
Abstract
Background:
Extracorporeal toxin removal is used for enhanced elimination in severe lithium poisoning. The Extracorporeal TReatments In Poisoning workgroup provides recommendations on the use of extracorporeal toxin removal in poisoning.
Objectives:
Our aim was to identify the pattern for using extracorporeal toxin removal in managing lithium poisoning in Hong Kong and compare the outcomes in extracorporeal toxin removal-treated patients and non-extracorporeal toxin removal-treated patients if indicated for treatment as defined by The Extracorporeal TReatments In Poisoning criteria.
Methods:
Lithium poisoning presented between year 2009 and 2019 in Hong Kong Poison Information Centre (HKPIC) database was categorized into extracorporeal toxin removal-treated group and non-extracorporeal toxin removal-treated group. Comparative analyses were performed.
Results:
Among 112 lithium-poisoned patients, 21% were treated with extracorporeal toxin removal. Larger proportion of patients had fulfilled at least one Extracorporeal TReatments In Poisoning criteria for extracorporeal toxin removal in the extracorporeal toxin removal-treated group (87% vs 18%, p < 0.005). The extracorporeal toxin removal-treat group patients were more commonly presented with impaired consciousness, seizure and dysrhythmia (p < 0.05). They also got higher admission (3.62 mmol/L vs 2.18 mmol/L, p < 0.05) and peak (4.15 mmol/L vs 2.28 mmol/L, p < 0.05) serum lithium concentrations, as well as a significantly higher serum creatinine concentration upon presentation (263.74 µmol/L vs 98.66 µmol/L, p < 0.05). Extracorporeal toxin removal-treat group patients more frequently had a severe poisoning outcome (91.3% vs 9%, p < 0.05) and developed complications (69.6% vs 13.5%, p < 0.05). Logistic regression identified seizure, peak serum lithium concentration, and serum creatinine concentration upon presentation as risk factors for severe poisoning outcome. In subgroup analysis on patients with at least one indication for extracorporeal toxin removal as defined by Extracorporeal TReatments In Poisoning criteria, the proportion of severe poisoning remained higher in the extracorporeal toxin removal-treated group (90% vs 43.7%, p < 0.05). Complication rate was not significantly different between the two groups.
Conclusion:
Clinically severe lithium poisoning patients were treated with extracorporeal toxin removal in Hong Kong. Extracorporeal TReatments In Poisoning criteria can serve as a reference in considering extracorporeal toxin removal treatment for lithium poisoning patients. Nevertheless, Extracorporeal TReatments In Poisoning criteria recommend more extracorporeal toxin removal treatment than it was actually done. Lithium poisoning patients with positive Extracorporeal TReatments In Poisoning criteria have been managed without extracorporeal toxin removal. No statistically significant adverse outcome was observed in these cases.
Keywords
Introduction
Lithium is the first-line treatment for bipolar disorder. 1 It has a narrow therapeutic index. The therapeutic serum level of lithium is 0.6–1.2 mmol/L. 2 Lithium poisoning has three different clinical manifestations, namely, acute (acute overdose by a patient who is not on lithium therapy), acute-on-chronic (acute overdose in a patient who is on lithium therapy), and chronic poisoning (progressive poisoning in a patient who is on lithium therapy). 3 Toxicity in single acute overdose is usually mild while acute-on-chronic and chronic overdose may result in significant toxicity. 3 Neurotoxicity is predominant in lithium poisoning. Neuropsychiatric symptoms range from tremors, hyperreflexia, agitation, ataxia to seizures, myoclonus, and coma. Gastrointestinal symptoms such as nausea and vomiting are more prominent in acute overdose. Cardiovascular toxicities include non-specific T-wave changes and prolonged QTc in electrocardiography, bradycardia, and hypotension. 4
The management of lithium poisoning is mainly supportive. Adequate urine output should be ensured by volume replacement. Activated charcoal does not effectively bind lithium. 5 Gastrointestinal (GI) decontamination with gastric lavage or whole bowel irrigation can be considered in significant acute overdose. 4 Given the pharmacokinetics of lithium, including low volume of distribution (0.6–0.9 L/kg) and no plasma protein binding, 6 extracorporeal toxin removal (ECTR) can be used for enhanced elimination in severe lithium poisoning. In addition, lithium is not metabolized and is eliminated almost entirely (95%) by kidneys, the use of ECTR can be life-saving in poisoning patients with impaired renal elimination. According to the Extracorporeal TReatments In Poisoning (EXTRIP) workgroup, recommendations for ECTR in lithium poisoning patients include serum lithium concentration ([Li+]) >4.0 mmol/L with impaired kidney function, presence of a decreased level of consciousness, seizures or life-threatening dysrhythmias irrespective of [Li+] while suggestions for ECTR include [Li+] >5.0 mmol/L or presence of confusion. 2 These recommendations and suggestions are sometimes referred as “EXTRIP criteria” in the literature (Figure 1). A study in Paris has compared locally derived decision rules to the EXTRIP criteria. 7 It demonstrated that EXTRIP criteria would have been indicated in more patients than was actually done, with no demonstrated improvement in outcome.
