
Abstract
Objective:
To compare local poisoning patterns of preadolescents and adolescents.
Methods:
Retrospective cross-sectional study. Data collected through the Hong Kong Poison Information Centre (HKPIC) Poisoning Information and Clinical Management System (PICMS). Patients aged 10 to 17 years old from January 2016 to December 2018 were included and divided into preadolescent (10–12 years old) and adolescent (13–17 years old) groups. Statistical analysis for categorical variables was performed using chi-square test of independence, p < 0.05. Strength of association examined with Cramer’s V. Rate ratios with 95% confidence interval were used to determine nature of association, using preadolescents as comparison group.
Results:
A total of 703 cases were analyzed. There were 107 cases in the preadolescent group and 596 cases in the adolescent group. Three variables showed moderate association: intentional exposure (rate ratio: 2.91, 2.13–3.98), exposure in school (rate ratio: 0.30, 0.21–0.44), and the use of pharmaceuticals (rate ratio: 1.95, 1.57–2.44). The most common substance of exposure were analgesics (n = 213, 24.94%) and fumes, gases, and vapors (n = 19, 15.08%) in adolescents and preadolescents, respectively.
Conclusion:
Epidemiological difference still exists between preadolescents and adolescents. The association of adolescents with intentional poisoning, and the use of pharmaceuticals was highlighted. The study acts as a recent update of pediatric poisoning patterns and hopes to act as a reference for future studies.
Introduction
Pediatric poisoning has long been a major concern worldwide as it represents a potentially preventable population group. Hong Kong has a growing population with 7.48 million people at the end of 2018 with age groups 0–19 making up 15.4% of the total population at the time. 1 In the past, a few epidemiological studies describing the local pediatric poisoning pattern have been done.2–6 From 1985 to 1994, 2% and 22% of poisoning patients were in the age groups 1–10 years and 11–20 years, respectively. 6 From 2005 to 2008, overall trends showed adolescent girls ingesting medications as a gesture of suicide, while younger children are more likely to have accidental poisoning.2,5 A bimodal distribution with the first peak at 1–3 years old and the second peak at 15–17 years old was noted with female predominance in the older children in overall poisoning cases. These trends were also reproducible in overseas studies.7–10
The American Academy of Pediatrics (2019) defines stages of adolescence into early adolescence or preadolescence (ages 10–13), middle adolescence (ages 14–17) and late adolescence (ages 18–21). From the age of 10, children undergo rapid growth with many physical, sexual, cognitive, social, and emotional changes. These changes extend onward past the ages of 14, with further development of abstract thinking and sense of identity. In the recent decade, overseas centers have observed a pattern shift, with a more frequent occurrence of intentional poisoning starting from an earlier than expected onset age, as young as 8 years 10 and 10 years onwards. 7 A spiked increase from 13 years onwards7,9 was observed. Overall poisoning incidence in the preadolescent and adolescent groups showed year-on-year dramatic increase since 2010.7,10 Unpublished local data also showed a spike in intentional poisoning incidence since 2017 in children older than 10 years of age. These observations raise the question: is there still a difference in epidemiological pattern between preadolescents and adolescents?
The study’s main objective is to identify and confirm whether there is still an epidemiological difference between preadolescent and adolescent poisoning locally. For this study, we have chosen to compare the groups aged 10–12 and aged 13–17, labeled as preadolescents and adolescents for ease of presentation. This was based on two main considerations: (1) to set two groups that are relatively comparable in terms of physical and cognitive development as opposed to even younger groups; (2) adjust the cut off age considering local culture trends and education schedules. In the local education system, majority of 13-year olds would have started secondary school education, which marks a significant change in social and educational environment.
The study hopes to provide updated insight to healthcare providers and educators which may facilitate strategies in local poisoning prevention and to act as a reference for future epidemiological studies.
Methods
Study design
The HKPIC receives consultations concerning poisoning from all health care professionals in Hong Kong, including public hospitals, private hospitals, and clinics. Poisoning cases managed in Emergency Departments of public hospitals are also voluntarily reported to the HKPIC. A retrospective cross-sectional study was designed, using the HKPIC PICMS database of consultations and reports between the period of January 2016 to December 2018. All poisoning cases that involved patients from 10 to 17 years of age were recruited. Duplicate records, cases with outcome relation coded as “not related” or “not applicable,” and cases with incomplete data were excluded from statistical analysis.
Composite age groups of preadolescents (10–12 years old) and adolescents (13–17 years old) were created for comparison. Primary objective of this study is to identify the epidemiological difference between preadolescent and adolescent poisoning patients, examining the variables: gender, reason of exposure, outcome severity, exposure in a residence, exposure in school, and use of pharmaceuticals. The secondary objective of the study was to perform a descriptive analysis related to all exposed poisons and mortality.
