
Abstract
Introduction:
The risk of venous thromboembolism increases after acute carbon monoxide poisoning. However, studies on the characteristics of patients who develop venous thromboembolism after carbon monoxide poisoning are rare. The aim of this study was to identify the risk factors for venous thromboembolism within 3 months after carbon monoxide poisoning.
Methods:
This is a population-based study that employed nationwide claims data from South Korea. Among the carbon monoxide poisoning patients (⩾18 years), the characteristics of the groups with and without venous thromboembolism (pulmonary embolism or deep vein thrombosis) were identified. All the significant variables in the univariable analysis were included in the multivariable logistic regression to determine the risk factors for venous thromboembolism occurrence.
Results:
Among the 24,232 carbon monoxide poisoning patients, 130 subjects developed venous thromboembolism within 90 days of their carbon monoxide poisoning diagnosis. The significant risk factors for venous thromboembolism in the multivariable analysis were age (adjusted odds ratio (aOR) = 1.01; 95% confidence interval (CI) = 1.003–1.03), intensive care unit admission (aOR = 3.80; 95% CI = 2.34–6.12), length of stay (aOR = 1.02; 95% CI = 1.0001–1.04), congestive heart failure (aOR = 2.17; 95% CI = 1.36–3.42), and cancer (aOR = 1.94; 95% CI = 1.10–3.22). The adjusted odds ratios for intensive care unit admission for patients with pulmonary embolism and deep vein thrombosis were 3.05 (95% CI = 1.61–5.61) and 5.60 (95% CI = 2.89–10.90), respectively.
Conclusion:
Patients with older age, intensive care unit admission, a longer length of stay, congestive heart failure, or cancer are at greater risk of developing venous thromboembolism after carbon monoxide poisoning. In particular, intensive care unit admission was the strongest risk factor for venous thromboembolism, pulmonary embolism, and deep vein thrombosis. Monitoring and administering prophylactic treatments to prevent venous thromboembolism would be helpful in high-risk in carbon monoxide poisoning patients.
Keywords
Introduction
Carbon monoxide (CO) is generated when carbon-containing fuels are incompletely burned with insufficient oxygen, and the inhalation of CO can cause serious complications or even death. 1 The common complications of CO poisoning are neurological and myocardial injuries.2,3 In addition, thrombus formation can occur in various parts of the body after CO poisoning. Cases of ST-segment elevation myocardial infarction,4–6 drug-released stent occlusion,7,8 or thrombus inside the heart, such as in the right atrium or left ventricle,9–12 after acute CO poisoning have been reported. Cases of cerebral infarction caused by thrombus in the internal carotid artery have been reported. 13
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a serious condition with high morbidity and mortality. 14 Cases of VTE after CO poisoning have been reported, and some patients have even experienced cardiac arrest.15–17 In a recently published population-based study, we showed that the risk of developing VTE after CO poisoning persists for up to 3 months. 18 In that study, the risk of VTE occurrence within 3 months after CO poisoning was found to be 4 times higher than at baseline and the risk at 1 month was 13 times higher than at baseline. Therefore, it is necessary to identify the characteristics of patients at a higher risk of VTE among those who experience CO poisoning and monitor these patients more closely. However, studies on the risk factors for VTE occurrence after CO poisoning are rare. The purpose of this study was to identify the risk factors for VTE within 3 months after CO poisoning.
Methods
Database
This is a population-based study using claims data from the National Health Insurance Service (NHIS) of South Korea (NHIS-2018-1-195). The NHIS is a nationwide health insurance system that covers 97% of 50 million people. The NHIS database includes demographic information, the International Classification of Diseases–10th Revision (ICD-10) codes, treatment and prescription information, and the date of death. The institutional review board of Hanyang University Hospital in Korea approved the study (IRB No. HYUH 2018-04-032).
Study population
Patients aged 18 years or older who were diagnosed with CO poisoning from 1 January 2004 to 31 December 2016 were included. Eligible patients were defined as those with a diagnostic code for CO poisoning (ICD-10: T58), and both inpatients and outpatients were included. For patients with multiple diagnoses of CO poisoning, it was not possible to distinguish whether they had been exposed to multiple poisonings or simply received follow-up care after the first exposure. Therefore, only patients who were diagnosed with CO poisoning once were included. The date of cohort enrollment, which was the day on which CO poisoning was first diagnosed, was defined as the index date. Patients who had already been diagnosed with CO poisoning during the 2-year washout period prior to the index date were excluded.
Outcomes and covariates
The primary outcome of this study was the first occurrence of VTE. Patients with VTE were defined as those with diagnostic codes for PE (I26) and DVT (I80.x) in both outpatient and inpatient settings. PE and DVT were analyzed separately as secondary outcomes.
