
Abstract
Introduction:
Tetrodotoxin poisoning is typically caused by puffer fish consumption. This study is to review its demographics, clinical presentations and management in Hong Kong.
Method:
Reported cases of tetrodotoxin poisoning to Hong Kong Poison Information Centre from October 2008 to March 2021 were included in the study. Information from electronic database was analysed.
Results:
Forty-two cases were included in this case series. The number of incidents of tetrodotoxin poisoning ranged from 0 to 5 per year, mostly in the winter months. Median ingestion-to-symptom and ingestion-to-door time was 2 and 6.5 h, respectively. 48% of puffer fish meal sharer was symptomatic and attended emergency department. 100% and 48% of all cases had neurological and cardiovascular/gastrointestinal symptoms, respectively. Fukuda and Tani clinical Grade 1 and 2 were the most common presentation. 17% required intensive care while most patients were managed safely in emergency department and/or emergency medicine ward.
Conclusion:
There are recurrent incidents of tetrodotoxin poisoning in Hong Kong. Public education is the key to prevent future outbreaks. Targeted history and enhanced availability of tetrodotoxin test would assist in its diagnoses.
Introduction
Puffer fish has been described for long in human history. It was illustrated on an Egyptian tomb of the fifth dynasty dated 2500 BC. 1 From time to time, there are food poisoning cases associated with puffer fish consumption. Tetrodotoxin, produced predominantly by marine Vibrio bacteria that live symbiotically with puffer fish, is implicated for the toxic effect. Despite its isolation for over a century, there remained no specific treatment for tetrodotoxin poisoning. In Hong Kong, selling of any food unfit for human consumption commits an offence and can be prosecuted in cases of puffer fish food poisoning. In this review, the demographics, clinical features and management of patients of tetrodotoxin poisoning reporting to Hong Kong Poison Information Centre will be illustrated.
Methodology and study design
Reported cases of tetrodotoxin poisoning to Hong Kong Poison Information Centre (HKPIC) from October 2008 to March 2021 were included in the study. The cases were retrieved from HKPIC electronic database ‘DATOX’, with the poison coding of ‘Non-pharmaceutical/Toxin in food/Tetrodotoxin’ or poison name of ‘puffer fish’ and ‘tetrodotoxin’. Information on patient demographic data, clinical data and treatment received was collected. Cases would be excluded if the poisoning outcome was judged to be unrelated to tetrodotoxin poisoning. Cases not due to food poisoning and cases with multiple toxin poisoning that complicate the clinical picture would also be excluded. This study was approved by Research Ethics Committee (Kowloon Central/Kowloon East) (KC/KE-21-0182/ER-4).
Results
There were 48 cases found. Four cases were excluded as the poisoning outcome was unrelated to tetrodotoxin poisoning. One case was excluded as tetrodotoxin from laboratory reagent rather than food was ingested. One case was excluded as both ciguatoxin and tetrodotoxin were suspected to account for patient’s symptom. Forty-two cases were included in this case series.
The median age of patients was 55 (range = 18–72) years. Twenty-four patients (57%) were male. Table 1 showed the demographics of our patients who suffered from tetrodotoxin poisoning. Most exposures occurred in residence and resulted from consumption of wild-caught puffer fish in Hong Kong. Both fresh or dried, cooked or uncooked puffer fishes resulted in toxicity. Half of the patients had symptom onset within 2 h from ingestion of puffer fish. It took another median of 4.5 h for half of the patients to attend Accident and Emergency Department (AED). Ambulance was the mean of transportation in 40% of patients in this case series.
Patient demographics.
