
Abstract
Background:
The incidence of maternal cardiac arrest is rising in recent years. Medical staff generally lack the experience of performing resuscitation on pregnant patients. Maternal cardiac arrest and perimortem caesarean section simulation training was newly introduced in the Advanced Life Support in Obstetrics provider courses in Hong Kong since April 2021.
Objective:
To evaluate the course participants’ opinions on maternal cardiac arrest simulation training.
Methods:
A questionnaire survey was conducted for all participants in the Advanced Life Support in Obstetrics provider course in April 2021 to assess their opinions on the usefulness of this training.
Results:
There were four Advanced Life Support in Obstetrics provider courses in April 2021 with 36 participants in each course, and 137 questionnaires were received at the end of the course. The response rate was 137/144 (95.1%). After excluding the questionnaires with incomplete information, 134 questionnaires were included for final analysis. Almost all of the participants agreed that the maternal cardiac arrest simulation training could help them in their work (97.8%), could improve their knowledge and skill (98.5%) and could improve team training and co-ordination (97.0%). The majority of them (97.0%) felt more confident in managing maternal cardiac arrest after the training, and 97.8% of participants felt that the perimortem caesarean section model was useful for training. Around 80% of the participants would recommend this course to their colleagues. There were no significant differences in opinions on the usefulness of this training among participants with regard to their specialty, whether they were doctors or nurses, their years of experience and the specific hospital settings.
Conclusions:
Maternal cardiac arrest simulation training was highly valued by all levels of obstetric, emergency medicine and anaesthesia staff in both public and private hospitals.
Introduction
The incidence of maternal cardiac arrest is around 2.8 to 3.6 per 100,000 pregnancies.1,2 The incidence has increased from 1 in 30,000 pregnancies in 2002 to 1 in 20,000 pregnancies in 2005 in United Kingdom. The rise in incidence was attributed to an increase in women with advanced maternal age, and thus a higher incidence of major obstetric complications and pre-existing maternal medical conditions such as hypertension and cardiac diseases. 3 Perimortem caesarean section (PMCS) should be initiated within 4 min after maternal cardiac arrest without return of spontaneous circulation for women ⩾20 weeks of gestation to relieve the aortocaval compression from the gravid uterus, allowing an increase in maternal venous return and cardiac output, as well as a decrease in oxygen demand and improvement in pulmonary mechanics. 4
A review on all PMCS published in the literature from 1985 to 2004 included a total of 38 PMCS cases, in which 34 foetuses survived and 13 of 20 mothers with reversible causes survived to time of discharge from hospital. Although there might be selection bias towards reporting successful PMCS cases in the literature, there was no evidence of maternal deterioration after PMCS. 5 Another review on all PMCS performed in the period 1980–2010 found the maternal survival rate was 54.3% (51/94). Neonatal survival and neurologic outcome were directly related to the time between maternal death and baby delivery. Therefore, in-hospital cardiac arrest is significantly associated with better maternal and neonatal survival compared with pre-hospital cardiac arrest. 6 PMCS is now considered as a legitimate medical intervention during resuscitation of maternal cardiac arrest to improve the maternal and neonatal survival. Two cases of pre-hospital maternal cardiac arrest treated with PMCS in the accident and emergency department (AED) in Hong Kong have been formally reported in the literature in 1994 and 2018 with PMCS performed 30 and 14 min on arrival to AED, respectively,7,8 although the actual number of PMCS performed in AED or in the obstetrics wards in Hong Kong over the past decades far exceeded these two published reports. From the two reported cases, we can observe that there is room for improvement in shortening the time to arrange for PMCS.
Maternal cardiac arrest is a high-risk, low-frequency scenario, and medical staff generally lack the experience of performing resuscitation on pregnant patients. However, applying left uterine displacement and promptly performing PMCS with ongoing effective maternal cardiopulmonary resuscitation is the key to improve maternal and neonatal outcomes. 9 Therefore, practical training in maternal resuscitation and PMCS is crucial to both obstetrics and AED staff, and thus it has been included in the curriculum of many obstetric emergency training courses. 10
Maternal cardiac arrest and PMCS simulation training was newly introduced in the Advanced Life Support in Obstetrics (ALSO) provider course in Hong Kong since April 2021. The objective of this study is to evaluate the course participants’ opinions on maternal cardiac arrest simulation training in the form of a questionnaire survey.