Covariates that could affect VTE included age, sex, place of treatment, length of stay, hospitalization with accompanying burns, comorbidities, and commonly known thromboembolism risk factors. The comorbidities included hypertension, diabetes, hypercholesterolemia, congestive heart failure, arrhythmia, chronic obstructive pulmonary disease (COPD), renal failure, liver cirrhosis, all types of cancer, thrombophilia, and inflammatory bowel disease. For the known VTE risk factors, lower limb fracture, surgery, hormone replacement therapy, pregnancy, tamoxifen, glucocorticoids, and antidepressants were included as covariates. The covariate definitions are detailed in Table S1. The known VTE risk factors were defined as having corresponding disease, treatment, or drug classification codes within 90 days prior to the index date. Comorbidities were defined as having the relevant ICD-10 codes more than two times as an outpatient or one or more times as an inpatient within 2 years before the index date. Treatment codes or drug classification codes were included as covariates even if they were prescribed only once. The places of treatment were classified as outpatient, general ward admission, and intensive care unit (ICU) admission. In the multivariable analysis, outpatients were set as a reference value to confirm the risk of VTE in patients who were admitted to the general ward and those admitted to the ICU. The length of stay was set as 1 day for outpatients and as the duration of hospitalization for inpatients. Being hospitalized for burns with a diagnosis of CO poisoning was included as a variable.
Statistical analyses
Among the CO poisoning patients, the patients who developed VTE during the first 3 months after the index date were the subjects, and the patients who did not develop VTE were the controls. Subjects and controls were defined based on whether they were assigned a code indicating a diagnosis of VTE, and whether or not they died during the 90-day follow-up period. The baseline characteristics are presented as mean (standard deviation) or median (interquartile range) for continuous variables and as frequency (%) for categorical variables. A univariable analysis was performed to compare the characteristics of CO poisoning patients with VTE with those of the control group. The continuous variables were tested for the normality of distribution using the Anderson–Darling test, and a Student’s t-test or Wilcoxon rank sum test was performed, as appropriate. Fisher’s exact test was performed for categorical variables. All variables with a p-value less than 0.05 according to the univariable analysis were included in the multivariable analysis to determine the independent risk factors. Logistic regression was used for multivariable analysis, and adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were calculated. The goodness of fit of the logistic model was confirmed by the Hosmer–Lemeshow test.
As in our previous study, we used a cohort-crossover design to reconfirm whether the risk of VTE occurrence after CO poisoning was increased. The cohort-crossover design excludes the effects of between-person confounders by setting their own different periods as control. The period up to 90 days after CO poisoning was compared with the period after 1 year in the same patient. The ORs and 95% CIs were calculated using conditional logistic regression for CO poisoning patients who could be followed for 1 year and 90 days (455 days), excluding patients who died during the follow-up period because they could not have a crossover period. Statistical analyses were conducted using SAS Enterprise Guide version 7.1 software (SAS Institute, Inc., Cary, NC) and R version 3.5.2 (www.R-project.org).
Results
Characteristics of the study population
A total of 24,406 patients aged 18 years or older were diagnosed with CO poisoning once between 2004 and 2016 (Figure 1). Ultimately, 24,232 patients were included, excluding 174 patients who were diagnosed with VTE within 2 years prior to the index date. Among these patients, 130 subjects were diagnosed with VTE within 90 days after the index date, and 24,102 controls were not diagnosed with VTE within 90 days. Of the 24,232 CO poisoning patients, 1071 (4.4%) died within 90 days: 19 (14.6%) patients in the VTE group and 1052 (4.4%) patients in the non-VTE group died within 90 days after CO poisoning.
