
Abstract
Introduction:
Procedural sedation and analgesia in children refer to the use of pharmacological measures to facilitate the management of painful procedures or emergency imaging, usually in emergency setting by non-anaesthetists. Emergency clinicians, nurses, patients and caregivers all have their roles to play in providing a safe sedation practice in the busy emergency department.
Method:
We did a retrospective review of all procedural sedation and analgesia done in patients below the age of 12 in our urgent care centre from October 2018 to August 2019.
Results:
There were 144 patients being identified in our review. Majority of them received intramuscular ketamine ranging from 2 to 4 mg/kg. There was no documented severe adverse effect in our review.
Conclusion:
Paediatric procedural sedation and analgesia is generally safe, efficient, adequate and facilitate early patient discharge.
Introduction
It is not uncommon for emergency physicians facing paediatric patients to have painful interventions or unplanned urgent imaging in the emergency room.
Procedural sedation and analgesia (PSA) were introduced in the past decades with the aim to carry out these procedures in a safe environment, minimise the discomfort, pain and psychological trauma, control the anxiety and facilitate amnesia for the threatening experience in addition to early and safe hospital discharge.
Method
We did a retrospective data analysis of all PSA in patients below the age of 12, being carried out in our urgent care centre (UCC) from October 2018 to August 2019. Clinical notes were retrieved and being reviewed by our senior nurse with a pre-designed check-list. The review was approved by the hospital ethics committee. Written informed consent was not necessary because no specific patient privacy data have been included in the manuscript.
Results
There were 144 patients, ranging from 1 to 12 years of age with the average age of 4.2 years old. There were five children under 2 years of age. The commonest indication for PSA was to facilitate suture, 132 (Table 1). Majority of them, 141 received intramuscular ketamine ranged from 2 to 4 mg/kg, others received combination of oral chloral hydrate, intravenous ketamine, intravenous midazolam and local anaesthetics. Twenty-two of them considered for having inadequate sedation with initial medications, four of them required additional dose or medications. The duration of the procedures ranged from 7 to 25 min with the mean time spent of 16 min. Time for regaining consciousness ranged from 15 to 140 min with the median time of sedation in the range of 45–60 min. There was no documented airway compromise or desaturation. Ten children reported to have vomiting and five of them had vomiting on waking up, none of them required medications for their vomiting (Table 2). About 96.5% discharged home after the procedure from the UCC.
Indications for having PSA for the 144 patients.
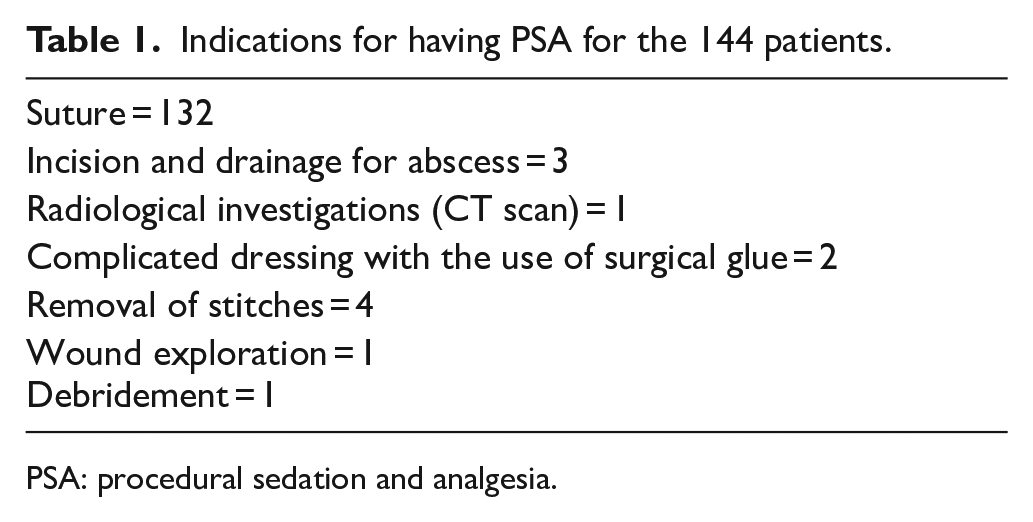
PSA: procedural sedation and analgesia.
