
Abstract
Background:
Acute myocardial infarction–induced cardiac arrest has high mortality rate.
Objective:
To investigate the risk factors of extracorporeal membrane oxygenation combined with percutaneous coronary intervention in rescuing acute myocardial infarction–induced cardiac arrest.
Methods:
Forty-three eligible patients were assigned into death and survival groups. Their general clinical data, treatment outcomes, and various indicators 24, 48, and 72 h after extracorporeal membrane oxygenation implantation were compared. The factors affecting clinical outcomes were determined by multivariate logistic regression analysis. A nomogram prediction model was constructed and validated.
Results:
After removing extracorporeal membrane oxygenation device, 19 patients recovered and 24 died (mortality rate: 55.81%). The two groups had different conventional cardiopulmonary resuscitation duration, number of diseased vessels, distribution of culprit vessel, time from cardiac arrest to extracorporeal membrane oxygenation implantation, length of stay in critical care unit, and mean arterial pressure 24 and 48 h after extracorporeal membrane oxygenation implantation (p < 0.05). Left anterior descending as the culprit vessel, number of diseased vessels, conventional cardiopulmonary resuscitation duration, time from cardiac arrest to extracorporeal membrane oxygenation implantation, and mean arterial pressure 48 h after extracorporeal membrane oxygenation resuscitation were independent risk factors for death. The predicted mortality rate was 72.6%, and the actual concordance index (C-index) was 0.869. Such indices after internal and external validations were 0.861 and 0.848, respectively, suggesting a good concordance.
Conclusion:
Left anterior descending as the culprit vessel, number of diseased vessels, conventional cardiopulmonary resuscitation duration, time from cardiac arrest to extracorporeal membrane oxygenation implantation, and mean arterial pressure 48 h after extracorporeal membrane oxygenation resuscitation are independent risk factors for patients with acute myocardial infarction–induced cardiac arrest undergoing extracorporeal membrane oxygenation combined with percutaneous coronary intervention.
Keywords
Introduction
Acute myocardial infarction (AMI) is the local necrosis caused by myocardial ischemia and hypoxia due to coronary artery occlusion and a sharp decrease or even interruption of blood supply to the coronary artery. 1 AMI has a raised incidence rate year by year and gradually tends to be prevalent in younger people. AMI is accompanied by such complications as arrhythmia, heart failure, and cardiogenic shock, which is likely to endanger the life of patients if no effective treatment is timely carried out. Statistically, AMI has a high mortality rate (up to 80%), severely affecting the survival of patients. 2 Percutaneous coronary intervention (PCI) is an effective and main treatment approach for AMI, which can improve the blood perfusion of the myocardium. For patients with AMI-induced cardiac arrest (CA), PCI should be carried out after cardiopulmonary resuscitation (CPR). 3 The hemodynamic status of patients with AMI-induced CA is unstable. In addition, traditional mechanical circulation assistance approaches such as intra-aortic balloon pump (IABP) cannot maintain the stability of hemodynamics in patients and complete CPR in time, so that patients miss the best timing for PCI and have a reduced survival rate. 4 Therefore, an effective resuscitation method able to stabilize the hemodynamics of patients with AMI-induced CA is a prerequisite and key for the successful application of emergency PCI, which can greatly improve the success rate of rescue in patients. Extracorporeal membrane oxygenation (ECMO) is a new technology capable of replacing the cardiac pump function, maintaining blood circulation, and providing effective respiratory and circulatory support, which has been widely applied in rescuing critically ill patients as well as AMI-induced CA patients without response to conventional cardiopulmonary resuscitation (CCPR). 5 In this study, the data of AMI-induced CA patients treated with ECMO combined with emergency PCI were retrospectively analyzed to explore relevant influencing factors, so as to provide a theoretical basis for the optimization of rescue plans for patients with AMI-induced CA.
Methods
Baseline clinical data
A total of 43 patients with AMI-induced CA admitted to and treated with ECMO combined with emergency PCI in the Department of Cardiology of our hospital from January 2016 to January 2017 were enrolled as the study subjects. There were 30 males and 13 females aged 44–76 years old, with 58.4 ± 10.5 years old on average.