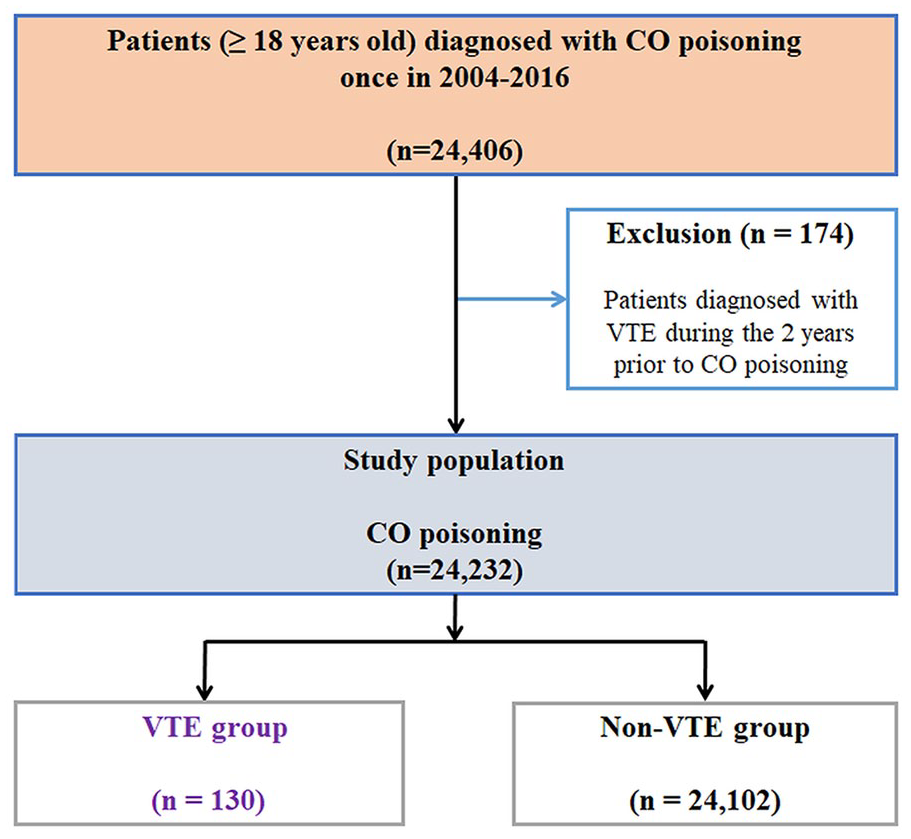
Study flow chart.
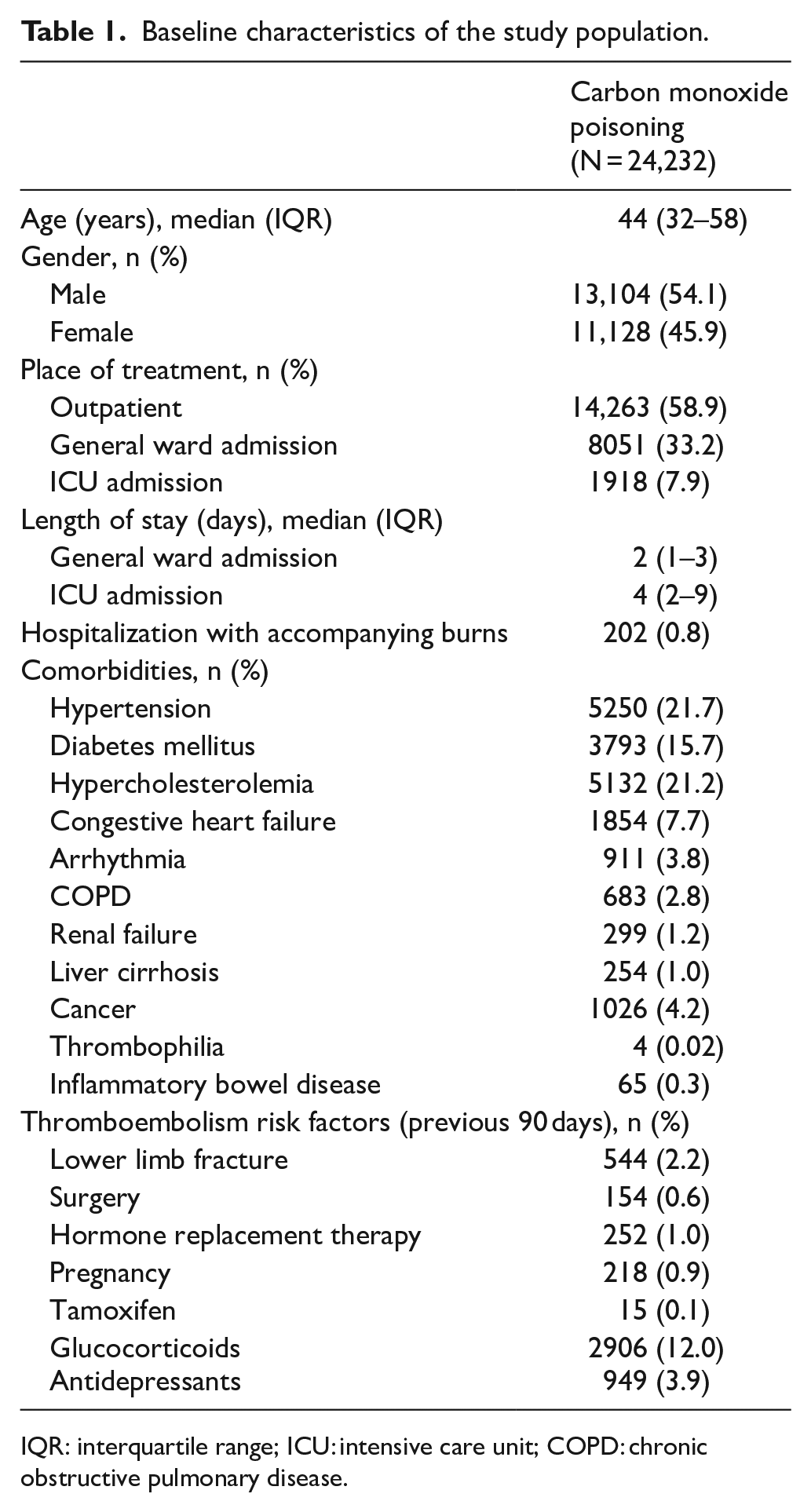
The baseline characteristics of the study population are shown in Table 1. The median age was 44 years (interquartile range (IQR): 32–58 years), and the sex distribution was 54.1% men and 45.9% women. The places of treatment for the study population were 58.9%, 33.2%, and 7.9% in outpatient settings, general wards, and ICUs, respectively. A total of 0.8% of the study population was hospitalized with burns.