Methods
The ALSO Provider Course is an educational programme designed for maternity care professionals including obstetric doctors, emergency physicians, midwives, nurses and other healthcare providers that may encounter maternal cardiac arrest to enhance their knowledge and procedural skills of managing obstetrical emergencies. It consists of required syllabus reading, lectures and hands-on workshops. Traditionally, the knowledge of resuscitation in maternal cardiac arrest in the ALSO provider course was delivered in a lecture. The participants will then practice cardiac pulmonary resuscitation skills individually on a manikin model in small groups during the practical workshops.
Maternal cardiac arrest and PMCS simulation training was newly introduced in the ALSO provider course in Hong Kong in April 2021 to enhance the skills and teamwork training of the medical staff. The knowledge and required skills in maternal resuscitation and PMCS was first delivered in a lecture, then followed by a maternal cardiac arrest and PMCS simulation training. The simulation scenario was a pregnant woman of gestation 38 weeks admitted to AED complaining of headache. She then developed cardiac arrest in AED while waiting for clinical assessment. The participants worked as a multi-disciplinary team with role-playing as emergency physicians, obstetricians, paediatricians and anaesthetists. Left uterine displacement, cardiopulmonary resuscitation, airway maintenance and intubation, defibrillation of shockable cardiac rhythm, administration of appropriate essential medication, performing PMCS after 4 min of cardiac arrest, investigating the underlying cause for the cardiac arrest and transferring the patient to the operation theatre to repair the uterine and skin wound after return of spontaneous circulation were performed. A simple and inexpensive manikin model was used for PMCS during the simulation. Video clips demonstrating how the manikin model was made and how PMCS could be simulated using this model have previously been published in the Hong Kong Journal of Gynaecology, Obstetrics and Midwifery 11 (available online at https://www.hkjgom.org/sites/default/files/pdf/v20n2-75-maternal-video1.mp4 and https://www.hkjgom.org/sites/default/files/pdf/v20n2-75-maternal-video2.mp4). After the simulation training, each participant will practice individual skills on basic life support on a manikin model with focus on pregnancy-related modifications in the form of small group workshops.
The PMCS simulation training was carried out in four ALSO provider courses, each with 36 participants, in April 2021. A questionnaire survey (Appendix 1) was conducted for all participants to assess their opinions on the usefulness of this maternal cardiac arrest and PMCS simulation training at the end of the course for improvement in future ALSO provider courses. This study was approved by the Kowloon Central/ Kowloon East Cluster Research Ethics Committee, Hospital Authority (Ref: KCC/KEC-2021-0136) and individual consent was waived by the ethics committee. The Statistical Package for Social Sciences for Windows package version 20 was used for data entry and analysis. Descriptive categorical data were expressed as numbers and percentages, and compared and analysed by chi-square test or Fisher’s exact test where appropriate. A p-value of <0.05 is considered statistically significant.
Results
There were a total of 144 participants in the four ALSO provider courses, and 137 questionnaires were received at the end of the course. Three questionnaires were excluded due to incomplete entries of important information, so that 134 questionnaires (93.1%) were included in the final analyses. Within this cohort, 67 (50.0%) participants were from AED, 66 (49.3%) were from Obstetrics and Gynaecology (O&G) departments and 1 (0.7%) was from Anaesthesiology. There were 35 (26.1%) doctors and 99 (73.9%) midwives and nurses, among which 59.7% of participants had less than 5 years of experience working in their current specialty, 14.9% of participants had encountered maternal cardiac arrest before in their clinical work, while 61.2% participants had not taken part in any maternal cardiac arrest simulation training before the ALSO course. The characteristics of the participants were shown in Table 1.
Characteristics of participants in the ALSO provider course in 2021.