The inclusion criteria are as follows: (1) patients whose clinical symptoms, medical history, and coronary angiography met the diagnostic criteria for AMI developed by the Canadian Cardiovascular Society (CCS) 6 and (2) those who were diagnosed with CA based on the hemodynamics or electrocardiogram (ECG) monitoring results, and whose time from CA to decision to ECMO implantation was <5 min before CCPR or who had unstable hemodynamic status after CCPR treatments such as administration of CPR drugs, continuous chest compression, electrical defibrillation, and ventilator-assisted respiration.
The exclusion criteria are as follows: (1) patients with CA due to cardiac surgeries or AMI caused by other diseases, (2) those with resurgence of CA after recovery through CCPR, (3) those with irreversible brain death or multiple organ failure, (4) those with abnormal blood coagulation function or malignant tumors, or (5) those unable to receive ECMO implantation due to other personal reasons. This study was approved by the ethics committee of the hospital, and family members of all patients signed the informed consent.
Implantation of ECMO
Patients were intravenously injected with heparin at a dose of 0.5 mg/kg, and a catheter was inserted. Then, a venous-arterial ECMO was implanted, ECMO parameters were set, and an ECMO loop was established, with 1000 mL of artificial colloid (5 mg unfractionated heparin in 500 mL of colloid) as the priming fluid for the catheter. The femoral vein–centrifugal pump–ECMO–femoral artery direction was used as the bypass pathway, and the initial flow rate for ECMO was set at 4.0~5.0 L/min. During bypass, heparin was intermittently injected into patients at a small dose to maintain the activated clotting time at 160 s, and the flow rate was 2~3 L/min. The flow rate was adjusted according to the changes of hemodynamics and blood oxygen saturation–related indicators during operation.
Application of emergency PCI
After ECMO implantation, patients were treated with emergency PCI when the spontaneous circulation returned and various indicators were stable. Before surgery, 300 mg of aspirin and 180 mg of ticagrelor were given for anti-platelet aggregation. 2000 U of heparin was injected through the sheath canal during surgery, and 6000–8000 U of heparin was injected through the sheath canal according to the results of coronary angiography. PCI was performed on relevant diseased vessels. The indicator of successful PCI was residual coronary artery stenosis rate after surgery <20%.
Postoperative ECMO use and withdrawal
If ECMO was continuously used after surgery, the dose of the drug used could be adjusted according to various parameters. When the oxygenation index was greater than 200 mm Hg, and the hemodynamics remained stable, that is, mean arterial pressure (MAP) >70 mm Hg and systemic central venous oxygen saturation (ScVO2) >60%, and other indicators gradually returned to normal, ECMO could be withdrawn tentatively. ECMO could be completely withdrawn if the hemodynamics remained stable. If the hemodynamics was unstable, the device would be used again, and then withdrawn tentatively after the hemodynamics was stable.
Grouping of patients
The patients enrolled were grouped based on their clinical outcomes. Twenty-four patients were assigned into death group, among whom 22 died after removing ECMO device (5 cases of circulatory failure, 14 of multiple organ failure, and 3 cases of cerebral hemorrhage) and 2 died due to circulatory failure before successful removal of ECMO device. Nineteen patients discharged from hospital upon recovery were assigned into survival group.
Observation indices
(1) The general clinical data included age, gender, weight, myocardial infarction location, past history, and smoking history. (2) The clinical treatment status included CCPR duration, SYNTAX score, number of diseased vessels, culprit vessel type, time from CA to ECMO implantation, length of stay in critical care unit (CCU), ECMO initial flow, number of patients receiving IABP, number of patients treated with continuous renal replacement therapy (CRRT), and time of ECMO use, which was observed and compared. (3) The clinical indicators within 72 h after ECMO implantation were as follows: (1) arterial blood gas indicators (pH, partial pressure of carbon dioxide (PCO2), partial pressure of oxygen (PO2), and lactic acid), (2) hemodynamic indexes (central venous pressure (CVP), MAP, ScVO2, heart rate, and left ventricular ejection fraction (LVEF)), and (3) blood indicators (platelet, urea nitrogen, white blood cell, creatine kinase-MB, serum creatinine, and hemoglobin).