Baseline characteristics of the study population.
IQR: interquartile range; ICU: intensive care unit; COPD: chronic obstructive pulmonary disease.
Excluding 2709 patients who could not be followed for 1 year and 90 days (455 days), 21,523 CO poisoning patients were analyzed to reconfirm the association between CO poisoning and the increased risk of incident VTE. The ORs (95% CIs) for incident VTE, PE, and DVT within 90 days after CO poisoning were 4.04 (2.56–6.38), 11.40 (4.57–28.44), and 2.26 (1.32–3.88), respectively.
Risk factors for VTE within 3 months after CO poisoning
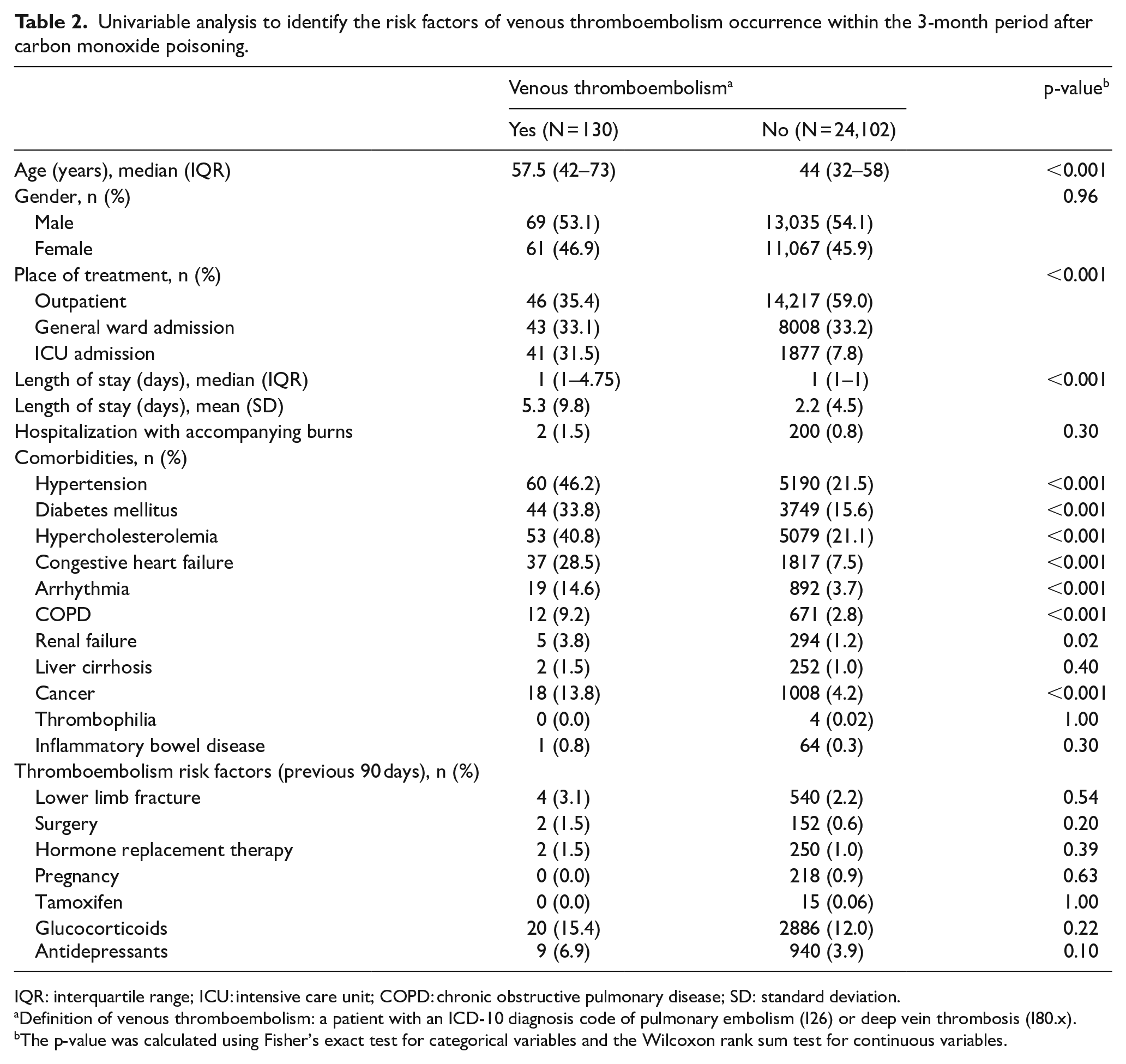
Table 2 shows the results of the univariable analysis performed to identify the risk factors for VTE development within 3 months after CO poisoning. The age of the VTE group (median = 57.5 years; IQR = 42–73 years) was older than that of the non-VTE group (median = 44 years; IQR = 32–58 years). The sex distribution was 53.1% men and 46.9% women in the VTE group and 54.1% men and 45.9% women in the non-VTE group. The proportion of outpatients in the VTE group (35.4%) was smaller than that in the non-VTE group (59.0%), and the proportion of patients with ICU admissions was higher in the VTE group (31.5%) than in the non-VTE group (7.8%). Except