
Abstract
Introduction:
In Hong Kong, heat-related illness (HRI) represents an important cause of morbidity and mortality among healthy adults engaging in outdoor activities during summer. It can result in intensive care unit (ICU) admission. This retrospective study aimed to profile critically ill patients with HRI and identify potential risk factors for mortality.
Methods:
This retrospective case series included adults with HRI from 1 January 2009 to 30 June 2020 admitted to the ICU of Pamela Youde Nethersole Eastern Hospital (PYNEH). Demographics, admission severity, co-morbidities, and laboratory investigations were analysed. Outcome data studied included mortality, ICU length of stay (LOS), ventilator days, and hospital LOS.
Results:
Among the 38 individuals included, 97% were hikers. About 92.1% of patients survived, while 7.9% expired. The median age of the patients was 48 years, and 78.9% were men. Hypertension was the most frequent concurrent disorder. Most cases were presented during the hot summer months of May (29%), July (24%) and August (18%). The localities’ median peak temperature and humidity were 33.2°C and 88%, respectively. Ninety-two percent of patients were airlifted to the hospital by helicopters. The median peak body temperature was 40.3°C. Central nervous system derangement (Glasgow Coma Scale (GCS) score ⩽ 8) was the top presenting feature (65.7%). About 57.9% of patients required vasopressor support, followed by mechanical ventilation (50%) and renal replacement therapy (31.6%).
Conclusions:
Most critically ill patients suffering from HRI were hikers and middle-aged adults. Mortality was 7.9% despite advanced life support in ICU. Raising public awareness of the associated risk with hiking in hot summer is essential for the prevention of HRI.
Introduction
Hong Kong is a sub-tropical country with a hot and humid climate between May and August. Afternoon temperatures often exceed 31°C with high humidity, which increases the risk of heat-related illness (HRI). 1 Due to global warming, HRI is getting more common in Hong Kong. According to the report of Hong Kong Observatory, the average number of people suffering from heat stroke was 75 per year from 2005 to 2013. HRI represents a continuum of disorders ranging from heat cramps and heat exhaustion to life-threatening heat stroke. 2 As dictated by situations, helicopters are often the emergency medical transportation of choice if there is no immediate access to hospitals like in the mountain areas. A previous study revealed that 24.4% of airlifted patients from the emergency scene suffered from HRI. 3 Exertional heat stroke represents the most severe entity among heat disorders.4 –6 Mortality of heat stroke ranged between 10% and 50% in the previous study. 7 While potentially fatal, it is preventable and salvageable. Patients suffering from the severe extreme of HRI often require advanced life supports in intensive care unit (ICU). However, local data on their clinical outcome was scarce. This study evaluated the clinical characteristics and outcomes of patients with HRI who required intensive care.
Methods
This retrospective study was conducted in Pamela Youde Nethersole Eastern Hospital (PYNEH), a tertiary care centre that received the majority of airlifted patients transferred by the Government Flying Service (GFS) in Hong Kong. Eligible patients were searched and retrieved from the Clinical Data Analysis and Reporting System of Hospital Authority with a diagnosis of heat stroke and heat exhaustion. Patients more than 18 years old with a primary diagnosis of HRI, both heat stroke and heat exhaustion, with admission to the ICU between 1 January 2009 and 30 June 2020 were recruited. Patients with the incomplete clinical record were excluded. Patients were followed till acute hospital discharge or death, whichever occurred earlier.
HRI represents a continuum of disorders ranging from heat cramps and heat exhaustion to life-threatening heat stroke. 8 Following Bouchama’s severity classification based on the core body temperature and central nervous system abnormalities, we categorised the participants into heat stroke (peak core body temperature ⩾40.0°C with Glasgow Coma Scale (GCS) score ⩽ 8), or heat exhaustion (peak core body temperature > 37°C but < 40°C). 9
Data including demographics, diagnosis, clinical characteristics, laboratory parameters and clinical outcomes were collected. All the data were extracted from the Clinical Management System (CMS) and ICU Clinical Information System (CIS), both were clinical data storage systems used by the Hospital Authority. The first value of vital and laboratory parameters during accident and emergency department (AED) admission and ICU admission were recorded. Except for peak core temperature, the highest documented temperatures on AED cards, including the one charted by GFS, were recorded.