Sample size was estimated using n = (Z2 P(1−P))/d2, assuming a 95% confidence interval and using data regarding gender proportions from previous studies. From Yip’s study, 2 72% of adolescent poisoning patients were female. The estimated sample size required was just over 300.
Definitions
Poisoning reports and consultation were coded within the PICMS according to definitions adopted from 2009 Annual Report of the American Association of Poison Control Centers’ National Poison Data System.
Regarding reason of exposure, intentional poisoning included cases coded as “abuse,” “malicious poisoning,” “misuse/others—intentional” and “suspected self-harm.”
Unintentional poisoning included cases coded as “adverse herb/PCM reaction,” “adverse pharmaceutical reaction,” “bite/sting,” “food poisoning,” “general unintentional,” “others—unintentional,” and “therapeutic error.”
Outcome severities were differentiated as (1) no effect, (2) minor effect with minimally bothersome and rapidly resolved signs or symptoms, (3) moderate effect with signs or symptoms that were more pronounced, prolonged, or systemic in nature than minor symptoms, where treatment is often indicated, (4) major effect with signs or symptoms that were life-threatening or resulted in significant residual disability or disfigurement, (5) death. For the purposes of analysis, “no effect” and “minor effect” cases were grouped as one category labeled “mild outcome.” Cases coded as “moderate effect,” “major effect” and “death” were grouped and labeled as “serious outcome.”
Pharmaceuticals included analgesics, anticholinergics, anticonvulsants, antidepressants, antihistamines, antimicrobials, antineoplastics, antipsychotics, cardiovascular drugs, cold and cough preparations, dietary supplements and herbals, electrolytes and mineral, gastrointestinal drugs, hormones, hypoglycemic agents, opioids, respiratory drugs, sedatives and hypnotics, slimming products, stimulants and street drugs, and vitamins. Non-pharmaceuticals included alcohol; bites and envenomations; Chinese herbal medicine; proprietary Chinese medicine; cosmetics and personal care products; fumes, gases, and vapor; homeopathic agents; household products; industrial products; metals, pesticides, and toxins in food; and miscellaneous agents.
Statistical method
Descriptive statistics and summary statistics were analyzed and reported. Age groups and categorical variables were cross-tabulated and analyzed using Pearson’s chi-square test of independence (p < 0.05). Cramer’s V was used as an effect size measurement to determine the strength of statistically significant variables, with 0 corresponding to no association and 1 corresponding to complete association. Ranges of strength were taken as 0–0.2, >0.2 to 0.6, and >0.6 corresponding with weak, moderate, and strong associations, respectively.
Incidence rates of being female, having intentional poisoning, having serious outcome, exposure at residence, exposure at school, and pharmaceutical use in each group were calculated. Rate ratios (95% confidence interval (CI)) of adolescents over preadolescents were calculated to further determine natures of association for variables.
Data were tabulated in Microsoft Excel and statistical analysis was performed using Statistical Package for the Social Sciences (SPSS).
Written informed consent was not necessary for the following quoted original paper because no patient data have been included in the manuscript. The study was approved by the Kowloon Central / Kowloon East Research Ethics Committee.
Results
A total of 1548 cases were identified, of which 843 cases were excluded from analysis due to duplicate records and outcome relation coded as “non-related” or “not applicable.” two more cases were excluded due to incomplete data. A total of 703 cases were included in statistical analysis (Figure 1). Figure 2 shows the distribution of patients per years of age. Composite age groups were created, with 107 cases in the preadolescent group and 596 cases in the adolescent group. The median age for each group was 11 and 16, respectively. The associations of age groups with study variables are shown in Table 1 and rate ratios’ forest plot in Figure 3.