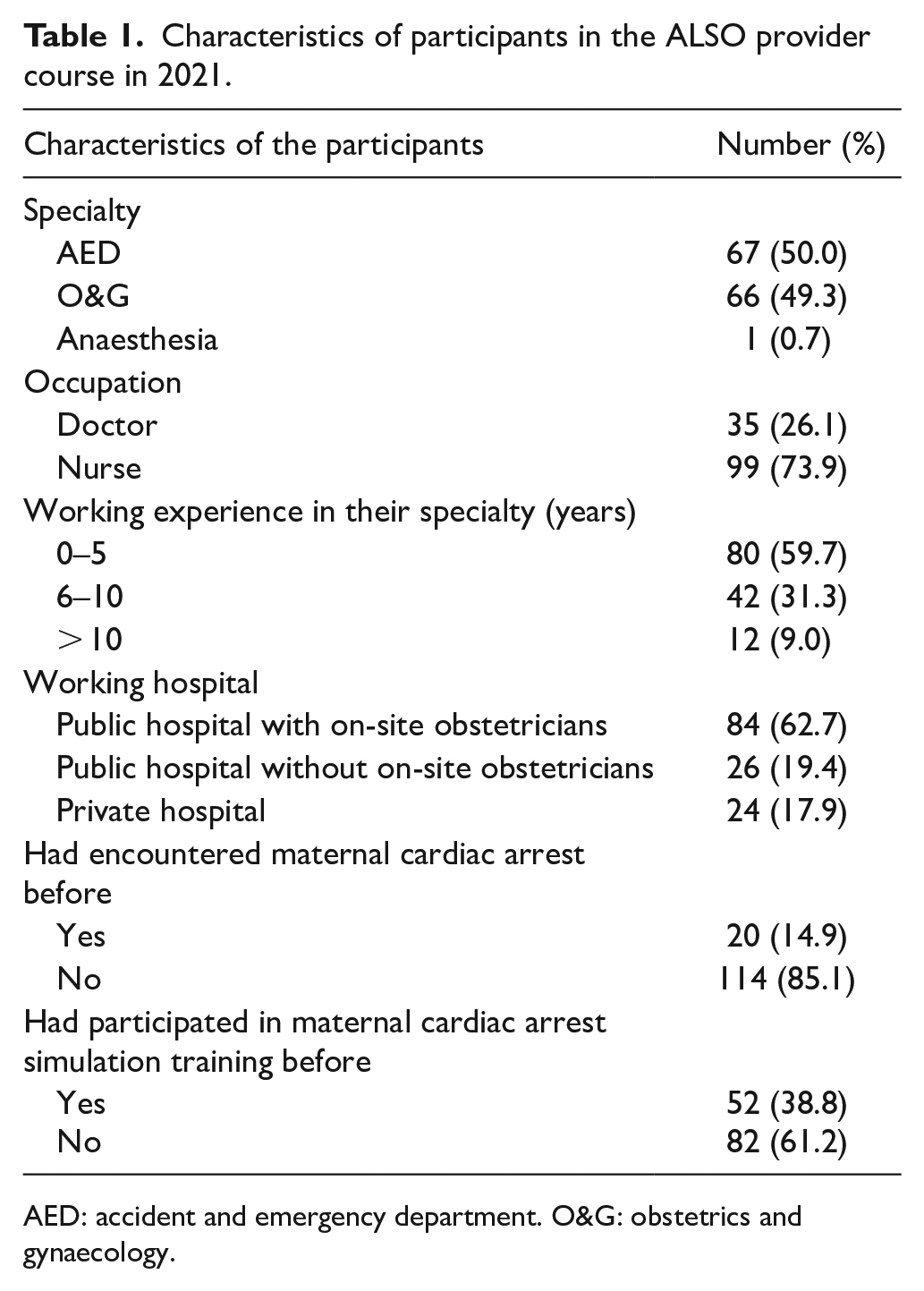
AED: accident and emergency department. O&G: obstetrics and gynaecology.