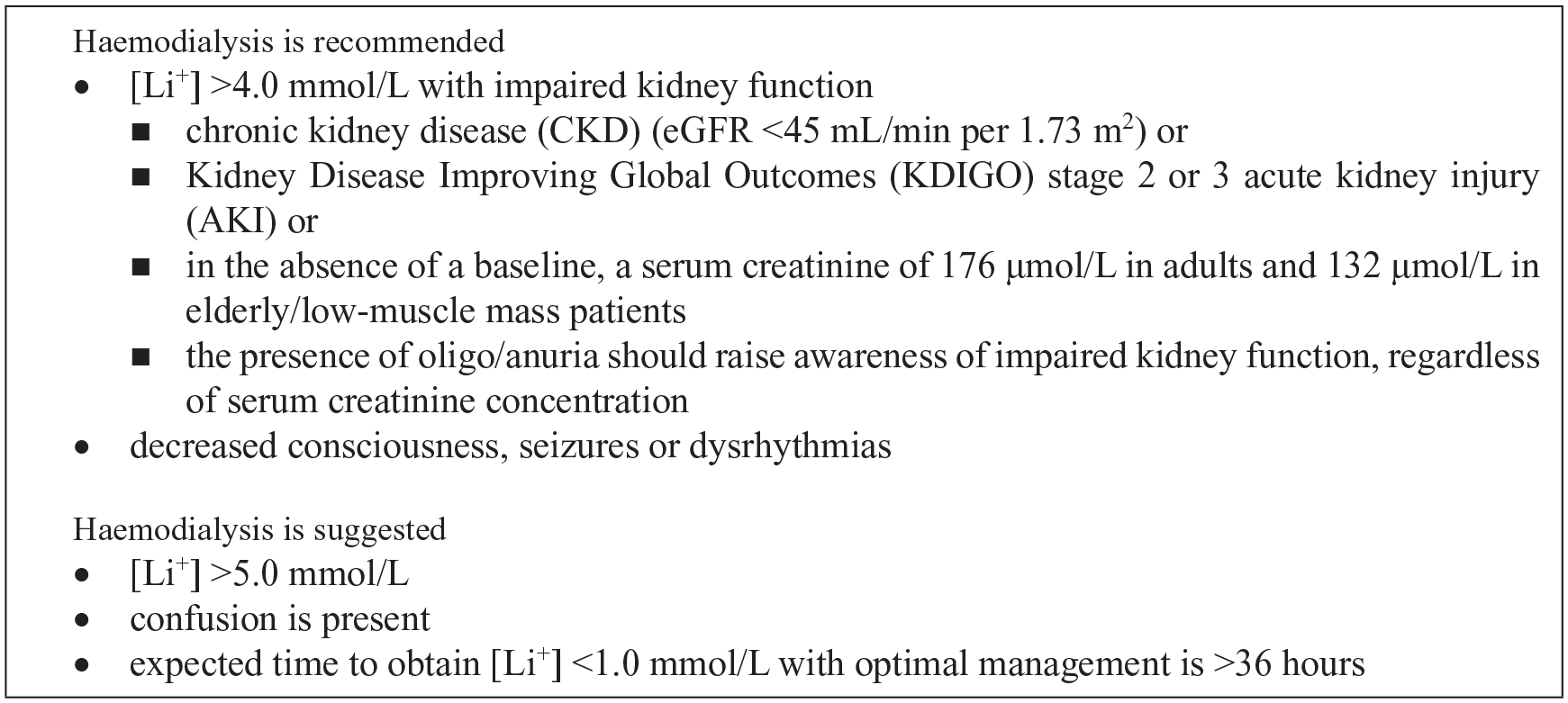
The Extracorporeal TReatment In Poisoning (EXTRIP) criteria for hemodialysis in lithium poisoning patients.