The peak and trough ambient temperatures were obtained through a historical search from the Hong Kong Observatory’s daily extract of meteorological observations. 2
This study was approved by the Hong Kong East Cluster Clinical Research Ethics Committee (Anonymized). The requirement for patient consent was waived for this retrospective study.
Statistical analysis
Results were expressed as median ± interquartile range (IQR) or a number of cases and percentages, as appropriate. Categorical variables were compared by Fisher’s exact test and chi-square test, whereas Mann–Whitney U test was used to compare continuous variables between survivors and non-survivors. All tests were two-sided and assessed at the 0.05 significant level. All data analyses were performed using Statistical Package for Social Sciences for Window, version 25 (SPSS, Chicago, IL, USA).
Results
Thirty-eight patients with HRI were admitted to the ICU during the study period. All were presented between May and October. Of which, most had occurred during the hot summer months of May (29%), July (24%), and August (18%). The median peak environmental temperature and humidity on the particular days of the HRI were 33.2°C (IQR: 32.2–33.6) and 88% (IQR: 85–90), respectively.
Table 1 shows the characteristics of patients with HRI. The median patient age was 48 years (IQR: 30–55). Males represented 78.9% of the patients. All patients were outdoors when they contracted the HRI, of which 37 patients were hiking, and one patient was working at a construction site. Thirty-five patients (92.1%) were airlifted to hospitals using the GFS helicopters. Ten patients (26.3%) had at least one co-existing illness, of which hypertension (15.8%) was the most common.
Characteristics of the 38 critically ill patients with HRI.
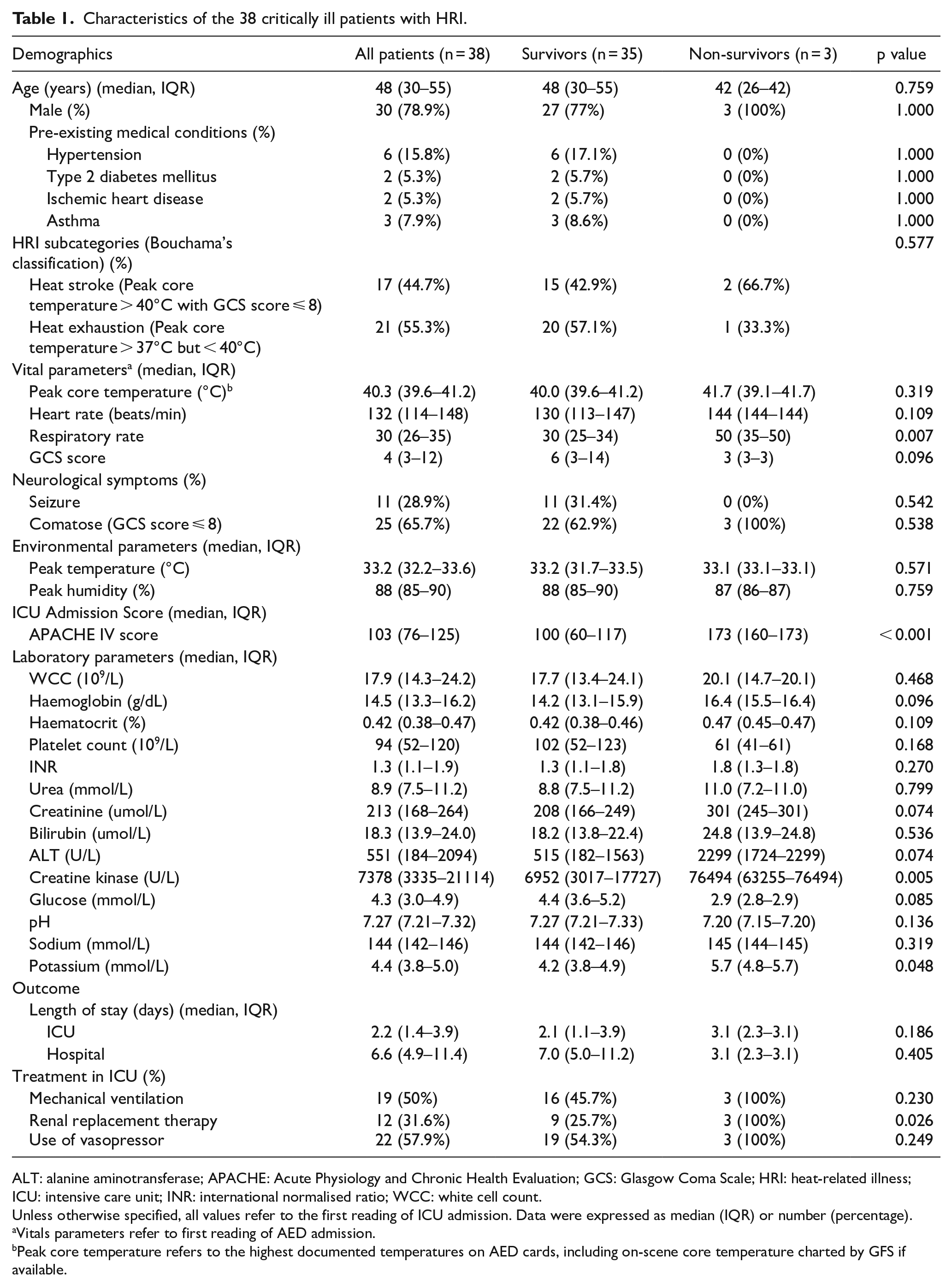
ALT: alanine aminotransferase; APACHE: Acute Physiology and Chronic Health Evaluation; GCS: Glasgow Coma Scale; HRI: heat-related illness; ICU: intensive care unit; INR: international normalised ratio; WCC: white cell count.
Unless otherwise specified, all values refer to the first reading of ICU admission. Data were expressed as median (IQR) or number (percentage).
Vitals parameters refer to first reading of AED admission.