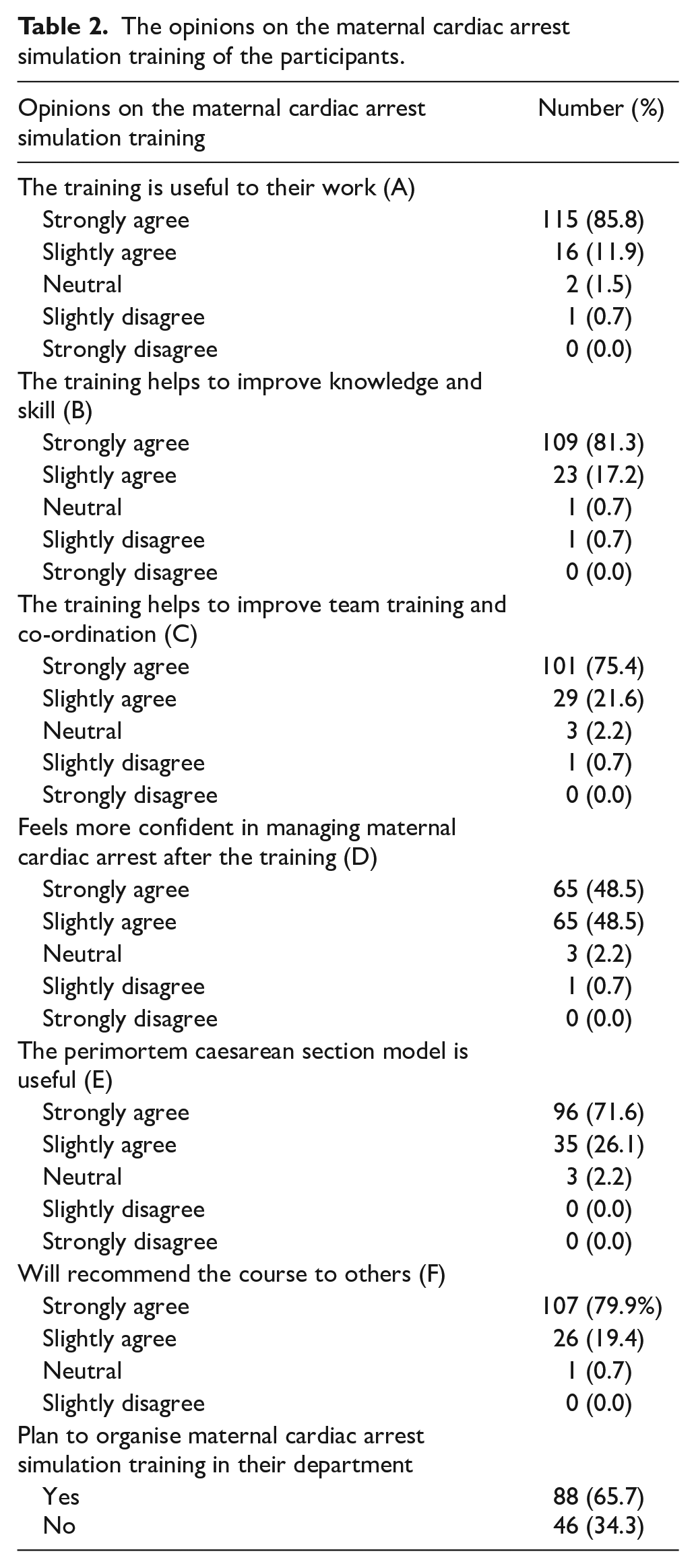
Overall, the maternal cardiac arrest simulation training was appreciated by a great majority of the participants. Almost all of the participants agreed (both strongly agreed or agreed were included) that the maternal cardiac arrest training could help them in their work (97.8%), could improve their knowledge and skill (98.5%) and could improve team training and co-ordination (97.0%). The majority of them (97.0%) felt more confident in managing maternal cardiac arrest after the training, and 97.8% of participants felt that the PMCS model was useful for training. Around 80% of the participants would recommend this course to their colleagues (Table 2).
The opinions on the maternal cardiac arrest simulation training of the participants.
The participants’ various characteristics were then evaluated to see whether there was any impact on their opinions on the maternal cardiac arrest simulation training. Overall, there were no statistically significant differences in opinions on the usefulness of the maternal cardiac arrest training between those working in AED or O&G streams, between doctors and nurses, between the staff with different years of working experience, between AED staff with on-site obstetricians support and those without on-site support, or between midwives working in public and private hospitals (Table 3).
Participants’ characteristics that may affect their opinions on maternal cardiac arrest simulation training.