The aim of this study was to identify the pattern for using ECTR in managing lithium poisoning in Hong Kong and compare the outcomes in ECTR-treated patients and non-ECTR-treated patients if indicated for treatment.
Methods
This retrospective cohort study was conducted in Hong Kong Poison Information Centre (HKPIC). Medical records of lithium poisoning presented between 1 January 2009 and 31 December 2019 were retrieved from HKPIC database (Poison Information and Clinical Management System (PICMS)). All adult lithium poisoning patients (age ⩾18 years) with at least one supratherapeutic serum lithium concentration ([Li+] >1.2 mmol/L) were included in this study. Patients with clinical presentation and/or outcome judged to be unrelated to lithium poisoning were excluded from the study.
Data were retrieved from PICMS and electronic patient record (ePR) of Hospital Authority, and subsequently tabulated in Microsoft Excel. Data collected included patients’ demographics (age, sex, and co-morbidities), lithium poisoning history (poisoning pattern, reason of exposure, presumed ingested dose, formulation, and co-ingestion), clinical data (vital signs, symptoms, clinical outcomes, length of hospital stay, and intensive care unit (ICU) admission), laboratory findings (admission and peak serum concentrations of creatinine and lithium) and management (GI decontamination, intravenous fluid, mechanical ventilation, and ECTR).
Impaired renal function is defined according to the EXTRIP workgroup definition, which includes chronic kidney disease (CKD) (eGFR <45 mL/min per 1.73 m2), Kidney Disease Improving Global Outcomes (KDIGO) stage 2 or 3 acute kidney injury (AKI), in the absence of a baseline, a serum creatinine of 176 µmol/L in adults, and 132 µmol/L in elderly/low-muscle mass patients. The presence of oligo/anuria should raise awareness of impaired kidney function, regardless of serum creatinine concentration. 2 KDIGO criteria defined stage 2 AKI as serum creatinine being 2.0–2.9 times baseline or urine output <0.5 mL/kg/h for ⩾12 h, while stage 3 AKI as serum creatinine being 3.0 times baseline, increase in serum creatinine to ⩾353.6 µmol/L, urine output <0.3 mL/kg/h for ⩾24 h, or anuria for ⩾12 h. 8
Continuous variables are expressed as mean or median and categorical variables as absolute values (percentage). To identify the predictors of ECTR requirement, univariate analysis is performed followed by multivariate analysis. Categorial variables are compared between groups using the chi-square or Fisher’s exact tests as appropriate. Continuous normally distributed variables are compared using Student’s t-test. For continuous variables that are not normally distributed, differences in medians between groups are compared using the Mann–Whitney U test. Backward stepwise logistic regression was performed to identify the risk factors for severe poisoning outcome. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS). A two-tailed p-value of <0.05 is considered statistically significant.
Results
Basic demographics
One hundred twenty-one lithium poisoning records fulfilling the inclusion criteria were retrieved. Excluding 9 cases with clinical presentation and/or outcome unrelated to lithium poisoning, 112 lithium-poisoned patients were included in the data analysis. The average number of cases per year was 10.2 (standard deviation (SD) = 2.4). There were 41 male patients (37%) and 71 female patients (63%) with median age of 49 years (interquartile range (IQR) = 11). Regarding poisoning pattern, 50 cases were acute-on-chronic (45%) and 62 cases were chronic (55%) poisonings. No acute poisoning based on the previously mentioned definition was reported in this study. Thirty-six patients fulfilled at least one EXTRIP criterion for ECTR, among which 20 (56%) were treated with ECTR (Table 1). In addition, three patients not fulfilling any EXTRIP criteria were treated with ECTR. Among the 23 patients undergone ECTR, 15 received continuous renal replacement therapy (CRRT), 7 received hemodialysis, and 1 received sustained low-efficiency dialysis (SLED).
Patients who fulfilled at least one EXTRIP criterion for ECTR (n = 36).