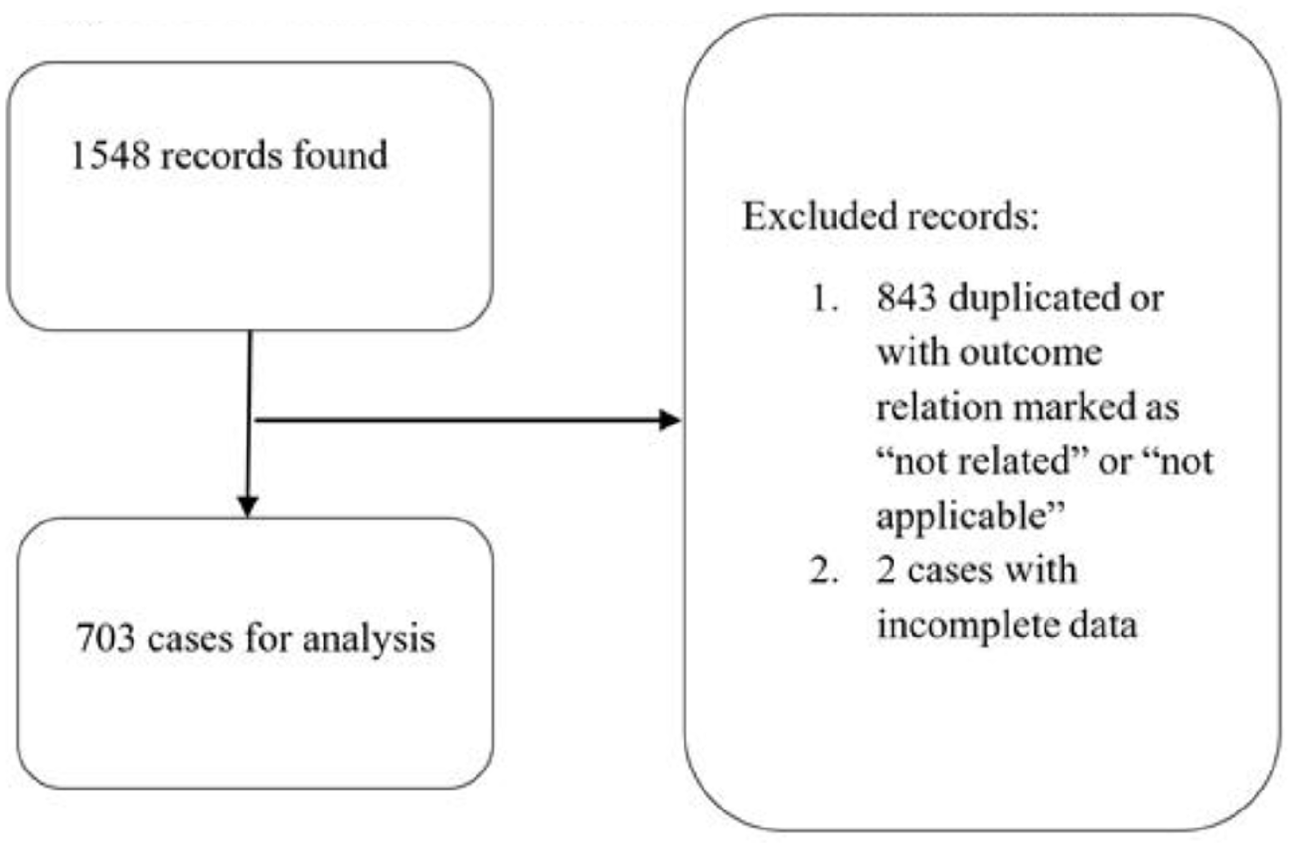
Flow chart of recruitment and exclusion of data for analysis.
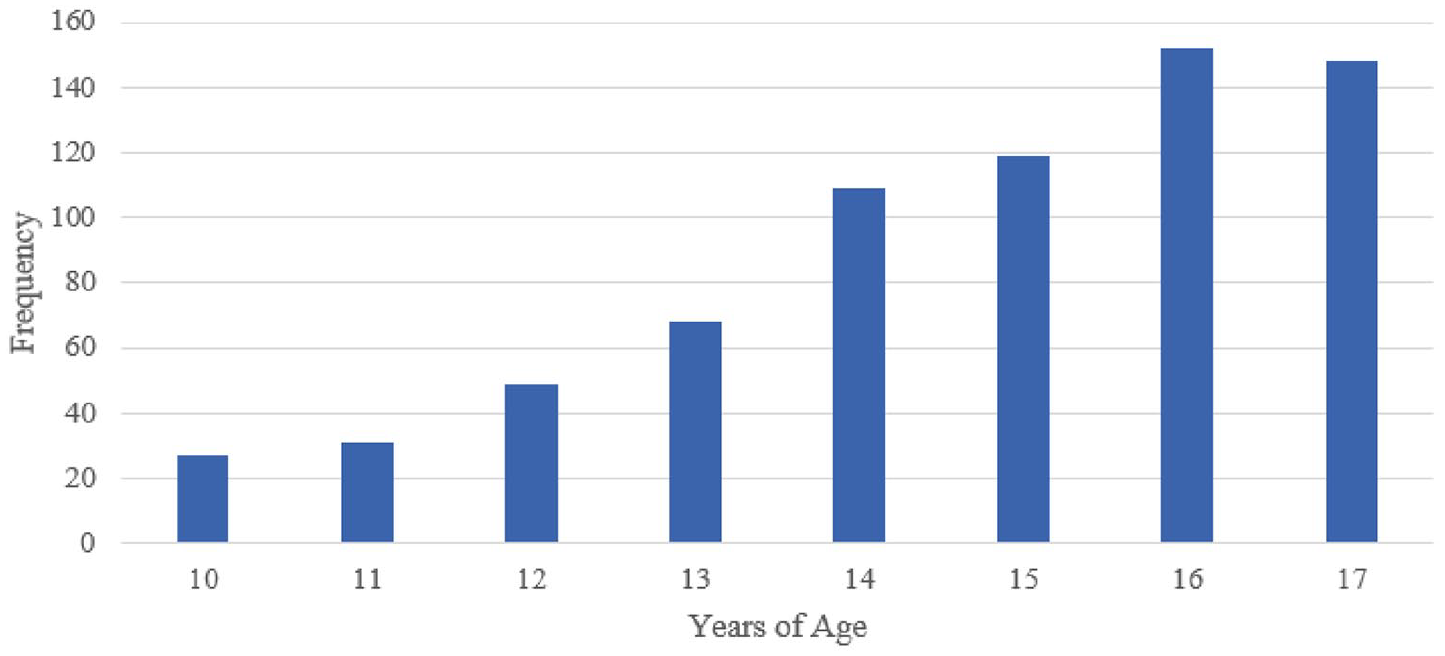
Patient distribution per years of age.