Establishment of nomogram prediction model
The patients were assigned into death group and survival group based on their clinical outcomes. The clinical parameters of patients were compared between the two groups, and multivariate logistic regression analysis was adopted to analyze the variables with statistically significant differences, so as to screen out the factors affecting the clinical outcomes of patients. A nomogram prediction model was constructed using the R software (R3.3.2) and rms package.
Evaluation of nomogram prediction model
The discrimination of the model was assessed by receiver operating characteristic (ROC) curve, and the area under the curve was calculated. The concordance index (C-index) ranged from 0.5 to 1, and the closer the value approached 1, the better the concordance between the predicted result and the actual result would be. As to internal validation, the bootstrap method was employed, and the C-index after internal validation was compared with the actual C-index. The closer to 0 the difference between the two values was, the better the concordance of the model would be. A total of 30 patients with AMI-induced CA rescued with ECMO combined with PCI from November 2018 to July 2019 in our hospital were selected for external validation, and the C-index was calculated for evaluating the accuracy of the model. The inclusion and exclusion criteria were the same with those in this study.
Statistical analysis
SPSS 19.0 software and R software (R3.3.2) were utilized for the statistical analysis. Quantitative data are represented as mean value ± standard deviation, and the t-test was performed for intergroup comparisons. Intergroup comparisons of numerical data were conducted with the χ 2 test. The factors affecting the death of patients were analyzed through multivariate logistic regression analysis. p < 0.05 indicated that the difference was statistically significant.
Results
Baseline clinical data
There were no statistically significant differences in the general clinical data of patients between the two groups (p > 0.05; Table 1).
Baseline clinical data.

Treatment outcomes of ECMO
The treatment status of patients was compared between the two groups. The results showed that the time of ECMO use, SYNTAX score, CRRT, use of IABP, and ECMO initial flow displayed no statistically significant differences (p > 0.05), whereas the CCPR duration, number of diseased vessels, culprit vessel distribution, time from CA to ECMO implantation, and length of stay in CCU had statistically significant differences (p < 0.05; Table 2).
Treatment outcomes of ECMO.

ECMO: extracorporeal membrane oxygenation; CCPR: conventional cardiopulmonary resuscitation; CA: cardiac arrest; CCU: critical care unit; IABP: intra-aortic balloon pump; CRRT: continuous renal replacement therapy.
Indicators at 24, 48, and 72 h after ECMO implantation
The indicators within 72 h after ECMO implantation were compared between the two groups of patients. It was found that the MAP at 24 and 48 h after ECMO implantation was significantly higher in survival group than that in death group, showing a statistically significant difference (p < 0.05), while other indicators had no statistically significant differences between the two groups (p > 0.05; Table 3).
Indicators at 24, 48, and 72 h after ECMO implantation.

ECMO: extracorporeal membrane oxygenation; MAP: mean arterial pressure; CVP: central venous pressure; LVEF: left ventricular ejection fraction; PCO2: pressure of carbon dioxide; PO2: pressure of oxygen.
Number of surviving patients.
p < 0.05 versus death group in the same period.
Multivariate logistic regression analysis results
Multivariate logistic regression analysis was conducted with the above indexes with statistically significant differences as independent variables and clinical outcomes (0 = survival and 1 = death) of patients as the dependent variable. It was discovered that the left anterior descending as the culprit vessel, left main coronary artery + triple as the number of diseased vessels, CCPR duration ⩾40 min, time from CA to ECMO implantation ⩾50 min, and MAP at 48 h after ECMO resuscitation <70 mm Hg were independent risk factors resulting in the death of patients (Table 4).
Multivariate logistic regression analysis results of factors affecting clinical outcomes of patients with AMI-induced CA.