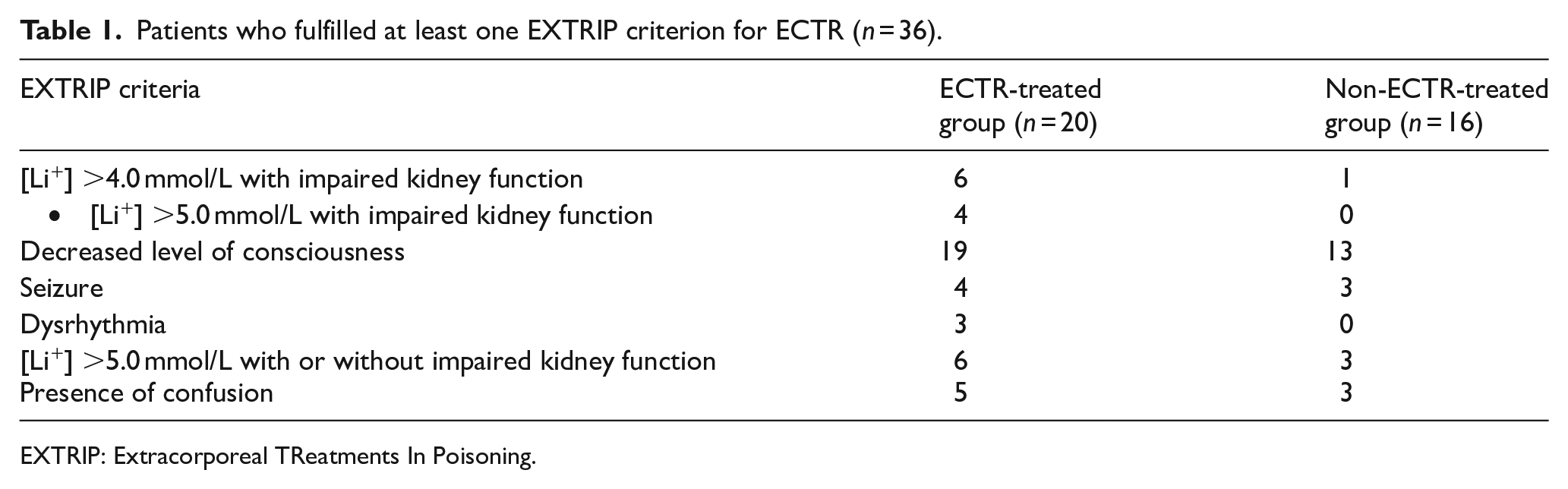
EXTRIP: Extracorporeal TReatments In Poisoning.
ECTR-treated versus non-ECTR-treated group
Comparisons between ECTR-treated group (n = 23) and non-ECTR-treated group (n = 89) are shown in Table 2.
Comparisons between ECTR-treated and non-ECTR-treated group.
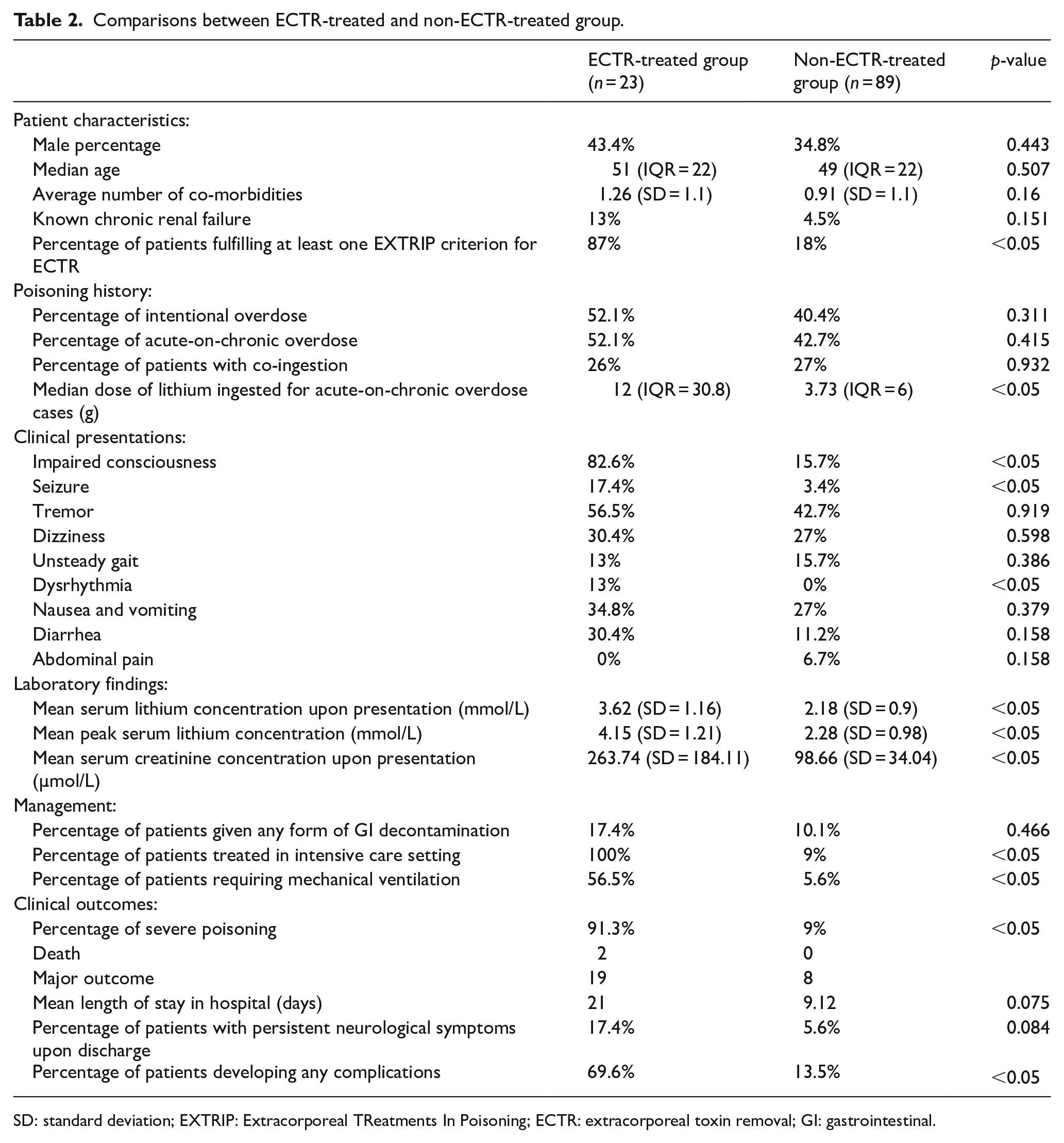
SD: standard deviation; EXTRIP: Extracorporeal TReatments In Poisoning; ECTR: extracorporeal toxin removal; GI: gastrointestinal.
Patient characteristics
There was no statistically significant difference between the sex distribution, median age, and average number of co-morbidities between ECTR-treated and non-ECTR-treated groups. Chronic renal failure was more prevalent in patients undergone ECTR, but not statistically significant (13% vs 4.5%, p = 0.151). Significantly larger proportion of patients had fulfilled at least one EXTRIP criterion for ECTR in the ECTR-treated group (87% vs 18%, p < 0.005).
Lithium poisoning history
Poisoning pattern in terms of intentional overdose, acute-on-chronic overdose, and co-ingestion was similar between the two groups. The median dose of lithium ingested for acute-on-chronic cases was significantly larger in patients treated with ECTR (12 g (IQR = 30.8) vs 3.73 g (IQR = 6), p < 0.005).