Association of variables with different age groups.
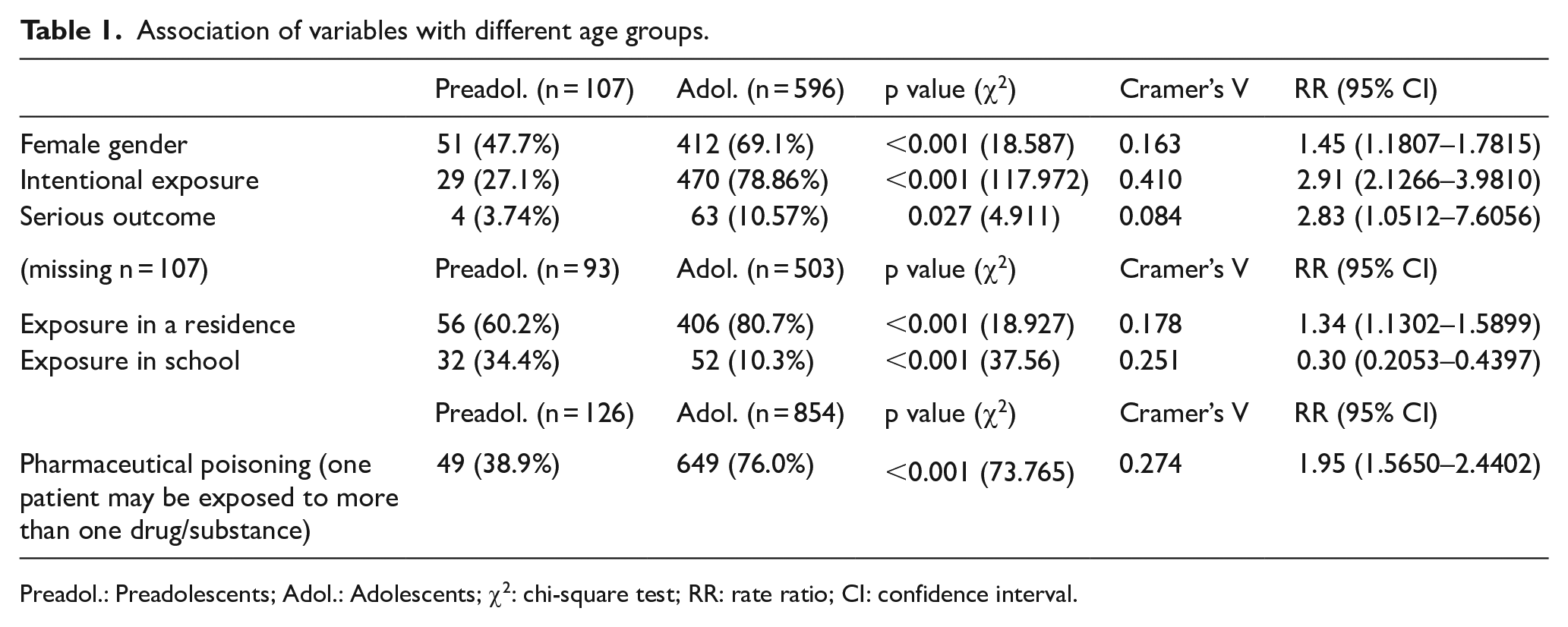
Preadol.: Preadolescents; Adol.: Adolescents; χ2: chi-square test; RR: rate ratio; CI: confidence interval.