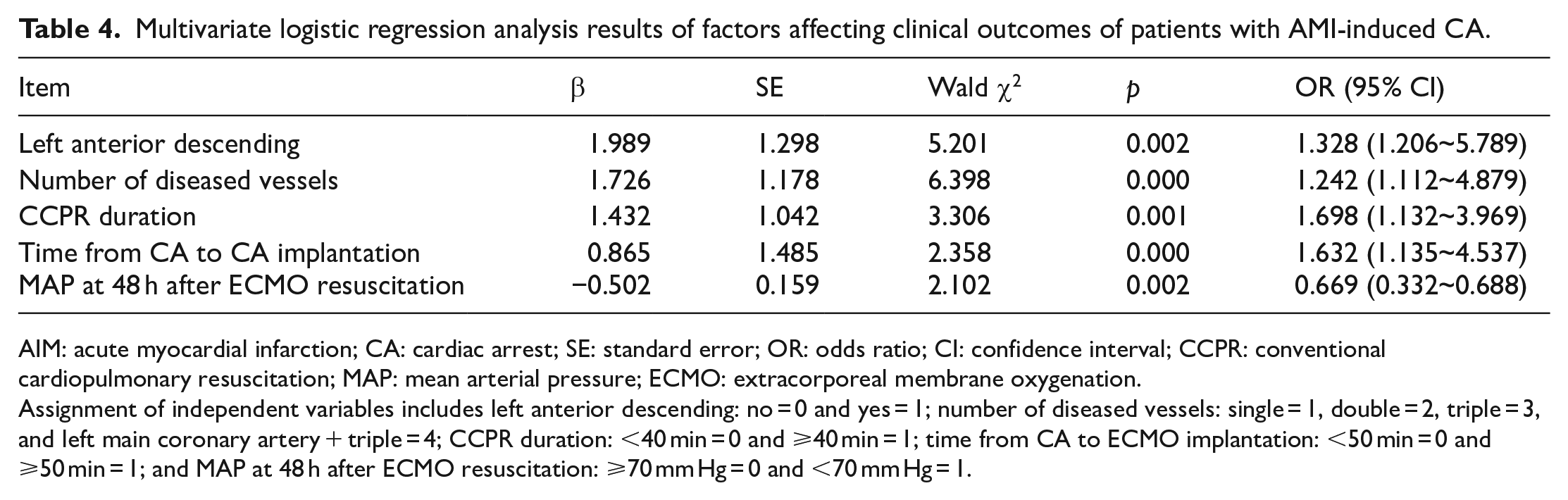
AIM: acute myocardial infarction; CA: cardiac arrest; SE: standard error; OR: odds ratio; CI: confidence interval; CCPR: conventional cardiopulmonary resuscitation; MAP: mean arterial pressure; ECMO: extracorporeal membrane oxygenation.
Assignment of independent variables includes left anterior descending: no = 0 and yes = 1; number of diseased vessels: single = 1, double = 2, triple = 3, and left main coronary artery + triple = 4; CCPR duration: <40 min = 0 and ⩾40 min = 1; time from CA to ECMO implantation: <50 min = 0 and ⩾50 min = 1; and MAP at 48 h after ECMO resuscitation: ⩾70 mm Hg = 0 and <70 mm Hg = 1.
Establishment of nomogram prediction model
The nomogram prediction model of factors relating to the death of patients was constructed using the R software based on the results of multivariate analysis. The left anterior descending as the culprit vessel was scored 35 points, the left main coronary artery + triple as the number of diseased vessels was scored 41.5 points, the CCPR duration ⩾40 min was scored 39 points, the time from CA to ECMO implantation ⩾50 min was scored 45 points, and the MAP at 48 h after ECMO resuscitation <70 mm Hg was scored 39 points. The corresponding value to the total score (199.5 points) of the above items was the incidence rate (72.6%) of death in patients predicted in the model (Figure 1).