for liver cirrhosis, thrombophilia, and inflammatory bowel disease, the proportion of other comorbidities was significantly higher in the VTE group than in the non-VTE group. The proportions of patients with lower limb fractures, surgery, hormone replacement therapy, pregnancy, tamoxifen, glucocorticoids, antidepressants, and hospitalization with burns were not significantly different between the VTE and the non-VTE groups.
Univariable analysis to identify the risk factors of venous thromboembolism occurrence within the 3-month period after carbon monoxide poisoning.
IQR: interquartile range; ICU: intensive care unit; COPD: chronic obstructive pulmonary disease; SD: standard deviation.
Definition of venous thromboembolism: a patient with an ICD-10 diagnosis code of pulmonary embolism (I26) or deep vein thrombosis (I80.x).
The p-value was calculated using Fisher’s exact test for categorical variables and the Wilcoxon rank sum test for continuous variables.
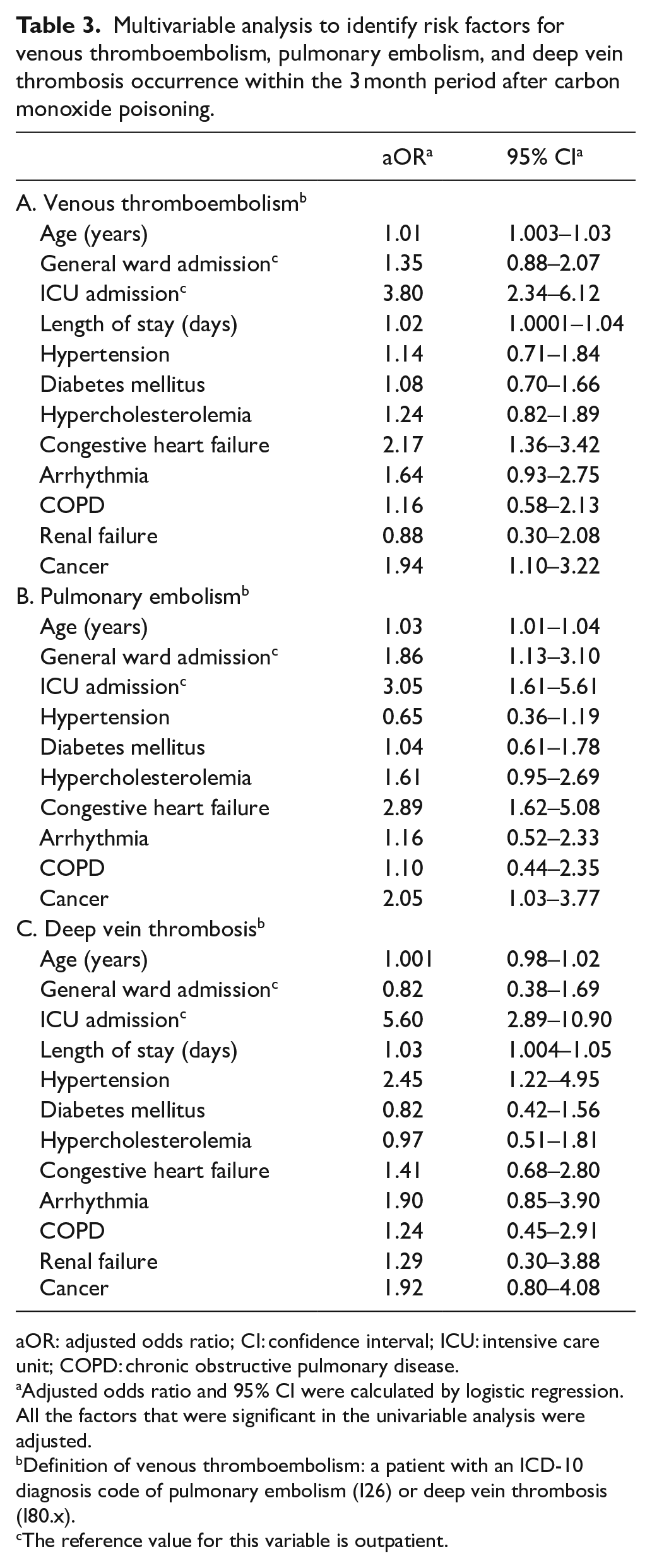
Multivariable analysis was performed by including all significant factors (p-value < 0.05) from the univariable analyses, and we determined the risk factors for VTE within 3 months after CO poisoning (Table 3 (panel A); Figure 2). The significant risk