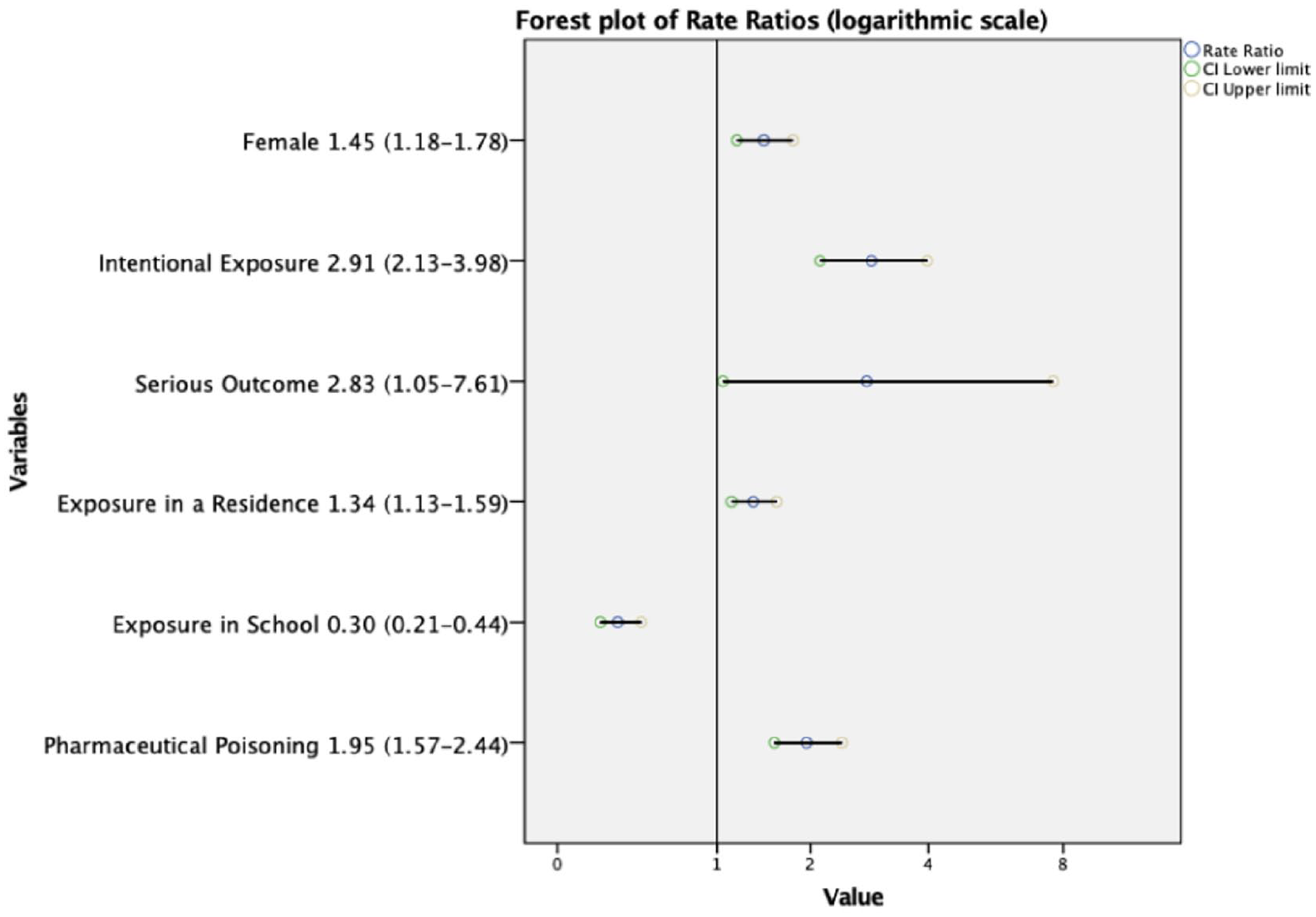
Forest plot of rate ratios (logarithmic scale).
Overall, although all study variables showed statistically significant association (Table 1), only three variables: reason of exposure, exposure in school, and use of pharmaceuticals showed moderate association and were considered of clinical relevance.
Age and gender
There was statistically significant correlation between age and gender (χ2 (1, n = 703) = 18.587, p < 0.001), but with weak strength of association (Cramer’s V = 0.163). Adolescents were 1.45 times more likely to be female than preadolescents (95% CI: 1.18–1.78). In clinical practice, there may not be a noticeable difference in gender predominance among the different age groups.
Age and reason of exposure
Reason of exposure was defined as intentional poisoning and unintentional poisoning. Age group and reason of exposure were moderately associated (χ2(1, n = 703) = 117.972, p < 0.001, Cramer’s V = 0.41). Adolescents had nearly three times more intentional exposure than preadolescents (95% CI: 2.13–3.98). This is one of the stronger associations found in this study and can confirm previous local2,5 and overseas observations.9,10
Age and outcome severity
For the purposes of analysis, outcome severity was grouped into mild outcome and serious outcome. Correlation between age group and outcome severity groups were statistically significant (χ2 (1, n = 703) = 4.911, p = 0.027). However, the strength of association was very weak (Cramer’s V = 0.084). The rates ratio was 2.83 (95% CI: 1.05–7.61). Use in clinical practice may be negligible.
Age and place of exposure
A total of 107 cases were excluded due to missing data for place of exposure. There were 93 cases in preadolescents and 503 cases in adolescents analyzed.