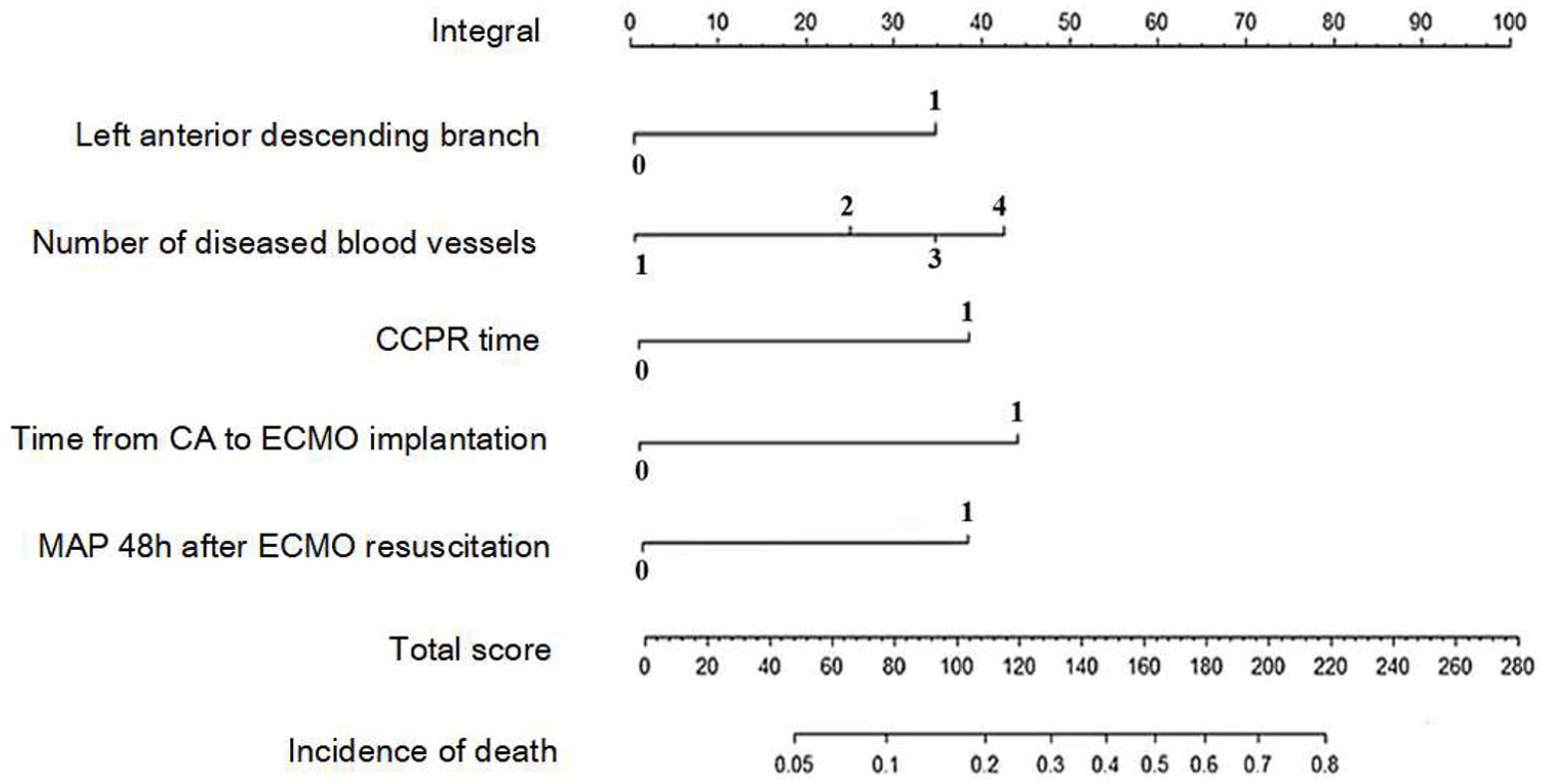
Nomogram prediction model of factors affecting death of patients.
Evaluation of nomogram prediction model
The discrimination of the model was tested to evaluate the concordance of the model. The results revealed that the actual C-index of the model was 0.869. According to the results of internal validation and external validation, the C-index was 0.861 and 0.848, respectively. The difference between the actual C-index of the model and the C-index after internal validation was 0.08, suggesting that the model had good concordance and high accuracy (Figure 2).