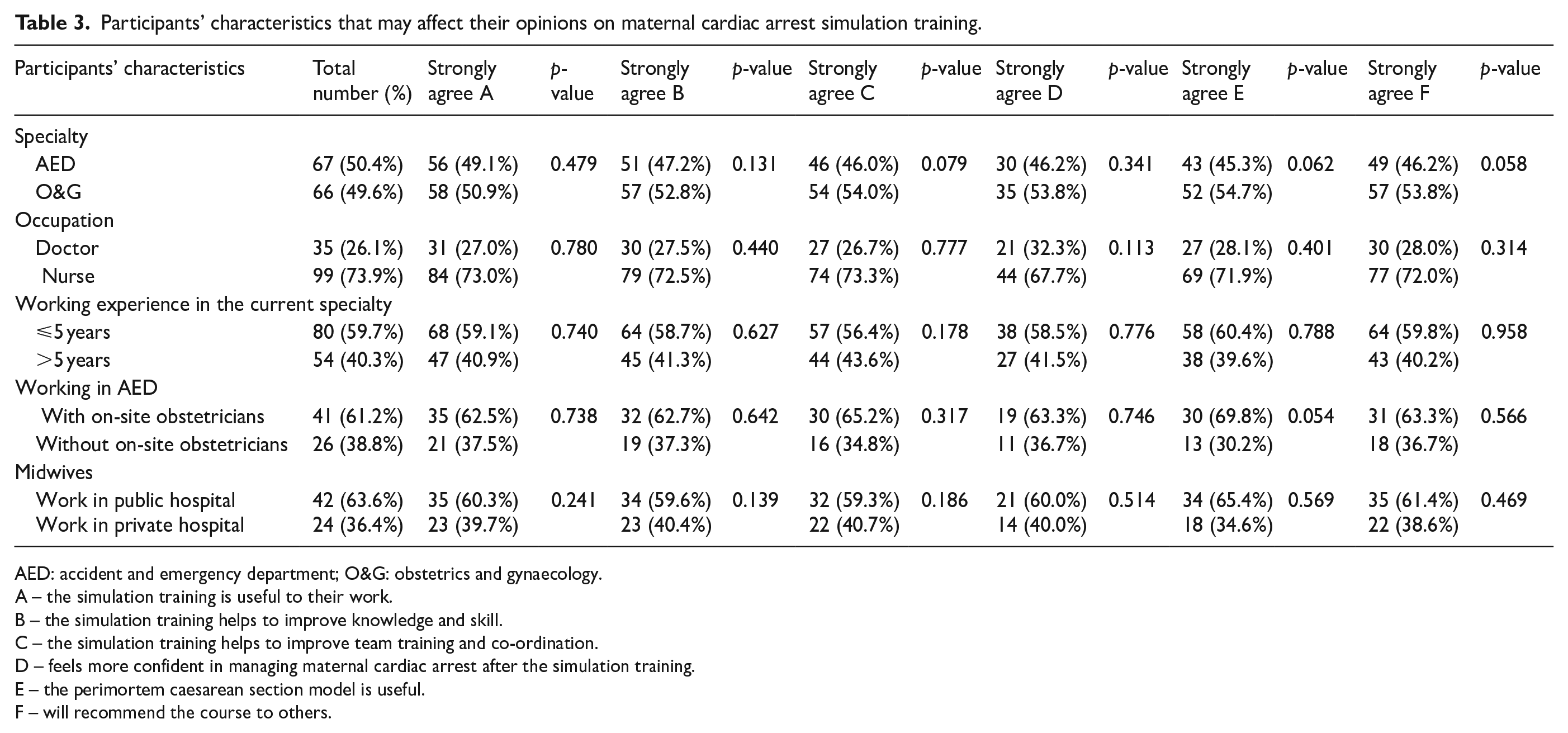
AED: accident and emergency department; O&G: obstetrics and gynaecology.
A – the simulation training is useful to their work.
B – the simulation training helps to improve knowledge and skill.
C – the simulation training helps to improve team training and co-ordination.
D – feels more confident in managing maternal cardiac arrest after the simulation training.
E – the perimortem caesarean section model is useful.