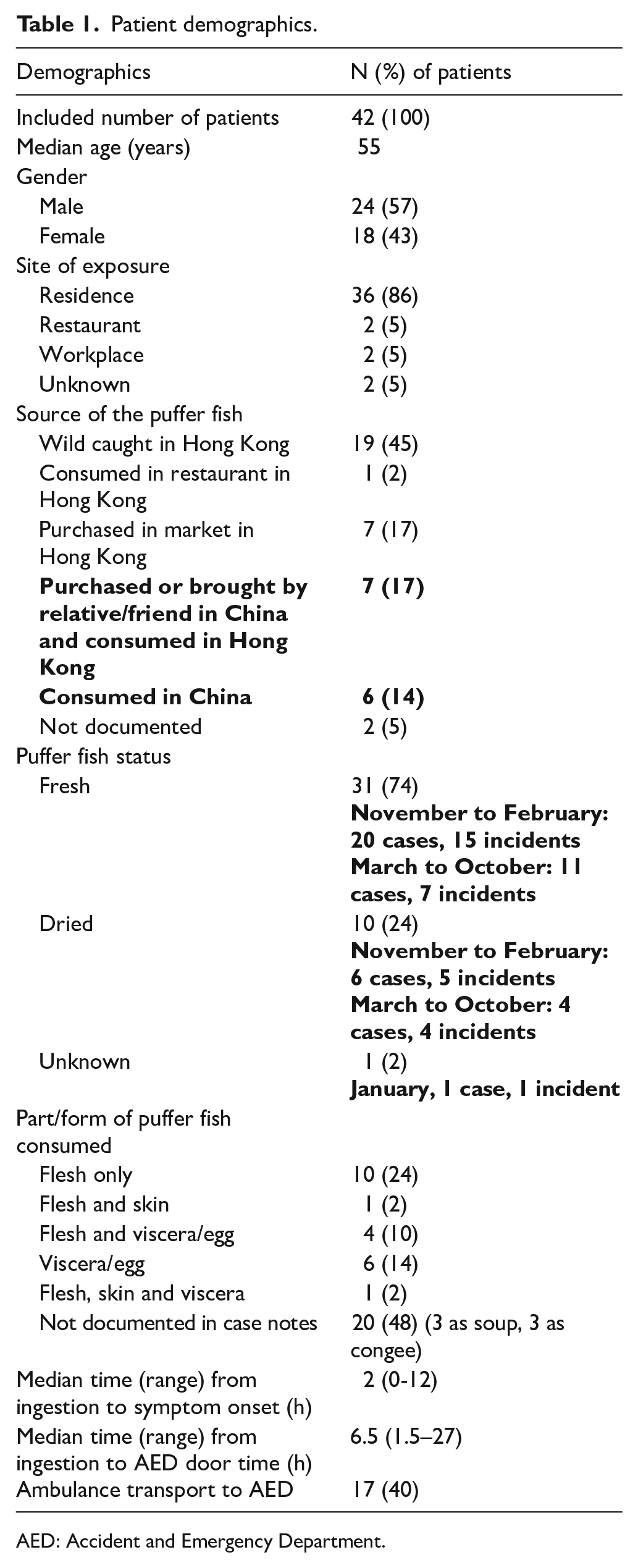
AED: Accident and Emergency Department.
From October 2008 to March 2021, the number of incidents of tetrodotoxin poisoning ranged from 0 to 5 per year. Overall, 48% of meal sharers in these incidents experienced symptoms and attended AED. Table 2 illustrated the annual number of incidents, the number of meal sharers involved, and the number of symptomatic cases attending AED.
Annual number of incidents of tetrodotoxin poisoning, the number of meal sharer, and the number of symptomatic cases attending AED.