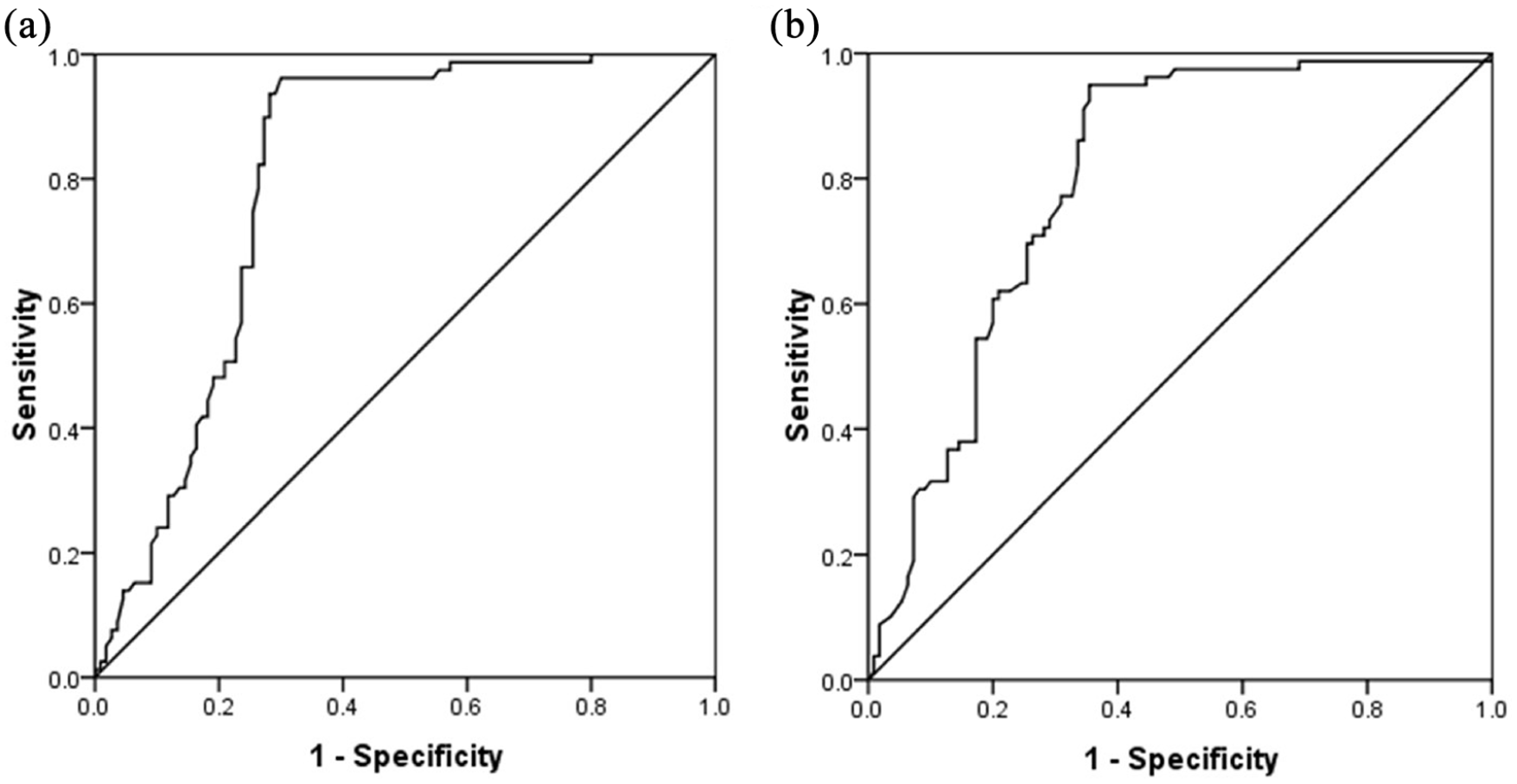
Assessment of nomogram prediction model for death of patients: (a) before internal calibration and (b) after internal calibration.
Discussion
The effect of CCPR on the rescue of AMI-induced CA is not satisfactory, which can only provide 25%–40% of the cardiac output before CA. 7 Vasoactive agents can adjust vasomotion, so they are used in the rescue of CA, but they will significantly increase myocardial oxygen consumption, cause myocardial ischemia, induce arrhythmia, and damage myocardial cell function if used in a large dose. 8 Coronary revascularization is an effective means to treat AMI patients, but a stable hemodynamic status before surgery is a precondition for successful rescue. 9 For this reason, providing ideal cardiopulmonary bypass support technology to maintain relatively stable hemodynamics can increase the survival rate of patients with AMI-induced CA.