Peak core temperature refers to the highest documented temperatures on AED cards, including on-scene core temperature charted by GFS if available.
Patients admitted to ICU with HRI had a median admission Acute Physiology and Chronic Health Evaluation (APACHE) IV score of 103 (IQR: 76–125). Consistent with our inclusion criteria, the median peak core body temperature was 40.3°C (IQR: 39.6–41.2). Seizure was present in 28.9% of patients. In all, 25 (65.7%) patients had their Glasgow Coma Scale (GCS) score 8 or less, with a median GCS score of 4 (IQR: 3–12). All non-survivors presented to the hospital with a GCS score of 3. Regarding the temperature lowering techniques, cold intravenous fluids were initiated in all patients in AED. In contrast, the use of external cooling with ice packs, fanning, and cooling blankets was documented in 52.6% and 78.9% of patients in AED and ICU, respectively.
Creatine kinase (CK) was increased in all patients with a median of 7378 U/L (IQR: 3335–21,114). The second commonest biochemistry abnormality was increased serum creatinine concentration (97%) with the median value of 213 umol/L (IQR: 168–264), while 12 (31.6%) of these patients progressed to renal failure and haemolysis commenced.
Liver enzymes were raised in 36 (94.7%) patients with the median alanine aminotransferase (ALT) 551 U/L (IQR: 184–2094) and deranged clotting profile with international normalised ratio (INR) 1.3 (IQR: 1.1–1.9). None of the patients demonstrated a bleeding tendency. N-acetylcysteine (NAC) infusion was initiated in 4 (10.5%) patients. Thrombocytopenia was observed in 20 (52.6%) patients with a median platelet count of 94 × 109/L (IQR: 52–120). Thirteen (34.2%) patients experienced hypoglycaemia with a median glucose level of 4.3 mmol/L (IQR: 3.0–4.9) on admission.
There were 19 (50%) patients requiring mechanical ventilation as respiratory support, while 22 (57.9%) patients remained in shock despite fluid resuscitation and were started on vasopressors as haemodynamic support. Renal replacement therapy was initiated in 12 (31.6%) patients.
The overall mortality rate was 7.9% (3 of 38), and none died within 24 h of admission. Median ICU length of stay and hospital length of stay were 2.2 days (IQR: 1.4–3.9) and 6.6 days (IQR: 4.9–11.4), respectively. All the survivors were discharged with a normal GCS score, of whom one suffered from severe ataxia.