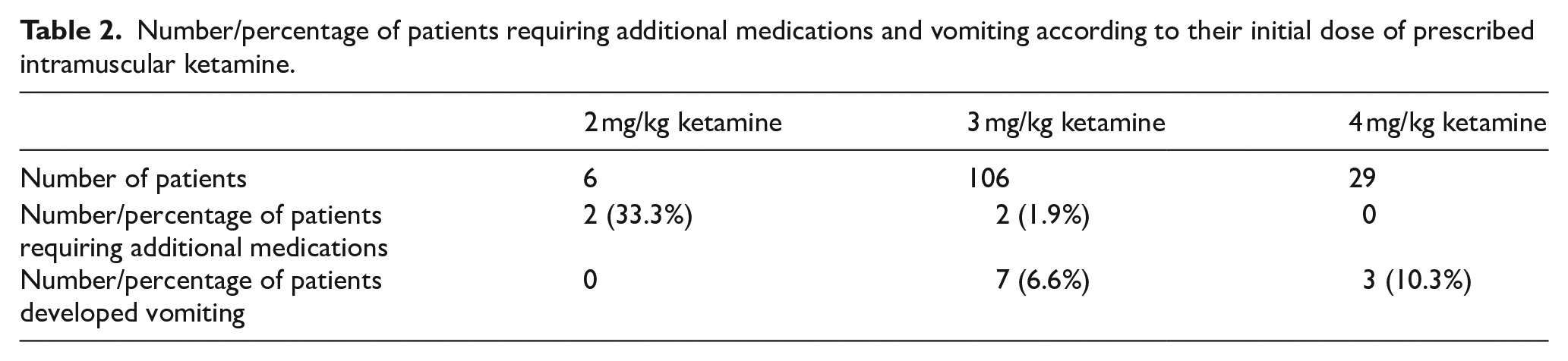
Number/percentage of patients requiring additional medications and vomiting according to their initial dose of prescribed intramuscular ketamine.
Discussion
Our UCC provides 24-h services by a group of nine emergency physicians, all of us are qualified paediatric advanced life support (PALS) providers by American Heart Association (AHA) with average daily attendance of 164 patients in a 304
All PSAs were carried out in the resuscitation room with informed consent, indications and potential complications of the intended procedures and PSA; alternatives including different means to carry out the intended procedures would be discussed and explained by case doctors, obtained prior to the intended procedures. The case doctor would be responsible for carrying out the procedure, while a designated nurse would be responsible for monitoring and documentation during the procedure. Dual lumen end-tidal carbon dioxide (ETCO2)/oxygen supplemental cannula were connected with continuous ETCO2 and SpO2 monitoring (Figure 1). Baseline vital signs including blood pressure, pulse and respiratory rate were taken and then regularly at 5-min interval afterwards. The degree of sedation was measured by simple clinical method of AVPU, (Alert, response to Verbal or Painful stimulation and Unresponsive) regularly as well. Ketamine (50 mg/1 mL) preparation was used. For intramuscular ketamine, injection was done by the case doctor or nurses over the buttock or the thigh area. Paediatric resuscitation equipment was ready and available. The child was being monitored by a designated nurse during the sedation process till they woke up and discharged or admitted to the hospital.
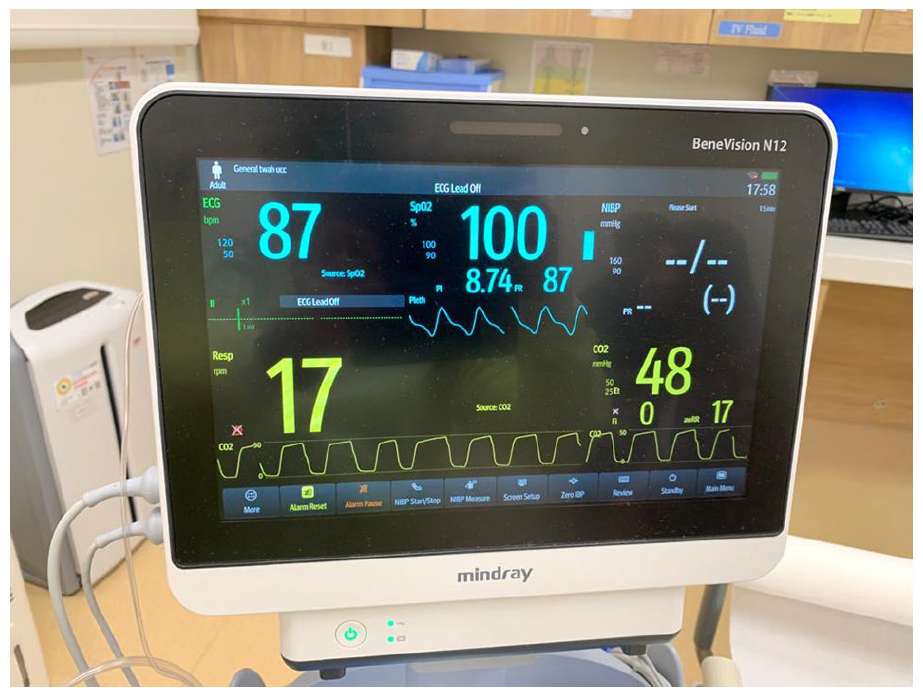
Dual-end tidal carbon dioxide and oxygen supplement cannula.