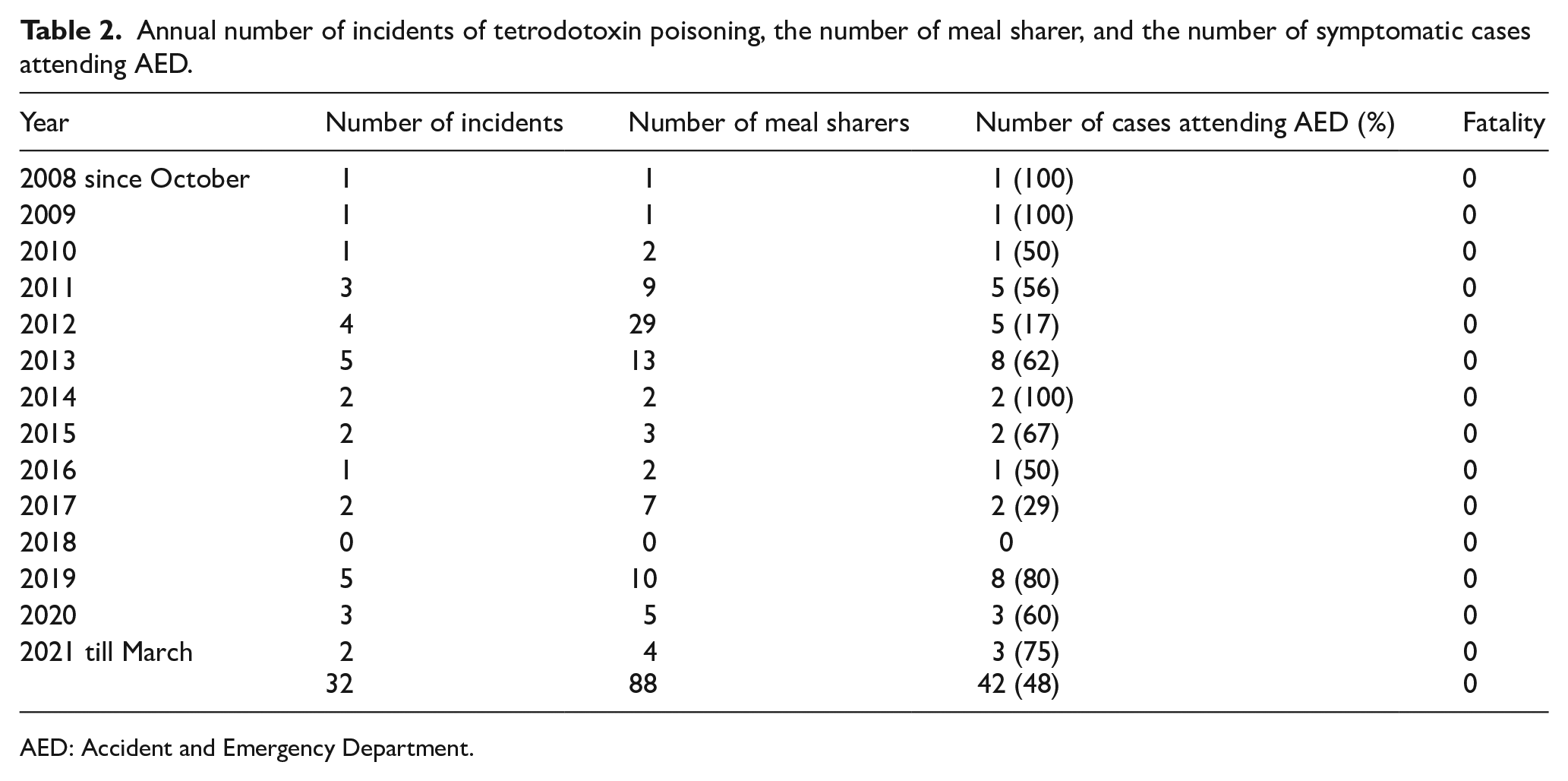
AED: Accident and Emergency Department.
Most incidents happened from November to February in the year. Chart 1 showed the cumulative monthly number of incidents and cases involved.