When compared with survivors, non-survivors had a significantly higher APACHE IV score (median APACHE IV 173 vs 100, p > 0.001), higher admission respiratory rate (median respiratory rate 50 vs 30, p = 0.007), higher admission creatine kinase level (median creatine kinase level 76494 U/L vs 6952U/L, p = 0.005), and requirement of renal replacement therapy (100% vs 25.7%, p = 0.026).
Discussion
The present retrospective study evaluated the outcomes of patients with HRI requiring ICU care. The findings of our current study supplement the understanding of HRI based on data in an ICU in Hong Kong.
We found lower mortality (7.9%) of HRI in our study compared with that of 14.5% observed by Liu et al. 7 In the paper from China, the documented admission median peak body temperature was 42°C, which was 1.7°C higher than our patients. Another possibility might be related to the severity of the patients; only the more severe cases were admitted to their tertiary hospitals, while milder cases were triaged to secondary medical centres. Therefore, the higher severity of patients might account for the higher mortality in their study. Moreover, in the China series, 50% of the patients were admitted to the hospital beyond 4 h of the onset of HRI. The delayed presentation could be explained by the prolonged transportation time to medical centres using ground transportations compared with Hong Kong, which is equipped with aeromedical services. And the delayed presentation might lead to delayed treatment and thus increase mortality.
A more significant proportion of patients (57.8%) were in shock in this case series. In contrast, only 28.6% were in shock observed by Sithinamsuwan et al. 10 In our study, the vasopressors use was up to 57.9%. One possible explanation could be a different triage criterion among the two ICUs, with some milder HRI cases without shock admitted to the emergency medical ward instead of ICU due to limited ICU bed availability in Hong Kong. Another possibility might be related to the demographics of the patients. The median age of our HRI patients was 48. The patients enrolled in the Thailand case series were from Phramongkutklao Army Hospital, a military medical centre. The median age in their study was only 21, with 89.3% of the patients being soldiers who might have better cardiopulmonary reserve with better compensation facing HRI.
Among our patients, only 23 of 38 (60.5%) patients had a recorded peak core temperature > 40°C to fulfil Bouchama’s diagnostic criteria of heat stroke. However, neurological manifestations were detected in 92% of our patients; 11 of them presented with seizures, while 25 were comatose (GCS score < 8) and 10 were confused (GCS score 9–14). Among the spectrum of HRI, only heat stroke is characterised by neurological dysfunction. Most of the diagnostic criteria in published literature adopted elevation of core temperature > 40°C as a necessary condition for the diagnosis of heat stroke. In clinical practice, the peak core temperature is often not measured at disease onset or not detected due to the cooling treatment prescribed. Therefore, the absence of an admission body temperature > 40°C does not negate a positive diagnosis of heat stroke. Appropriate cooling interventions should not be delayed in establishing heat stroke diagnosis. Alternatively, though not widely adopted, the Japanese Association for Acute Medicine (JAAM) criteria for heat stroke can be considered as a core temperature > 40°C is not required to be diagnostic. 11
CK has been demonstrated as a valuable marker to differentiate between survival and death with an area under the curve (AUC) of ROC plot > 0.9 in a study by Alzeer et al. 12 on serum enzymes in patients with heat stroke. Our univariate analysis suggested that an increase in CK level was also shown to be a statistically significant risk factor for mortality, with the average level up to around 76,000 U/L. As observed by Veenstra et al., 13 rhabdomyolysis with a high CK exceeding 15,000 U/L could result in a higher chance of acute kidney failure. In our study, the requirement of renal replacement therapy for renal failure is another statistically significant risk factor for mortality in univariate analysis. Due to the small sample size in this study, it is difficult to recommend an optimal cutoff for CK to differentiate between survivors and non-survivors.
Acute liver derangement is one of the known complications of heat stroke. Microthrombosis related to thrombosis and vascular endothelium injury has been proposed as the aetiology.14,15 Hepatocellular injury in heat stroke could be delayed by up to 24 h and, in severe cases, would require a liver transplant. 16 Our data showed a trend towards that compared with survivors, non-survivors liver enzymes ALT (2299 U/L vs 551 U/L; p 0.074) and INR (1.8 vs 1.3; p 0.27) were higher, and the glucose level (2.9 mmol/L vs 4.4 mmol/L; p 0.085) was lower, although we failed to demonstrate a statistically significant result. NAC has been used in non-acetaminophen-induced acute liver failure, with the proposed mechanism being its antioxidant and vasodilating effects. 17 A few case reports described the use of NAC as an early potential therapeutic option for heat stroke-induced liver injury.18 –20 In our study, four patients were given NAC, and all survived. Further studies are warranted to assess the efficacy of NAC in patients with HRI-related liver injury.