This is a retrospective clinical records review and analysis of all PSA in patients below the age of 12, being carried out in our UCC from October 2018 to August 2019.
A total of 144 children underwent PSAs during the study period, ranging from 1 to 12 years of age, with the mean age of 4.2 years old; only five of them are younger than 2 years of age. Most (57.7%) of the PSAs were carried in the evening shift, from 16:00 to mid-night. More than 90% of them had PSA for suturing in UCC, and the rest were for incision and drainage of abscess, complicated wound dressing, urgent computed tomography (CT) scan, removal of stitches, wound exploration and wound debridement. Indeed, suturing, repair or exploration of wounds was considered to be the commonest indications of PSA in paediatric patient groups. 1
Almost 98% (141/144) of them received intramuscular ketamine, ranging from 2 to 4 mg/kg, the rest were given combinations of oral choral hydrate, intravenous ketamine, intravenous midazolam or local anaesthesia. For those having intramuscular ketamine, up to 75%, 106 of the 141 received 3 mg/kg intramuscular ketamine as the initial dose. One-third of patients required additional medications when they were given initial dose of 2 mg/kg ketamine, while only 1.5% required additional medication if they received more than 3 mg/kg ketamine as the initial dose. Hartling et al. 2 reported the use of ketamine, midazolam, nitrous oxide and propofol to be safe in paediatric emergency procedural sedation. Our initial ketamine dose followed the protocol suggested by Holloway et al. 1
On average, the patients would be sedated for about 1 h time, 61 min, median duration of sedation was 45–60 min. It was sufficient for all procedures being done, time required for the procedures ranged from 7 to 25 min with the mean time spent of 16.28 min. However, the range for sedation was wide, from 15 to 140 min. For patients receiving initial dose of 2 mg/kg intramuscular ketamine, they might end up in inadequate sedation requiring additional medications or they would have relatively short period of sedation. For patients having the procedure done in the late evening or around mid-night, they had relatively long duration of sedation time. We postulated they were sleeping in their usual time instead of being sedated. We seldom actively waked them up especially when they were stable clinically.
There was no documented airway compromise or desaturation. One patient was given 2 L/min of supplementary oxygen via the dual nasal cannula as he was noticed to be unconscious during the procedure; his saturation was 97%−100% all along. There was no documented airway, ventilation or circulation compromise in our audit.
Ten patients reported vomiting after the procedure, none in the 2 mg/kg IM ketamine group, 6.6% in the 3 mg/kg IM ketamine group and 10.3% in the 4 mg/kg IM ketamine group. Most of the vomiting happened shortly after waking up. However, none of them required additional medications. There were no long-term adverse effects being reported during their subsequent follow-up. Indeed, ketamine was known to have post-procedural emesis up to about 12.3% in various studies. 3 Bellolio et al. 4 reported 80.7 vomiting per 1000 sedation. Suryaprakash and Tham 5 reported age of older than 8 was a predictable factor of intramuscular ketamine-associated emesis.
Almost 96.5% discharged home shortly after the procedure from UCC; only five of them were admitted for various reasons, three of them admitted for administrative reasons, one admitted for proper orthopaedic consultation as the child was found to have a tendon injury during wound exploration in UCC, and one admitted for close monitoring as the child developed skin rash and vomiting after the PSA.
After our review, we had a new designed form (Figure 2) in order to facilitate pre-procedure checking for contra-indications of PSA, monitoring during the procedure. Patients were considered safe to be discharge if they were pink in colour, breathing spontaneously, and fully conscious. A well-written discharge checklist and patient information pamphlet was also prepared (Figure 3). It is recommended physicians should consider 2 h of fasting before the intended procedure; however, the degree of urgency and parent’s preference would take into account as well. Indeed, fasting has not been demonstrated to reduce the risk of emesis or aspiration in emergency department procedural sedation 6 as recommended by the American College of Emergency Physicians.