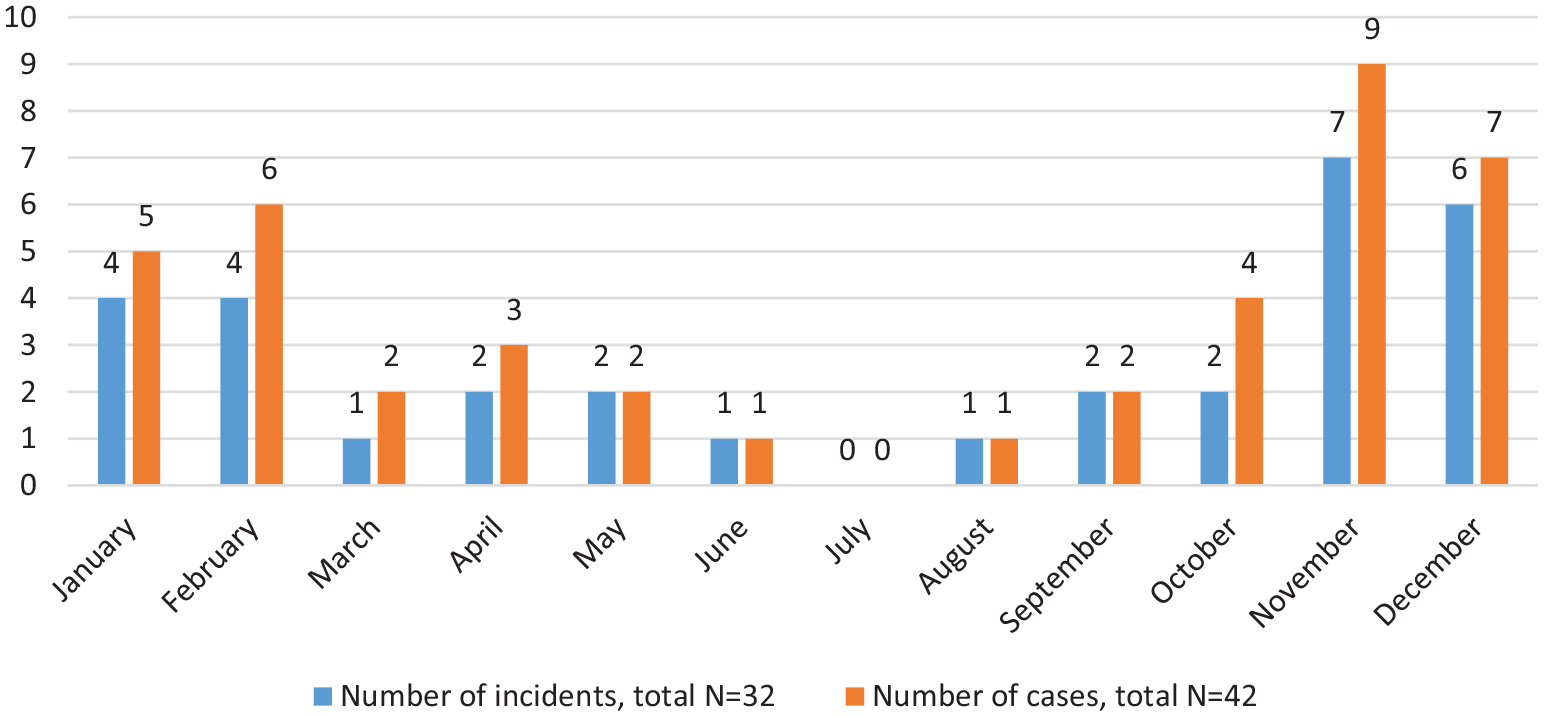
Cumulative monthly number of tetrodotoxin poisoning in Hong Kong.
The Fukuda and Tani clinical grading classified the patients into four severity categories according to their neurological, gastrointestinal, cardiovascular and respiratory symptoms and signs 2 (Table 3). Grade 1 patients experience perioral numbness with or without gastrointestinal symptoms, while Grade 4 patients suffered severe cardiovascular and respiratory failure. 57% in our series belonged to Grade 2, followed by 33% of Grade 1.
Clinical urgency, features, and severity grading.