Of note, both aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are present in skeletal muscle, and they are frequently elevated in patients with severe rhabdomyolysis.21,22 Both aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are present in skeletal muscles. To determine the source of the elevated aminotransaminases in rhabdomyolysis, we can use other liver markers. γ-glutamyl transferase (GGT) is not found in muscle and would suggest liver injury if elevated. Likewise, elevation in bilirubin would not be expected in isolated muscle injury.
In our study, one of the survived patients suffered from bowel ischaemia as a complication of HRI. He presented with a seizure on admission and was thus intubated and sedated. He was noted to have persistent shock, progressive abdominal distension and high output from the nasogastric tube during his ICU stay. Computed tomography (CT) revealed bowel ischaemia. Laparotomy showed ischaemia over the caecum and ascending colon. Right hemicolectomy was performed. Pathology of the resected bowel suggested mucosal necrosis. Bowel ischaemia is a rare complication of HRI. 23 Under HRI, blood flow to the skin is increased to facilitate heat dissipation at the expense of splanchnic and renal blood flow.24,25 Blood flow to the intestines can be significantly reduced up to 80% during exercise and is further compromised in HRI. 26 The reduction of intestinal blood flow would lead to disruption of the intestinal barrier and production of endotoxin. 27 In patients with HRI, one should consider the possibility of bowel ischaemia in patients with unexplained shock and signs of acute abdomen. Early investigations are required to reveal the presence of bowel ischaemia.
There are limitations of our retrospective study. The small number of patients and low mortality rate limited statistical analysis with multivariable logistic regression. These limitations could be overcome with a multi-centre study using a large sample size with prior sample size calculation. Besides, patients with severe HRI who passed away before ICU admission were not included in this study. We likely underestimated the actual HRI mortality.
Moreover, most of our studied patients came from wilderness environments. Although PYNEH received the majority of the patients transferred by GFS, some of the patients might be airlifted to other hospitals depending on locality and severity. So, it only represented a subset of patients with HRI who required intensive care in Hong Kong. The generalisability of our findings to Hong Kong can be improved. Further study with inclusion of HRI patients who were non-airlifted and out of wilderness setting (e.g. occupational, recreational, and classical heat stroke) could be considered.
Besides, 92.1% of our studied patients were airlifted to the hospital by GFS. Pre-hospital management including pre-hospital cooling by paramedics, plays a vital role in early management of HRI, but they are often not well documented in the emergency department or ICU medical records. As pre-hospital factors may also affect the outcome, pre-hospital data from GFS could be retrieved for further analysis.
Furthermore, the peak daily temperature and humidity may not accurately reflect actual heat stress on our patients. The Hong Kong Heat Index (HKHI) developed by the Hong Kong Observatory may be a better alternative in reflecting the heat stress impact on the excess hospitalisation ratio. 28 However, historical data of the HKHI was not available for analysis. The general public can refer to the Hong Kong Observatory website for daily updates on HKHI. It should take appropriate precautions when HKHI reaches around 30 or above to prevent adverse health effects from hot weather. 28
With higher maximum temperatures and the popularity of outdoor activities, exposure to extreme heat and humid environments is a growing concern. Public education and health programmes to prevent HRI are therefore needed.
Conclusion
Most critically ill patients suffering from HRI were hikers and middle-aged adults. Mortality was 7.9% despite ICU advanced life support. Raising public awareness of the associated risk with hiking in hot summer is essential for the prevention of HRI.
Footnotes
Author contributions
Concept or design: CCY Chan. Acquisition of data: HP Shum, LL Chang. Analysis or interpretation of data: CCY Chan, HP Shum, P Wu. Drafting of the manuscript: CCY Chan, P Wu, NYW Leung, WW Yan. Critical revision of the manuscript for important intellectual content: All authors. All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Hong Kong East Cluster Clinical Research Ethics Committee (HKECREC-2021-058). The requirement for patient consent was waived for this retrospective study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.