Exposure in a residence had statistically significant but weak association with age groups (χ2(1, n = 596) = 18.927, p < 0.001, Cramer’s V = 0.178). Adolescents had 1.34 times more exposures in a residence than preadolescents (95%CI: 1.13–1.59).
Exposure in school showed a moderate association with age (χ2(1, n = 596) = 37.56, p < 0.001, Cramer’s V = 0.251), where adolescents were only 0.3 times as likely to have exposures at school (95% CI: 0.21–1.44). This result may be influenced by a one-off school cluster contributing to 10 out of 93 preadolescent poison cases and 18 out of 503 adolescent cases occurring in school. This will be further elaborated in the discussion section.
Age and substance exposed
Substances involved were divided into pharmaceuticals and non-pharmaceuticals for analysis. There were 980 substances involved, where a single patient may have been exposed to more than one substance. There was a total of 126 substances used in preadolescents and 854 in adolescents. There was moderate association between age and pharmaceutical nature of substance (χ2 (1, n = 980) = 73.77, Cramer’s V = 0.274). Adolescents were almost twice as likely to use pharmaceutical agents than preadolescents (95% CI: 1.56–2.44).
In preadolescents, the three most encountered poison categories were fumes, gases, and vapors (n = 19, 15.08%); bites and envenomation (n = 18,14.29%); and household products (n = 12, 9.52%; Figure 4). There was a school cluster reported in March 2016 involving 28 cases exposed to gas leak, presumably tetrahydrothiophene. Ten cases were preadolescents, and 18 cases were adolescents. This explains the unexpected spike in cases exposed to fumes, gases, and vapors in preadolescents.
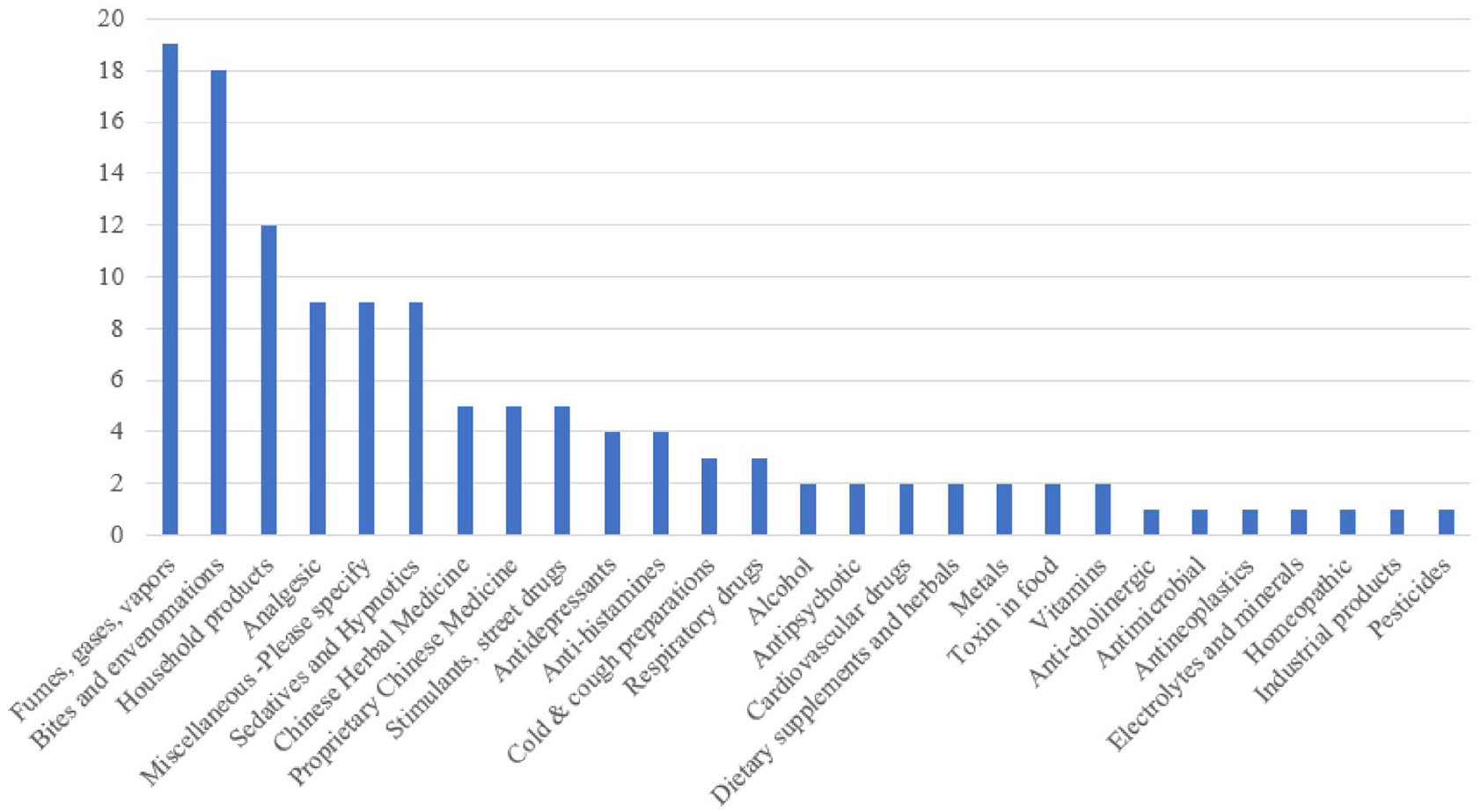
Poison exposure in preadolescents.