F – will recommend the course to others.
Discussion
Our questionnaire survey showed that the maternal cardiac arrest simulation training was highly evaluated by all groups of participants in the ALSO provider course, irrespective of their specialty, the types of staff, their years of experience and in which hospital settings.
A study had demonstrated similar positive staff feedback on the usefulness of the maternal cardiac arrest simulation training with increased confidence in managing this condition after the simulation training from a group of O&G doctors and nurses. 12 Another study showed improved knowledge, confidence and competence in management of maternal cardiac arrest on a group of O&G resident trainees when comparing their pre- and post-individual knowledge tests and surveys after simulation training. 13 Fisher et al. had investigated the usefulness of maternal cardiac arrest training on Maternal-Foetal Medicine staff by conducting pre-intervention, intervention and post-intervention evaluative simulations. The post-intervention scores showed significant improvement in initiating cardiopulmonary resuscitation and PMCS after maternal cardiac arrest. 3 Advanced cardiac life support (ACLS) training is required in medical specialties and in emergency medicine. However, ACLS is not a compulsory training for O&G doctors and nurses. The combination of inadequate training and rare exposure to cardiac arrest could result in a lack of confidence in initiating maternal resuscitation or PMCS in time. As around half of the participants in the ALSO provider course were from O&G speciality, individual skills training in basic life support was therefore also included in the ALSO course in the form of small group workshops.
Apart from O&G staff, our study showed that the maternal cardiac arrest simulation training was also highly evaluated by the AED staff. The review article on the PMCS from 1980 to 2010 showed that 28.7% of maternal cardiac arrest was pre-hospital arrest, with trauma accounting for 20.2% of all the causes. 6 Therefore, AED staff should also be equipped with skill and knowledge in managing maternal cardiac arrest. ACLS courses, in general, have not addressed interventions specific to obstetric patients, and significant knowledge gaps have been shown in healthcare providers.14–16 Cohen et al. 17 have shown that important knowledge of the need of left uterine displacement and the benefit of early resuscitative hysterotomy was inadequate in obstetricians, anaesthetists and emergency physicians. The Society for Obstetric Anesthesia and Perinatology had issued a consensus statement in 2014, which provided critical information including point-of-care checklists and operational strategies relevant to maternal cardiac arrest. 18 The American Heart Association had published its first scientific statement on maternal cardiac arrest in 2015 with up-to-date information for maternal resuscitation and has recommended periodic multidisciplinary drills and specific courses on maternal resuscitation. 19 The Managing Obstetric Emergencies and Trauma (MOET) course, which included education on PMCS, was introduced in the Netherlands in 2003. A study assessed the PMCS incidence in the 11 years before and the 5 years after introduction of the MOET course. PMCS was more likely to be performed after MOET course (four PMCS in 11 years (0.36/year) preceding MOET course versus eight in 5 years (1.6/year) after MOET course, p = 0.01). 10 McDonnell 20 and Vencken et al. 21 had reported successful outcomes in three PMCS performed and they attributed the success to the usefulness of maternal cardiac arrest simulation training. Despite the rare occurrence of maternal cardiac arrest, to our surprise, 14.9% of the ALSO course participants reported that they had encountered real maternal cardiac arrest events before. However, more than half of the total participants (61.2%) had never taken part in maternal cardiac arrest simulation training before attending the ALSO courses. This could reflect that maternal cardiac arrest may not be a very rare event in local clinical practice, and that many of our ALSO participants were eager to update their knowledge on maternal resuscitation after experiencing these events. With the documented usefulness of maternal resuscitation and PMCS simulation training from the literature, and the positive feedback from the participants in the ALSO courses this year, the ALSO (Hong Kong) Board has recently resolved that such simulation training on maternal cardiac arrest and PMCS will be continued in ALSO provider courses in Hong Kong in the coming years.