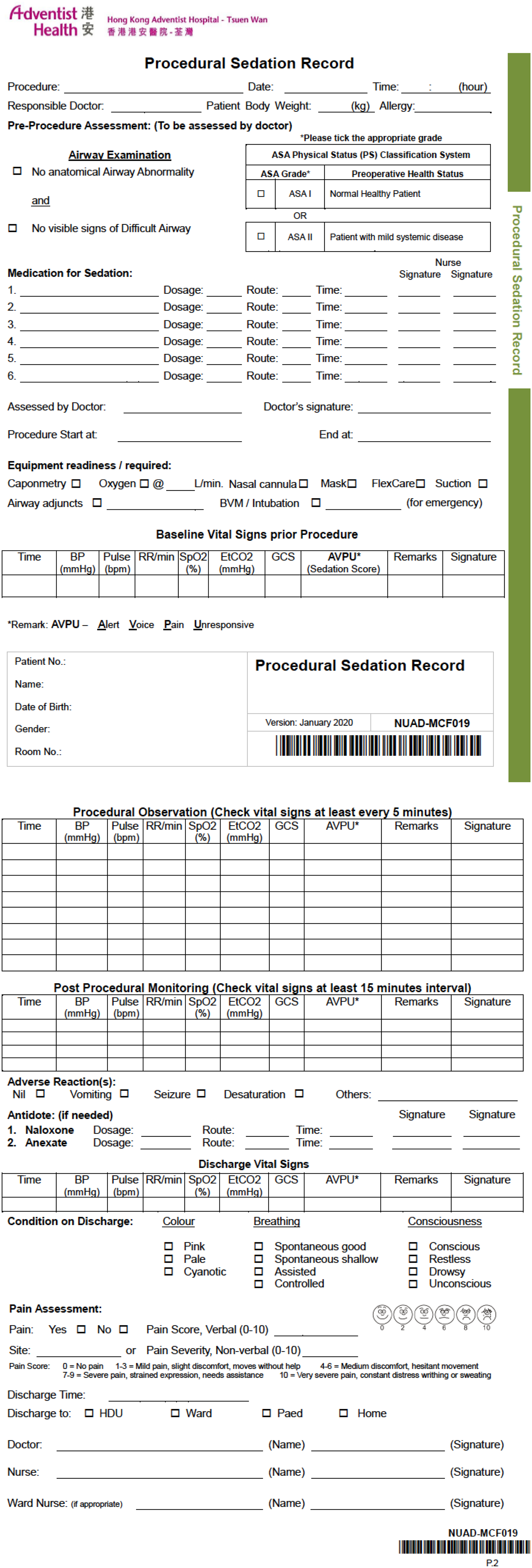
New designed procedural sedation record in Urgent Care Centre of Tsuen Wan Adventist Hospital.
Patient discharge information pamphlet after having procedures requiring procedural sedation and analgesia.
Limitations
This is a retrospective audit. As such, all assessments were based on the documented vital parameters for the reviewer to have the best educated guess on the airway adequacy and patency, respiratory efforts, circulation status and potential complications during the sedation. A prospective observational study with pre-designed forms will provide a more accurate understanding.
Moreover, as majority of cases, 141 out of 144, were using ketamine as the medication choice for the procedure, it may not be possible to generalise similar results in other clinical setting that other routes or medications may be used.
Although it is more reliable and predictable to use intravenous route for the administration of sedatives, balancing parents acceptance, patients experience and potential practical difficulty in setting intravenous route for children, intramuscular injection of ketamine was chosen as an alternative.
Conclusion
Paediatric PSA is generally safe, efficient, adequate and facilitates early patient discharge provided by well-trained and qualified provider under close monitoring in emergency setting with all necessary equipment ready.
Footnotes
Acknowledgements
There is no specific acknowledgement to other potential contributor who does not meet the criteria for authorship
Author contributions
Conceptulisation: MHN. Methodology: KMY, MHN, SLK and DL. Investigation: SLK. Data Curation: KMY and SLK. Formal analysis: KMY and SLK. Project administration: MHN and DL. Visualisation: KMY and SLK. Writing original draft: KMY and SLK. Writing-review and editing: KMY. Supervision: MHN and DL. All authors read and approved the manuscript.
Availability of data
The data sets generated and analysed during this study are available upon request to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Informed consent was obtained for undergoing the procedural sedation and analgesia as usual. However, as no identifying information was collected and its nature of being a retrospective study, no specific informed consent was obtained for the analysis and publication of this article, and it was approved by the Ethics Committee.
Ethical approval
The study was approved by the Hospital Ethics Committee of Tsuen Wan Adventist Hospital on 12 November, 2021.