As a novel technology, ECMO is able to maintain blood circulation, stabilize hemodynamics, and act as an artificial blood pump to effectively replace the heart function and reduce the burden on the heart. Besides, ECMO can also provide external respiratory support, exert cardiac pump function, and relieve the ischemia and hypoxia of tissues and organs. As a result, ECMO can create the conditions for emergency PCI and improve the survival rate of patients. 10 It is recommended in the 2015 American Heart Association (AHA) guidelines for CPR that ECMO may be adopted in treating patients with reversible factors-induced CA. 11
The survival rate of patients with AMI-induced CA undergoing ECMO combined with PCI is 45.9%, 12 being consistent with the results herein. In this study, the success rate of ECMO in the 43 patients with AMI-induced CA was 100%, all patients had recovered spontaneous heartbeat, and the success rate of emergency PCI after CPR was 44.19% (19/43). It has been reported that the culprit vessel type, number of diseased vessels, CCPR duration, and the time from CA to ECMO implantation are independent risk factors affecting the clinical outcomes of patients with AMI-induced CA. 13 In this study, patients were assigned into death group and survival group based on their clinical outcomes. Then, the general clinical data, ECMO treatment status, and various clinical indexes were compared between the two groups of patients. It was found that the CCPR duration, number of diseased vessels, distribution of culprit vessel, time from CA to ECMO implantation, length of stay in CCU, and MAP at 24 and 48 h after ECMO implantation showed statistically significant differences between the two groups of patients (p < 0.05). Next, the above indicators with statistically significant differences were subjected to multivariate logistic regression analysis. The results showed that the number of diseased vessels, CCPR duration, the left anterior descending as the culprit vessel, MAP at 48 h after ECMO resuscitation, and time from CA to ECMO implantation were independent risk factors resulting in the death of patients.
CCPR duration <40 min is an independent risk factor for the survival of patients. 14 The results of this study revealed that the CCPR duration was 30.8 ± 6.7 min in survival group, in line with that in the relevant literature, whereas it was 48.9 ± 20.6 min in death group, which was markedly prolonged. Research manifested that the MAP at 48 h after ECMO implantation reflects the stability of the hemodynamics in patients and is also an independent risk factor for the survival and discharge of patients. 15 In this study, the MAP of patients at 48 h after ECMO implantation was clearly higher in survival group than that in death group, consistent with that reported in the literature. A study reported that the left anterior descending as the culprit vessel is an important independent risk factor for the death of patients. 16 It was found in this study that the proportion of patients with the left anterior descending as the culprit vessel was obviously higher in death group than that in survival group (58.33% vs 21.05%), consistent with that in the literature. Hence, during ECMO treatment, the establishment of rapid standard operating procedures, shortening of the hypoperfusion time before ECMO treatment, rapid rescue with ECMO, and close monitoring of blood pressure can signally improve the survival rate of patients. It is worth noting that ECMO device, a non-biocompatible material, will cause greater damage to the blood system after implantation, and its long-term application may lead to severe complications. Therefore, timely removal of the device should be considered when the condition of patients is restored and stable.
The nomogram prediction model graphs and visualizes the results of multivariate logistic regression analysis, which intuitively displays the influencing factors of clinical events and quantifies their risks, thereby offering reliable support for the development of reasonable treatment plans in clinical practice. 17 In this study, the nomogram prediction model was established with the results of multivariate logistic analysis to predict the relevant factors affecting the death of patients, and it was evaluated. It was uncovered that the actual C-index of the model was 0.869, the C-index was 0.861 after internal validation performed by repeated sampling through the bootstrap method and 0.848 after external validation, and the model had good concordance. This indicates that such a model has high prediction accuracy and can effectively predict the risk factors affecting the death of patients.
Conclusion
In conclusion, the number of diseased vessels, CCPR duration, left anterior descending as the culprit vessel, MAP at 48 h after ECMO resuscitation, and time from CA to ECMO implantation are independent risk factors leading to the death of patients. However, there were some shortcomings in this study. For instance, the sample size was small, and the impact on postoperative long-term survival in survival group needs to be further studied.
Footnotes
Acknowledgements
The author is grateful for the cooperation of all included subjects.
Author contribution
J.Y. performed this study and prepared this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data sets used in this study are available from the corresponding author on reasonable request.
Ethical approval
The study was approved by the ethical committee of The Affiliated Union Hospital of Fujian Medical University.
Informed consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Human rights statement
This study has been conducted in full accordance with the ethical standards of institutional committee on human subjects as well as with the Helsinki Declaration.