High-fidelity expensive simulator manikins had been used in the above-reported studies on maternal cardiac arrest simulation training.3,12 Training equipment is found to be the most expensive component of emergency obstetric care training 22 so that many emergency obstetric courses have not specifically included such simulation training as part of their essential curriculum. We have developed a simple inexpensive manikin model for PMCS, which highly mimics human anatomy. 11 This model had helped to test out many real-life conditions. The optimal positions for various personnel participating in the PMCS around the bed could be practised. The splash of liquor on the floor after PMCS would alert the participants to the risk of electric shock injury to participating staff when continuing to perform cardiac defibrillation and, therefore, the need to stay away from the wet floor and to maintain a dry floor surface with towels or blankets after PMCS as much as possible. The latter manoeuvre, indeed, would also go a long way to prevent slip and fall accidents for staff during maternal resuscitation. About 97.8% of the ALSO participants opined that this PMCS model was useful for their training. Encouragingly, almost two-thirds of the participants expressed that their departments were planning to organise maternal cardiac arrest simulation training. We believe that developing an inexpensive and easily available PMCS model will be most valuable for promoting maternal resuscitation simulation training. It had been suggested that the frequency of training every 2 years is not sufficient for mastery of maternal cardiopulmonary resuscitative skills, 15 and healthcare professionals tend to lose their technical expertise when their exposure to such an event was so infrequent. 23 Therefore, we suggest all relevant staff should have the opportunity to participate in maternal cardiac arrest simulation training at least on a yearly basis in their own departments, after their first exposure to such maternal cardiac arrest training in formal courses such as the ALSO. Since three-fifth of the ALSO participants (61.2%) did not have any of the maternal cardiac arrest simulation training before, there is certainly room for improvement in maternal resuscitation training, not only by offering more simulation training in formal courses, but also in organizing similar training in individual O&G and AED units to allow more staff to have the exposure. Training professionals, helping patients and saving lives is an important mission of clinical simulation. 24
Limitation of the study
The main limitation is that the ALSO participants were from different hospitals and departments. The simulation training in the ALSO course cannot help to identify unit-specific system and equipment issues. Therefore, we still recommend each unit to organise regular simulation training to identify deficient areas in protocols, systems and settings in individual clinical units, and to enhance communication between various disciplines and specialties in their hospital, even if their staff had attended similar simulation training in obstetric courses before.
Another limitation of this study is that this questionnaire survey only investigated the feedback from the staff while the effectiveness of the simulation training on managing a real cardiac arrest cannot be demonstrated due to the very low incidence of such acute life events. A pre- and post-training performance scoring system of the participants can be considered in future ALSO courses to objectively document their enhancement in knowledge and competence after simulation training. A web-based pre- and post-course scenario multiple choice questionnaire (MCQ) may help to enhance the course effectiveness with quantitative assessment.
Conclusion
Maternal cardiac arrest and PMCS simulation training in the ALSO course was highly valued by all levels of O&G and AED staff participants in both public and private hospitals. The training was evaluated by the opinion survey as being useful to their work, helps to improve knowledge and skills, as well as team training and co-ordination. We recommend that such simulation training should be regularly organised in O&G department and AED. Future study to evaluate whether the behavioural changes would improve patient outcome is required.
Research Data
sj-sav-1-hkj-10.1177_10249079211072403 – for Impact of foeto-maternal resuscitation and perimortem caesarean section simulation training: An opinion survey of healthcare participants
sj-sav-1-hkj-10.1177_10249079211072403 for Impact of foeto-maternal resuscitation and perimortem caesarean section simulation training: An opinion survey of healthcare participants by Choi Wah Kong and William Wing Kee To in Hong Kong Journal of Emergency Medicine
Footnotes
Appendix 1
Opinions on maternal cardiac arrest and perimortem caesarean section simulation training
Author contributions
C.W.K. is responsible in concept and design of the study, acquisition of data, analysis and interpretation of the data, and drafting of the manuscript. W.W.K.T. is responsible for analysis and interpretation of the data and critical revision for important intellectual content. All authors had full access to the data, contributed to the study, approved the final version for publication and take responsibility for its accuracy and integrity.
Availability of data and materials
The data file is attached in the supplementary file.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Individual consent was waived by the research ethics committee.
Ethical approval
This study was approved by the Kowloon Central/ Kowloon East Cluster Research Ethics Committee (Ref: KCC/KEC-2021-0136)
Human rights statement
This study conforms to the ethical guidelines of the 1975 Declaration of Helsinki
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.