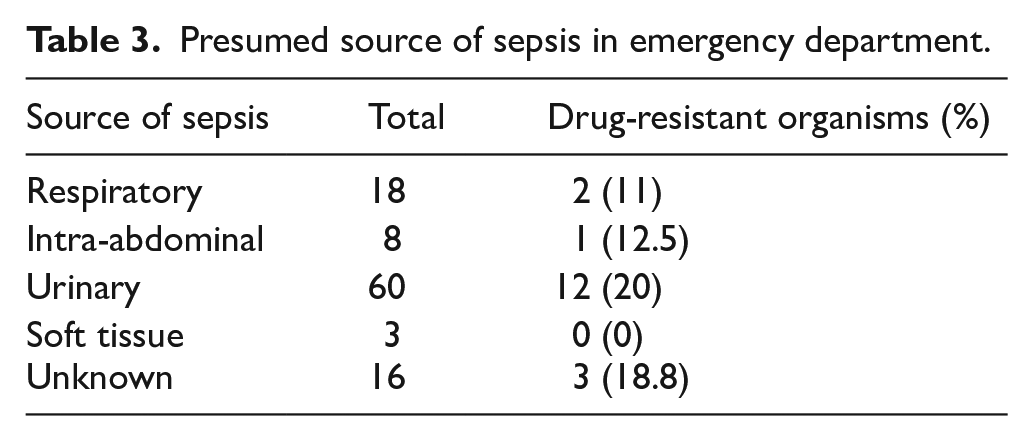
Urinary tract was the presumed source of infection in more than half of the cases, while in around 15% of the cases the source of infection was unknown at the emergency department (Table 3). Fisher’s exact test showed that the incidence of drug-resistant organism bloodstream infection is not different among different sources of infection (p = 0.93).
Presumed source of sepsis in emergency department.
Among the 105 patients, 100 of them received first dose of antibiotics in the emergency department. Among these patients, 81% of them received first-line antibiotics. Amoxicillin/clavulanate acid (augmentin) was the most commonly given first-line antibiotics (n = 70), while cefoperazone/sulbactam (sulperazon) was the most commonly used big gun antibiotic (n = 14). Among the patients who received first-line antibiotics, 17% of them turned out to have infection with drug-resistant organisms. Only 15% of patients who received big gun antibiotics had infection with drug-resistant organisms.
Among the microorganisms isolated in blood culture, the majority of them were gram-negative organisms: 47 of them were Escherichia coli and 22 of them were Klebsiella pneumoniae. There were 14 gram-positive organisms. More than half of the drug-resistant organisms were Escherichia coli (55%).
Discussion
In this study, age is found to be a risk factor for bloodstream infection caused by drug-resistant organisms. This finding is similar to the results from previous studies. However, this finding alone may not be enough to inform the choice of antibiotics in emergency department. In a study by Wright et al., 5 they found that age above 65 years was a risk factor for multidrug-resistant urinary tract infection in emergency department patients. Whether this cut-off can be applied to our patients is unknown, and factors including functional performance and presence of comorbidities may be more important than chronological age. Studies have found that clinical frailty score correlates with mortality in different disease conditions, and in some cases even better than chronological age.9 –12 Aging population is a global health issue, and healthcare professionals are more aware of the problem of frailty. Emergency physicians and nurses are more familiar with the concept and identification of frailty, and easily used assessment tools may be helpful in research and clinical settings. Further research can focus on the association between measures of frailty (e.g. Clinical Frailty Scale by Rockwood et al. 13 ) and infection with drug-resistant organisms.
Based on our previous clinical experience, it is expected that residence in nursing home and hospitalization in the previous 30 days are associated with drug-resistant organism bacteremia. This study failed to show a significant association. Previous Infectious Diseases Society of America (IDSA) guidelines for the management of hospital-acquired pneumonia in 2005 had included the term healthcare-associated pneumonia. 14 They suggested that residence in nursing home and previous hospitalization were risk factors for pneumonia with drug-resistant pathogens. The entity of healthcare-associated pneumonia was removed from the later versions of IDSA guidelines as subsequent studies showed that the risk factors encompassing healthcare-associated pneumonia failed to predict high prevalence of pneumonia with antibiotic-resistant organisms. 15 The findings in this study seem to suggest a similar phenomenon.
One possible explanation is the difference in carriage rate of multidrug-resistant bacteria in the community adults versus nursing home residents. Kwok et al. 16 found that more than 50% of healthy adults in Hong Kong community carried extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae, while the carriage rate of methicillin-resistant Staphylococcus aureus (MRSA) was 2.5%. It can be deduced that the chance of community-acquired bacteremia caused by drug-resistant organisms is high due to the high carriage rate of ESBL-producing Enterobacteriaceae. Another study on residents of elderly nursing homes found that around 30% of nursing home residents carried MRSA. 7 Our impression that nursing home residents have high carriage rate of drug-resistant organisms is correct, but the pattern of organism involved may be different from that in the community. Nursing home residents may have more other drug-resistant infections (e.g. pneumonia, soft tissue infection) rather than bacteremia, as bloodstream infections were mostly caused by gram-negative bacilli. Another problem is the likely confounding effect of age and residence in nursing home.
The study by Kwok et al. 16 also found that previous antibiotic use is associated with carriage of multidrug-resistant bacteria. The association of previous antibiotics use and the development of infection with multidrug-resistant pathogens are similarly found in other studies.3,5 While prescription of antibiotics from public hospitals is easily identified on electronic medical record, antibiotics prescribed by private doctors are difficult to trace and patients with sepsis may not be able to give a full medication history. Eliciting a full medication history is not possible due to the retrospective nature of this study, so previous antibiotic use was not included for analysis in this study.
This study has some limitations. Blood cultures were performed in patients who presented with suspected sepsis in the emergency department. The diagnosis of suspected sepsis was mainly based on initial clinical assessment by the treating physician, and the decision to perform blood culture was up to the physician. While a lot of patients with infection presented with typical signs and symptoms of systemic inflammatory response syndrome (SIRS), it is not specific or sensitive for infection. Clinical gestalt was found to be accurate in diagnosing respiratory infections, 17 but it may not be reliable in cases of occult sepsis. Frail elderly patients, patients with severe immunosuppression, and patients in the early stage of infection may not present with obvious signs and symptoms of sepsis, so they may be missed in the initial assessment in emergency department. As a result, the patients included in this cohort may not fully represent all patients with bloodstream infection in the emergency department.
The prevalence of chronic obstructive pulmonary disease and cirrhosis is surprisingly low in the study sample. It may be due to underreporting by physicians in the electronic medical records. This is a limitation because of the retrospective nature of the study.
Only 17% of the bacteremia cases were caused by drug-resistant organisms. This is in contrast to previous studies, in which multidrug-resistant gram-negative organisms accounted for up to 20%‒30% of the cases.3,18 It is also unexpected based on the high carriage rate of ESBL-producing Enterobacteriaceae in the community. 16 The exact reason of this is unknown, but it is unlikely to be of low disease severity, as the 30-day mortality rate was 15%, comparable to that reported in other populations.19 –21
In conclusion, age is a significant risk factor for drug-resistant organisms among patients with bloodstream infection in the emergency department. Further research may be needed to find out the relationship between frailty and infection with drug-resistant organisms. This study fails to identify other risk factors to inform antibiotics prescription in the emergency department. The surge in drug-resistant microorganism drives clinicians to prescribe broad-spectrum antibiotics, creating a vicious cycle of drug resistance. More study is needed to guide clinicians and to break the vicious cycle.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.