factors for VTE according to the multivariable analysis were age (aOR = 1.01; 95% CI = 1.003–1.03), ICU admission (aOR = 3.80; 95% CI = 2.34–6.12), length of stay (aOR = 1.02; 95% CI = 1.0001–1.04), congestive heart failure (aOR = 2.17; 95% CI = 1.36–3.42), and cancer (aOR = 1.94; 95% CI = 1.10–3.22). The p-value of the Hosmer–Lemeshow test for the multivariable logistic model of VTE was 0.587, indicating that the model fit well.
Multivariable analysis to identify risk factors for venous thromboembolism, pulmonary embolism, and deep vein thrombosis occurrence within the 3 month period after carbon monoxide poisoning.
aOR: adjusted odds ratio; CI: confidence interval; ICU: intensive care unit; COPD: chronic obstructive pulmonary disease.
Adjusted odds ratio and 95% CI were calculated by logistic regression. All the factors that were significant in the univariable analysis were adjusted.
Definition of venous thromboembolism: a patient with an ICD-10 diagnosis code of pulmonary embolism (I26) or deep vein thrombosis (I80.x).
The reference value for this variable is outpatient.
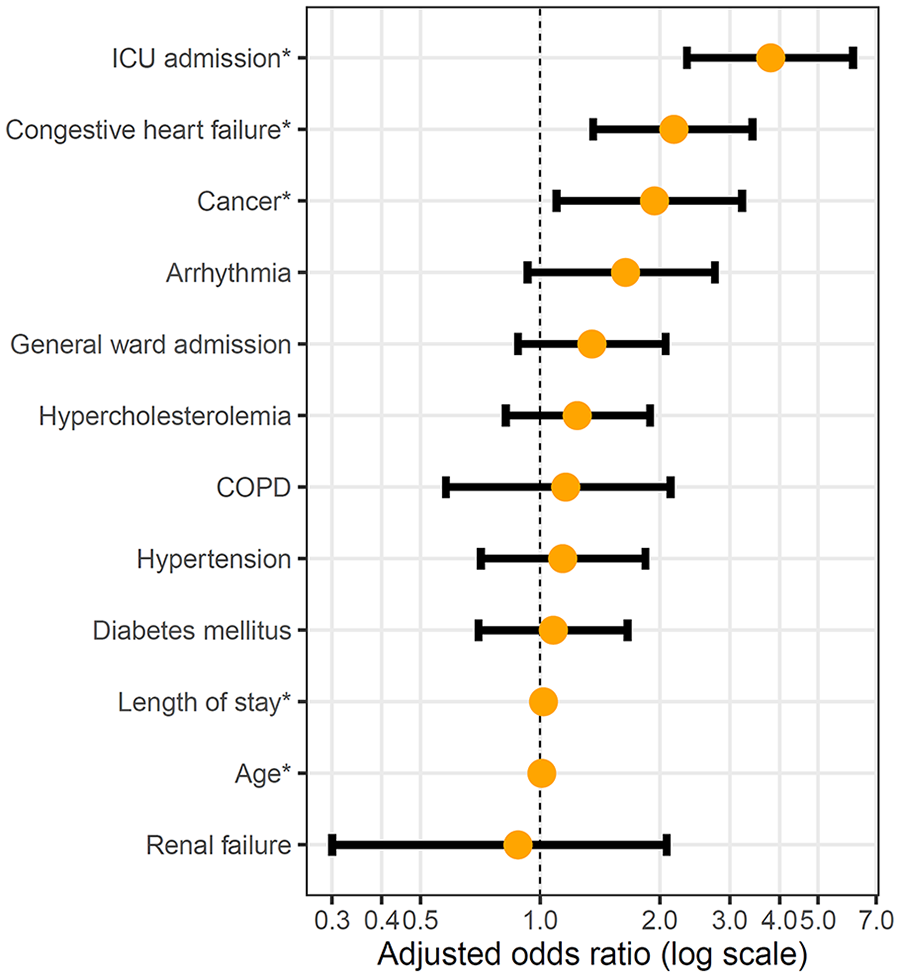
Adjusted odds ratios of risk factors for venous thromboembolism occurrence within the 3-month period after carbon monoxide poisoning.