Clinical presentations
Impaired consciousness (82.6%), tremor (56.5%), and nausea and vomiting (34.8%) were the most common presentations among ECTR-treated patients while tremor (42%), dizziness (27%), and nausea and vomiting were the most common among non-ECTR-treated patients. The percentage of patients with impaired consciousness, seizure, and dysrhythmia was significantly higher in ECTR-treated group than non-ECTR-treated group (p < 0.05).
Laboratory findings
The admission (3.62 mmol/L (SD = 1.16) vs 2.18 mmol/L (SD = 0.9), p < 0.05) and peak (4.15 mmol/L (SD = 1.21) vs 2.28 mmol/L (SD = 0.98), p < 0.05) serum lithium concentrations of ECTR-treated group were significantly higher. Patients underwent ECTR also got a significantly higher serum creatinine concentration upon presentation (263.74 µmol/L (SD = 184.11) vs 98.66 µmol/L (SD = 34.04), p < 0.05).
Management
100% of patients undergone ECTR were managed in intensive care unit (ICU) while only 9% of non-ECTR-treated patients had been admitted to ICU (p < 0.005). Significantly higher percentage of patients of ECTR-treated group required mechanical ventilation (56.5% vs 5.6%, p < 0.05). Comparable proportion of patients were given any form of GI decontamination.