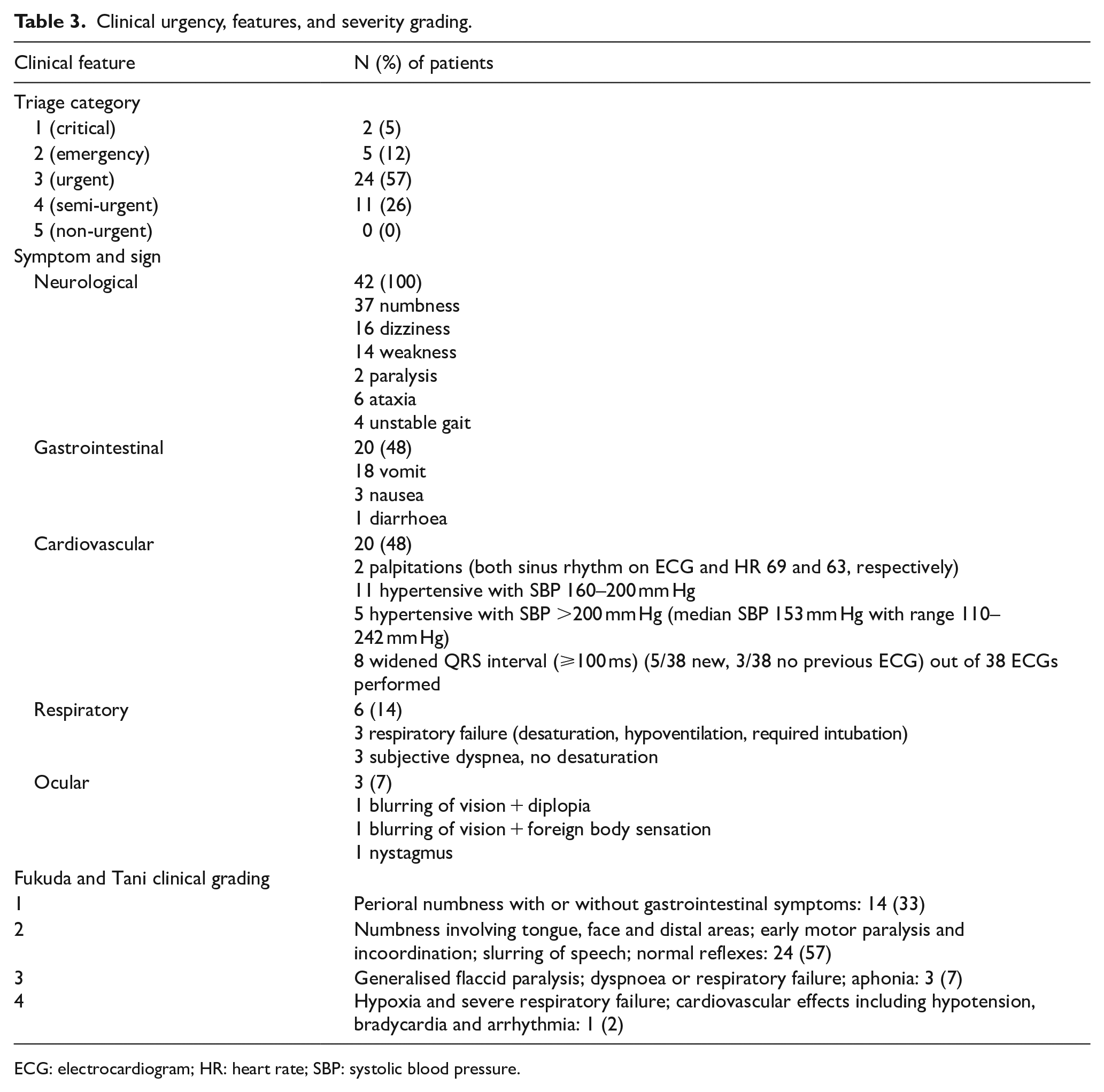
ECG: electrocardiogram; HR: heart rate; SBP: systolic blood pressure.
Three patients had major effect in their clinical outcome, requiring endotracheal intubation. All of them (100%) consumed egg or viscera of fresh or dried puffer fishes. Four of nine patients with moderate effect in clinical outcome had known parts of puffer fish consumption. Three of these four patients (75%) had egg or liver consumed. In contrast, only 5 of 20 patients (25%) with minor outcome had documented skin, egg or liver consumed. The remaining 10 patients with minor outcome did not have documentation on which part of puffer fish consumed.
Most of the patients were triaged in emergency department as Category 3 (urgent) and Category 4 (semi-urgent) (Table 3). All of them presented with various types and degree of neurological symptoms. Cardiovascular and gastrointestinal symptoms were also common (48%). Thirty-eight cases had electrocardiogram (ECG) performed, with median heart rate 74/min (range = 53–100/min), median QTc interval 433 ms (range = 362–483 ms) and median QRS duration 92 ms (range = 50–126 ms). Eight cases had widened QRS ⩾100 ms. For those with previous ECGs available for comparison, the QRS widening was new onset in five cases, including two of three cases with major outcome.