Risk factors for PE and DVT within 3 months after CO poisoning
We identified the risk factors for PE and DVT. Of the 24,232 patients, 82 subjects were diagnosed with PE and 24,150 controls were not diagnosed with PE within 3 months after CO poisoning. Among the 24,232 CO poisoning patients, DVT occurred within 3 months in 58 patients and did not occur in 24,174 patients; 10 patients were diagnosed with both DVT and PE. Tables S2 and S3 show the univariable analysis results for the occurrence of PE and DVT, respectively.
Table 3 (panel B) shows the results of the multivariable analysis to identify the risk factors for PE within 3 months after CO poisoning. The significant risk factors for PE were age (aOR = 1.03; 95% CI = 1.01–1.04), general ward admission (aOR = 1.86; 95% CI = 1.13–3.10), ICU admission (aOR = 3.05; 95% CI = 1.61–5.61), congestive heart failure (aOR = 2.89; 95% CI = 1.62–5.08), and cancer (aOR = 2.05; 95% CI = 1.03–3.77). Table 3 (panel C) shows the risk factors for DVT within 3 months after CO poisoning. The significant factors for DVT were ICU admission (aOR, 5.60; 95% CI = 2.89–10.90), length of stay (aOR = 1.03; 95% CI = 1.004–1.05), and hypertension (aOR = 2.45; 95% CI = 1.22–4.95). The p-values of the Hosmer–Lemeshow test for the multivariable logistic model of PE and DVT were 0.491 and 0.686, indicating that the models fit well.
Discussion
This study identified the risk factors for VTE among patients with CO poisoning. Because VTE is a low-incidence disease, a sufficient number of subjects are required to identify the risk factors. In this study, a population-based study was conducted on 24,232 CO poisoning patients, and 0.5% (n = 130) of these patients developed VTE within 3 months. We found that CO poisoning patients with older age, ICU admission, a longer length of stay, congestive heart failure, and cancer were at higher risk. In particular, ICU admission was the strongest risk factor for VTE, PE, and DVT, respectively.
VTE has an annual incidence of approximately 1 in 1000 in Western populations and 13.8 to 19.9 in 100,000 in Asian populations. 19 The mortality rate within 3 months after PE occurrence is 8.6%–17%,20–22 and more than 50% of patients with hemodynamically unstable PE die. 20 Therefore, it is important to identify the risk factors for VTE occurrence and implement measures to prevent VTE in high-risk patients. Several studies and case reports have reported that CO poisoning is a potential risk factor for VTE.15–17,23,24 CO forms carboxyhemefibrinogen (COHF), which increases the activity of fibrinogen and induces blood clotting.25,26 In addition, in patients with CO poisoning, oxidative stress is increased around the blood vessels, 27 which may cause platelet aggregation and endothelial cell damage, resulting in blood clots.12,28 Risk factors for VTE cannot be identified in 1/3 to 1/2 of patients, but other patients experience VTE caused by various triggers of hypercoagulability and endothelial injury. 29
In this study, the strongest risk factor for VTE among CO poisoning patients was ICU admission. The aORs for VTE, PE, and DVT in patients admitted to the ICU were 3.80, 3.05, and 5.60, respectively. Critically ill patients are at high risk of developing VTE. 30 The incidence of DVT in patients admitted to the ICU was reported to be approximately 5.4% to 9.6% in recent studies.31,32 PE was clinically suspected in 0.4% to 1.9% of medical ICU patients.33,34 In our study, the incidence of PE among ICU inpatients was 0.9%, which was similar to the results of the previous studies, and the incidence of DVT was 1.4%, which was lower than the incidence reported in other cohorts. In case reports on CO poisoning patients who developed VTE, PE was more common than DVT.15–17 The reason for this trend is still unclear, but it is believed that VTE is more often diagnosed due to the clinical manifestations of PE rather than those of DVT in CO poisoning patients. In a case report, a CO poisoning patient was diagnosed with only PE without DVT. 17 This finding is presumedly due to poor screening for VTE in CO poisoning patients, and it is assumed that PE is often diagnosed only after clinical manifestations such as dyspnea, hypoxemia, and cardiac arrest. In a case series reporting five CO poisoning patients who developed PE, tests for DVT were not performed or DVT was not found. 15 In our study, 22% of the patients with PE and 47% of the patients with DVT had been admitted to the ICU, and the risk was greater because the proportions of patients admitted to the ICU were higher than those in the non-PE and non-DVT groups, respectively. It is necessary to monitor and prevent the occurrence of VTE in CO poisoning patients who are receiving critical care. 35
Heart failure is a risk factor for VTE, and Tang et al. 36 reported a risk ratio of 1.51 that was obtained through a meta-analysis. In the cohort of CO poisoning patients, the aOR for incident VTE in patients with heart failure was 2.08. Heart failure not only increases the risk of VTE but also increases short-term mortality. Piazza et al. 37 reported that the odds ratios for in-hospital mortality and 30-day mortality among 1844 VTE patients with heart failure were 2.04 and 1.57, respectively.