In adolescents, the three most encountered poison categories were all pharmaceuticals, including analgesics (n = 213, 24.94%), sedatives and hypnotics (n = 100, 11.71%), and antidepressants (n = 96, 11.24%; Figure 5).
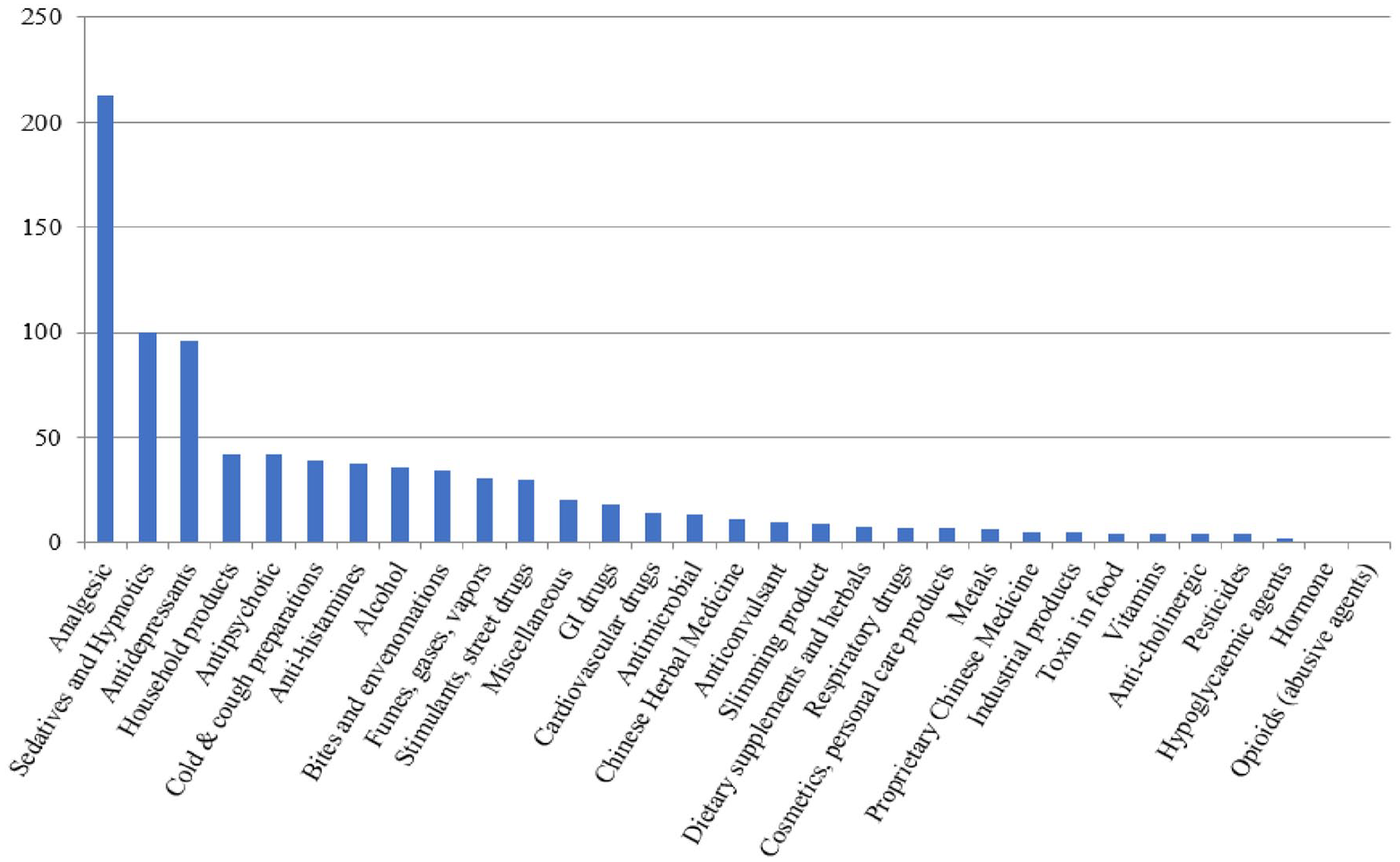
Poison exposure in adolescents.