Eight (19%) patients were directly discharged from emergency department, 19 (45%) patients were managed in Emergency Medicine ward, 8 (19%) were managed in general medical ward and 7 (17%) required intensive care. As expected, the length of stay is the shortest in patients directly discharged from AED and the longest in patients requiring intensive care. The median length of stay in these four groups was 9, 24, 32 h and 3 days, respectively. The Fukuda and Tani clinical grading correlated well with the disposal. There were no Grade 3 or 4 patients discharged from AED, admitted to Emergency Medicine ward or general medical ward, and no Grade 1 patient was admitted to intensive care unit.
There is currently no specific antidote for tetrodotoxin poisoning. The mainstay of treatment given was supportive. None of the cases underwent gastric lavage and three cases were given activated charcoal. There were seven cases admitted to intensive care unit, and three of them required respiratory support with endotracheal intubation.
Discussion
In Hong Kong, the prevention and control measures of tetrodotoxin poisoning are carried out by different government departments. This included food surveillance by the Centre for Food Safety; food analysis by Government Laboratory; food poisoning investigation by Centre for Health Protection; food regulations (Public Health and Municipal Services Ordinance) enforced by Food and Environmental Hygiene Department. With the continuous effort of various parties in prevention, outbreak control and investigation, there was no documented fatality due to puffer fish consumption in Hong Kong since year 1994. 3 However, from our case series, since most victims had their puffer fishes caught wildly or bought from China, tetrodotoxin poisoning was still recurrently reported. Therefore, public education is the most important part of tetrodotoxin poisoning prevention.
Clinical availability of tetrodotoxin test
Some cases may have the ‘puffer fish’ tissue sample or cooked food remnant sent by the Food and Environmental Hygiene Department to Government Laboratory for analysis. However, their results were not accessible by emergency physicians. In our series, tetrodotoxin testing was not often done. Only seven (17%) had food or urine/blood samples sent for analysis in Hospital Authority laboratories. Although two cases in 2019 had food remnant and vomitus sent for analyses, these were finally cancelled due to unavailability of the test. Tetrodotoxin test for human was only available in certain tertiary hospitals in Hong Kong before 2021. Since the first quarter of year 2021, the Toxicology Reference Laboratory provided tetrodotoxin test for all public hospitals in Hong Kong. Hopefully, with the increased availability of the tetrodotoxin test, more cases can be supported by laboratory confirmation. Nonetheless, like any other laboratory test, the turnover time would limit the clinical usefulness of the test. It would be prudent to take a comprehensive history, detailed physical examination and manage our patients in emergency department according to the presenting toxidrome, with laboratory test as adjunct to confirm our diagnoses retrospectively.
Neurological symptom
All the patients in our series presented with various types and severity of neurological symptoms. The symptoms range from simple lip numbness to respiratory failure requiring intubation and intensive care. There is no simple rule to predict which patient would have lip numbness only and which patient would deteriorate into respiratory failure. Although there is no specific antidote for tetrodotoxin, patients are advised to seek medical help once they experience symptom. If compared with stroke, which is the emergency condition with most acute alarming neurological symptoms, the median symptom-onset-to-door-time of stroke in a tertiary hospital and puffer fish poisoning in Hong Kong are 95 min and 6.5 h, respectively. 4 There is still room of improvement to advance the door time in puffer fish poisoning. An important difference between stroke and puffer fish poisoning is that the onset of stroke is unpredictable while the onset of puffer fish poisoning is preceded by oral ingestion of puffer fish with median of 2 h before. The reason why some patients delayed or even did not (52%) present to the emergency department has to be explored. It could be due to lack of awareness between puffer fish ingestion and the neurological symptom. Another explanation would be due to less severe symptom in puffer fish food poisoning, that most cases attending emergency department had Fukuda and Tani clinical grading 1 to 2. This implicates the need for reinforcement of public education on early warning symptoms and signs of puffer fish food poisoning. It is important to prevent deterioration without appropriate medical care in the out-of-hospital setting.
Gastrointestinal symptom
Gastrointestinal symptoms were the next most common symptom reported in this case series after neurological symptom. The diagnosis of tetrodotoxin poisoning may be difficult if the history of puffer fish consumption, the timing of ingestion, and the number of involved individuals were not specifically asked for. Presentation of nausea, vomiting, diarrhoea and non-specific numbness in an otherwise healthy individual may result in common diagnosis of gastroenteritis only. Therefore, under-diagnosis is possible in our series.