Cancer is a strong risk factor for VTE, and approximately 20%–30% of patients with VTE have cancer. 38 In our study, 14% of the VTE group had cancer. Among the cancer patients, those undergoing surgery have a 2–3 times higher risk of developing VTE, and chemotherapy also increases the risk of VTE. 39 In this study, the risk of VTE was doubled when CO poisoning occurred in a patient with cancer. VTE in cancer patients increases mortality by two- to six-fold and should be monitored carefully. 40
Age is a well-known risk factor for VTE, and the risk of VTE doubles with every 10 additional years of age. 39 In this study, when the age increased by 1 year, the risk increased 1.01 times, and when the age increased by 10 years, the risk of VTE increased approximately 1.1 times, which is smaller than the previously reported 2 times. However, the CO poisoning patients included in this study were relatively young (median age = 44 years), and the risk is likely to be higher in relatively older groups. It is known that 60% of patients with VTE are 65 years of age or older, and mortality and morbidity due to VTE are higher in the older population. 41
Hypertension is a risk factor for atherosclerosis and VTE. In a meta-analysis, Mi et al. 42 reported that atherosclerosis risk factors such as hypertension, obesity, diabetes, smoking, and hyperlipidemia were also risk factors for VTE, and the odds ratio for VTE in patients with hypertension was 1.40. Recently, a new approach has been proposed, with VTE being classified as a panvascular syndrome, similar to coronary artery disease, peripheral artery disease, and cerebrovascular disease. 14 Although hypertension was not a risk factor for VTE or PE in this study, it did significantly increase the risk of DVT by 2.5 times.
This study has several limitations. First, clinical information such as initial consciousness, vital signs, immobilization, CO exposure time, cause of exposure, co-exposure, and laboratory data reflecting the severity of the CO poisoning could not be confirmed. In particular, clinical information on the reasons for ICU admissions could not be clearly identified. Second, it was not possible to confirm whether the health screening data, such as obesity, smoking, and alcohol consumption, were associated with the VTE risk. However, the underlying diseases and known thromboembolism risk factors were defined using diagnostic and treatment codes, and efforts were made to examine the various covariates related to VTE. Third, we were able to identify the start and end dates of hospitalization from the NHIS database; however, it was not possible to confirm the start and end dates of ICU admission. Most of the CO poisoning patients with ICU admissions would have been admitted at the beginning of their hospital stay. However, it is possible that some patients were admitted to the ICU after being diagnosed with VTE.
Conclusion
Patients with older age, ICU admission, a longer length of stay, congestive heart failure, or cancer are at greater risk of developing VTE after CO poisoning. In particular, ICU admission was the strongest risk factor for VTE, PE, and DVT. Monitoring and administering prophylactic treatments to prevent VTE would be helpful in high risk in CO poisoning patients.
Supplemental Material
sj-pdf-1-hkj-10.1177_1024907921994426 – Supplemental material for Risk factors for venous thromboembolism after carbon monoxide poisoning: A nationwide population-based study
Supplemental material, sj-pdf-1-hkj-10.1177_1024907921994426 for Risk factors for venous thromboembolism after carbon monoxide poisoning: A nationwide population-based study by Yongil Cho, Tae Ho Lim, Byuk Sung Ko, Hyunggoo Kang, Jaehoon Oh and Heekyung Lee in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
This study employed the National Health Insurance Service database (NHIS-2018-1-195). The interpretations and conclusions reported here do not represent those of the NHIS.
Author contributions
Y.C. and T.H.L. were responsible for the conception and design of the study. Y.C. and B.S.K. were involved in data analysis. Y.C. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
National Health Insurance Service (NHIS) data are third-party data that are not owned by the authors. The raw data can be accessed with permission from the NHIS in Korea.
Ethical approval and informed consent
The institutional review board of Hanyang University Hospital in Korea approved this work (IRB No. HYUH 2018-04-032), and the requirement for informed consent was waived for this retrospective study.
Human rights
All the procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.