Mortality
There were two cases of mortality in this study. Overall mortality rate in this study was 0.28%. A 15-year-old girl, with known history of depression, overdosed on paracetamol, promethazine, and fluoxetine as an act of self-harm. She presented with a cut wrist wound and emotional outburst. She was admitted to the pediatric intensive care unit and later developed agitation, status epilepticus, and refractory hemodynamic compromise. Despite best medical treatment, she rapidly deteriorated and succumbed on Day 3 of admission. Another case involved a 16-year-old girl with known history of dysthymia and depression. She was found in cardiac arrest after burning charcoal at home. She arrived at the Emergency Department with no detectable vitals and was certified dead.
Discussion
The study confirms that there is still an epidemiological difference between preadolescents and adolescents. The three most clinically relevant associations found were reason of exposure, exposure in school, and use of pharmaceuticals. Adolescents had three times more intentional exposure and two times more use of pharmaceuticals. Adolescents only had 0.3 times the incidence of poisoning in school than preadolescents.
When looking into the “exposure in school” variable, a school cluster of town gas exposures with 10 preadolescent cases and 18 adolescent cases were noted. If the statistical analysis were performed again after removing the school cluster, chi-square test was still statistically significant with p < 0.001; however, Cramer’s V would decrease to 0.23 and rate ratio was 0.26 (95% CI: 0.16–0.43). Thus, school as a location of exposure may have less clinical significance than the study suggests if the school cluster was removed.
Local experience observed a 72% female incidence in adolescent poisoning. 2 A similar 68.57% was observed in this study. However, age group and gender were found to be only weakly associated in the study’s older spectrum of pediatrics. These findings may provide insight to strategies in pediatric poisoning prevention.
There were two cases of mortality among the 703 cases studied over the 3-year period. Both cases were adolescents with psychiatric history, whom intentionally self-poisoned as an act of self-harm. This is in stark contrast to the zero-mortality rate among 1,208 emergency department cases reported in a Singapore study over a 5-year period. 9 Previous studies showed that although almost all intentional overdosed adolescents presenting to hospital survived, repetition was common, and 1 in 100 survivors would die by suicide within 7 years.11,12 The association between age group and prevalence of psychiatric illness was not studied. Speculations have been made that social media, online engagement, and smartphone usage have effects on mental health. Local figures on information and technology use 13 showed a sharp increase in ownership of a smartphone starting from the age of 10 onwards and gradual year-on-year increase in use of Internet since 2014. Local census data 14 noted an increase of smartphone ownership in the 10–14 age group from 46.1% in 2012 to 76.9% in 2015. The relationships of technology use, mental health, and pediatric poisoning pattern may represent a potential area of interest in future studies.
The top-3 substances involved in adolescents were analgesics, sedatives, and antidepressant. Common analgesics like paracetamol may be easily purchased over the counter. The number of psychiatric patients using the Hospital Authority services increased from 187,000 in 2011–2012 to over 226,000 in 2015–2016.15,16 There are expectedly more households stocking psychiatric prescription medications at home, thus contributing to the ease of accessibility of these drugs by adolescents.11,12 In the event of intentional poisoning, the youth may be ignorant of the potential late dire effects of pharmaceutical overdose. This may lead to tragic consequences even if initial intent was non-lethal and impulsive 10
Healthcare providers, educators, and family members should be aware of the increased tendency for adolescent’s intentional exposure to poison. Adolescents may potentially benefit from education on pharmaceuticals, risk assessment, access to stress-coping tools, and social support network. Prevention in preadolescents may require a greater emphasis on environmental and home safety.
The study is not without limitations. Cases incorporated into the database are from consultations and voluntary reporting. There may be an underestimation of cases who had minimal clinical effects because of poisoning. These patients may be readily managed at home or by the primary care physicians without initiating consultations. Effects of school cluster cases may not be reproducible at a different timeframe as they are expected to be one-off unique events. Being a cross-sectional retrospective study, causal relationship cannot be determined among variables and is unable to make any predictions of causal effects.
Conclusion
The study acts as a recent update of poisoning patterns in the more mature spectrum of pediatric patients, highlighting the association of adolescents with intentional poisoning and use of pharmaceuticals, which represent an important demographic that may benefit from targeted preventive measures. The study also hopes to act as a reference for studies looking at future changes in pediatric poisoning pattern, assessing the effects of city events occurring after this study period, for example, local social unrest involving Anti-extradition Law Amendment Bill Movement and the outbreak of the global COVID-19 pandemic.
Footnotes
Acknowledgements
The authors would like to thank Mr. M. H. Wong and the Hong Kong Poison Information Center for facilitating database access.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data were collected through the Hong Kong Poison Information Center (HKPIC) Poisoning Information and Clinical Management System (PICMS). Consultations and reports between the period of January 2016 to December 2018 involving ages 10–17 were included for the study.
Ethical approval and ethical number provided by the review board
The study was approved by the Kowloon Central/Kowloon East Research Ethics Committee (REC reference no. KC/KE-20-0341/ER-4).