Clinical outcomes
Patients treated with ECTR were more frequently having a severe poisoning outcome (91.3% vs 9%, p < 0.05). Severe poisoning outcome is defined as patient died or patient’s outcome was judged as major effect in PICMS. Two patients undergone ECTR died. More patients in the ECTR-treated group developed complications (69.6% vs 13.5%, p < 0.05) which included nephrogenic diabetes insipidus, rhabdomyolysis, sepsis, and/or pneumonia. None developed ECTR-related complications. Length of hospital stay and proportion of patients with persistent neurological symptoms upon discharge were not significantly different between two groups. We classified persistent neurological symptoms as any documented neurological deficits upon discharge in the discharge summary. Reported symptoms include dysphagia, failed phonation, critical illness polyneuropathy, encephalopathy, limb rigidity, incoherent speech, tremor, and disorientation.
Backward stepwise logistic regression was performed to identify the risk factors for severe poisoning outcome. Seizure (odd ratio (OR) = 69.2, 95% confidence interval (CI) = 1.3–3744, p = 0.038), peak serum lithium concentration (OR = 6.9, 95% CI = 2.1–22.4, p = 0.01), serum creatinine concentration upon presentation (OR = 1.04, 95% CI = 1.00–1.08, p = 0.014) were significantly associated with severe poisoning outcome.
Subgroup analysis was performed on patients with at least one indication for ECTR as defined by EXTRIP criteria (n = 36) (Table 3). The proportion of severe poisoning remained significantly higher in the ECTR-treated group (90% vs 43.7%, p < 0.05). Complication rate, length of hospital stay, and proportion of patients with persistent neurological symptoms upon discharge were not significantly different between two groups.
Subgroup analysis on patients with at least one indication for ECTR as defined by EXTRIP guideline.

EXTRIP: Extracorporeal TReatments In Poisoning; DI: diabetes insipidus.
Discussion
In this study, not all patients fulfilling EXTRIP criteria underwent ECTR for lithium poisoning. There were 16 out of 36 (44%) patients fulfilled EXTRIP criteria but did not receive ECTR. Among these patients, a majority of them presented with decreased level of consciousness, one of the EXTRIP criteria for ECTR. Some of them had a relatively low serum lithium concentration. Their clinical condition improved and serum lithium concentration dropped gradually with supportive treatment. Some patients had co-ingested other drugs or concomitant medical condition, such as zopiclone overdose and hypoglycemia, which could be attributed to patients’ impaired consciousness. Decreased level of consciousness was not quantitatively defined by the EXTRIP workgroup. We used Glasgow Coma Scale (GCS) <15 as the definition as in another study. 9 The broad definition of decreased level of consciousness could be the reason why more patients fulfilled EXTRIP criteria for ECTR than it was actually done. Similarly, ECTR is recommended for lithium poisoning in the presence of seizures. In this study, a man in his 40s developed seizure. He has normal renal function and a mildly elevated [Li+] 1.84 mmol/L. ECTR was not performed, and he has a spontaneous recovery.
Serum lithium concentration does not necessarily correlate with clinical toxicities. A female patient in her 20s with [Li+] 5.57 mmol/L was declined for ICU admission as she was relatively asymptomatic. She had not developed impaired consciousness nor AKI. She was managed with supportive treatment and intravenous fluid. Her [Li+] dropped to 0.8 mmol/L within 2 days with uneventful recovery. Another woman in her 40s with [Li+] 5.1 mmol/L also had normal renal function was managed without ECTR and has uneventful recovery. Similarly, hemodialysis was initially suggested in a 29-year-old female patient with [Li+] 5.2 mmol/L. She was clinically well and her [Li+] dropped gradually upon confirmatory testing. Hemodialysis was withheld for this patient. All three cases mentioned here were acute-on-chronic poisoning cases. Waring et al. 3 suggested that acute-on-chronic and chronic lithium poisoning were at greatest risk of severe toxicity. In the contrary, Oakley et al. 10 reported that severe lithium neurotoxicity rarely results from acute ingestion of lithium, even in patients currently taking lithium. 10 Delayed diffusion of lithium to brain can explain the absence of symptoms in patients despite elevated [Li+] in acute setting. 10 Serum lithium concentration should not be used as the sole factor in considering ECTR. Patients’ clinical presentations and progress have been taken into account in clinical practice.