Cardiovascular symptom
Cardiovascular symptoms were also common in our series. Two patients had palpitation despite normal ECGs. Five and eleven patients had systolic blood pressure more than 200 and 160 mm Hg, respectively. The hypertension was transient during admission that only one patient was discharged with newly added oral amlodipine as anti-hypertensive medication. However, this patient claimed to have normal home blood pressure monitoring and defaulted follow-up after a few months. As a sodium channel blocker, widening of QRS complex (>100 ms) was newly found in eight patients (19%). No arrhythmia was detected. Concentration-dependent prolongation of PR and QRS intervals was observed in animals exposed to different tetrodotoxin concentrations. 5
Tetrodotoxin stability
Tetrodotoxin is water-soluble and heat-stable, so boiling of puffer fish and serving as soup or congee in our patients cannot destroy the toxin. However, salting and successive traditional fermentation over a few years was reported to reduce tetrodotoxin in puffer ovary to edible level. 6 Another study suggested that by knowing the various life cycle stages and tissue parts of tank-cultivated bullseye puffer (Sphoeroides annulatus), food safety was not a concern. 7 However, it would be dangerous for unqualified public who caught the puffer fish by themselves to decide on the potential toxicity.
Saxitoxin and accumulation of tetrodotoxin along the food chain
Puffer fish of the family Tetraodontidae was found to possess both tetrodotoxin and saxitoxins. In a study, saxitoxins accounted for 25% and 13% of total toxin amount in male and female fishes, respectively. 8 Although both tetrodotoxin and saxitoxins are sodium channel blocker, one puffer fish harbouring multiple toxins certainly complicate the clinical presentation. A study showed that combination of tetrodotoxin with saxitoxin increased the lethality of tetrodotoxin, even in the safe tetrodotoxin dose proposed by the European Food Safety Authority. 9 With rising water temperatures around the world, tetrodotoxin has been identified in a variety of marine organism worldwide, including trumpet shell marine snails, 10 Pacific oysters, 11 French bivalves and gastropods, 12 and New Zealand shellfish. 13 Both tetrodotoxin and saxitoxin can accumulate in fishes through the food chain. With the habit of enjoying culinary delicacy from all over the world, Hong Kong citizen are at high risk of exposure to tetrodotoxin from multiple marine food sources, not only from puffer fish. 14
Limitation
There are some limitations in our series. First, only food poisoning cases presumably related to tetrodotoxin were included. Other sources of exposure including one case ingesting laboratory grade tetrodotoxin for self-harm were not included. Second, under-reporting is likely as described in our discussion. Third, not all puffer fishes are poisonous, nor all tetrodotoxin poisoning cases were related to puffer fish consumption. Viral or bacterial food poisoning after puffer fish consumption is still possible in our case series and could affect our data integrity. Fourth, saxitoxin could have accounted for symptoms in some of our cases theoretically. Finally, missing data on case notes limited the reliability of our conclusions. These are important limitations to be borne in mind when interpreting results of our study.
Conclusion
We reported a series of 42 cases of tetrodotoxin poisoning in Hong Kong. Most incidents happened from November to February in the year. About half of the puffer fish meal sharer attend AED with symptoms. All and about half of the attending cases presented with neurological and cardiovascular/gastrointestinal symptoms, respectively. Most of them can be managed safely in AED and Emergency Medicine ward with shorter length of stay. Targeted history and enhanced availability of tetrodotoxin test would assist in diagnoses of tetrodotoxin poisoning.
Footnotes
Acknowledgements
The authors thank Mr M. H. Wong and the Hong Kong Poison Information Centre for facilitating database access.
Availability of data and materials
Data were collected through the Hong Kong Poison Information Centre (HKPIC) Poisoning Information and Clinical Management System (PICMS) retrospectively. Consultations and reports between the period of October 2008 to March 2021 were included for the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
The study was approved by the Kowloon Central/Kowloon East Research Ethics Committee (REC reference no. KC/KE-21-0182/ER-4).
Informed consent
Written informed consent was not necessary because no patient data have been included in the manuscript.