The use of ECTR as the management of lithium poisoning depends on local resources. In this study, a man in his 60s presented with single seizure, confusion, and AKI was managed conservatively due to the limited capacity of ICU. The administration of ECTR might also be subject to clinician’s clinical decision. A 51-year-old man with [Li+] 2.7 mmol/L developed impaired consciousness (GCS = 3) and AKI requiring intubation and inotrope support. He was not managed with ECTR and the reason of which was not mentioned. He was discharged home after a prolonged hospital stay of 59 days. Variability in treatment decisions in lithium poisoning was evident. 11
In this study, most patients undergone ECTR (87%) had fulfilled at least one EXTRIP criterion. They were more likely presenting with life-threatening symptoms including impaired consciousness, seizure and dysrhythmia, having higher serum lithium concentration and higher serum creatinine upon presentation. They more frequently required mechanical ventilation (56.5%) and all of them required intensive care. We conclude that ECTR-treated group was a group of patients with clinically life-threatening lithium poisoning. For this reason, they had poorer clinical outcome as compared with the non-ECTR-treated group. This group of patients had longer hospital stay which might increase the risk of hospital-acquired infection. None of them developed ECTR-related complications. ECTR per se is unlikely a risk factor for severe poisoning outcome.
Subgroup analysis was performed on patients with at least one indication for ECTR as defined by EXTRIP criteria. The proportion of severe poisoning is significantly higher in the ECTR-treated group compare with non-ECTR-treated group. As stated above, ECTR per se is not a risk factor for severe poisoning. The decision for ECTR in these cases was probably not determined by EXTRIP criteria alone, but the patients’ general clinical condition, progress and clinicians’ own clinical decision. Patients undergone ECTR could be critically ill and ECTR served as a life-saving treatment. For clinically stable patient with preserved renal function, it may be reasonable to withhold the decision for ECTR even if an EXTRIP criterion is present. Moreover, EXTRIP workgroup published its recommendations for lithium poisoning in 2015. Before that, recommendations for treatment of lithium poisoning were based on individual observational studies. 11 Currently, there is no high-quality evidence proving that the utilization of EXTRIP criteria is clinically superior when comparing with conventional clinical decision for ECTR.
Study limitations
The key limitation of this study was related to its retrospective nature. It relied on the accuracy and completeness of data. There was incomplete information in medical record. Missing data on vital signs were especially significant. The outcome severity and relation were subject to individual judgment of clinicians who entered the data. However, there would not be significant discrepancy in grading cases with major outcomes or death with reference to the American Association of Poison Control Centers’ National Poison Data System. 12 All death or major effect cases were further reviewed by clinical toxicologist to ensure that the grading was appropriate. 13 There was no objective indicator to judge the degree of outcome severity in relation to lithium poisoning. Clinical outcomes of the patients can depend on individual susceptibility, co-morbidities, effects of acutely co-ingested drugs, or interactions with chronic medications.
As commented by Hoffman, 14 it should never be expected that the first iteration of EXTRIP’s recommendations would stand as the ultimate decision tool. EXTRIP workgroup had initiated an evidence-based evaluation of the use of ECTR in lithium poisoning and provided a practical guideline that might help facilitate clinical decision.
Conclusion
Clinically severe lithium poisoning patients were treated with ECTR in Hong Kong. Life-threatening clinical presentation (e.g. seizures), high serum lithium concentration, and renal impairment are associated with severe poisoning outcome in lithium poisoning. Most lithium poisoning patients undergone ECTR had fulfilled at least one EXTRIP criterion. EXTRIP criteria can therefore serve as a reference in considering ECTR treatment for lithium poisoning patients. Nevertheless, EXTRIP criteria recommend more ECTR treatment than it was actually done in this study. Lithium poisoning patients with positive EXTRIP criteria have been managed without ECTR. No statistical significant adverse outcome was observed in these cases.
Footnotes
Acknowledgements
The authors acknowledge Mr Man Ho Wong and Miss Gia Chu for their assistance on data retrieval.
Author contributions
Both authors contributed to the study design and data interpretation. S.H.C. collected the data and drafted the manuscript for intellectual content. C.K.C. analyzed the data and revised the manuscript for intellectual content. The authors certify that we have each made a substantial contribution so as to qualify for authorship and that we have approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data of the study were retrieved from Hong Kong Poison Information Centre database (Poison Information and Clinical Management System) and electronic patient record of Hospital Authority.
Informed consent
Patient consent was waived by the Ethics Committee.
Ethical approval
This study was approved by the Research Ethics Committee (Kowloon Central/ Kowloon East) of Hospital Authority (reference no. KC/KE-20-0128/ER-2).
Human rights statement
Patients’ privacy was not infringed in this study.