
Abstract
Introduction:
Neutropenic sepsis is an emergency sequela in post-chemotherapy fever. Its definition comprises of spectrums of diseases with variable quoted mortality. This study aims to evaluate the incidence of “modified” neutropenic sepsis, with a more stringent definition employed. Predictive risk factors toward occurrence of “modified” neutropenic sepsis among Chinese patients would also be explored.
Methods:
A single-center retrospective longitudinal study was conducted in a medium-sized regional hospital in Hong Kong. All patients with diagnoses of post-chemotherapy fever fulfilling the inclusion and exclusion criteria were recruited. Baseline characteristics and outcome variables of each case subject were collected. Six potential predictive risk factors were chosen for further analysis. Case subjects were followed up for the inpatient progress and outcomes. Relative risks of each risk factor to “modified” neutropenic sepsis were calculated.
Results:
A total of 135 case subjects were recruited. Five developed “modified” neutropenic sepsis, that is, incidence 3.70% (95% confidence interval = 1.59%–8.38%). Only background hematological malignancy was found to be significantly associated with the outcome of “modified” neutropenic sepsis (Relative Risk [RR] 13.2, 95% confidence interval = 1.56–115.70, p = 0.010), with an incidence of 12.9% (95% confidence interval = 5.14%–28.85%). Hematological malignancy was also found to be significantly associated with lower median absolute neutrophil counts (0.95 × 109/L vs 2.3 × 109/L, p = 0.005) and longer median hospital stay (8 days vs 6 days, p < 0.001).
Conclusion:
Incidence of “modified” neutropenic sepsis is low. Hematological malignancy is associated with significantly higher rate of “modified” neutropenic sepsis.
Introduction
Myelosuppression is a known major dose-related toxicity for systemic chemotherapy for cancers. 1 Fever occurs commonly in the setting of neutropenia, especially in severe neutropenia which is defined as absolute neutrophil counts <0.5 × 109/L. 2 It is well proven that the risk of febrile neutropenia increases with the duration and severity of neutropenia in both acute leukemic patients 3 and patients with solid tumors. 4
Definitions for neutropenic sepsis (also termed as febrile neutropenia or neutropenic fever) varied among the literature, but the definition by the National Institute for Health and Care Excellence (NICE) appears to be the most adopted one, where neutropenic sepsis is defined as a temperature ⩾38°C plus an absolute neutrophil count of <0.5 × 109/L. 5 Reported incidence 6 and mortality 7 varied widely in the literature, for both non-hematological malignancies and hematological malignancies, probably due to the ambiguous and non-specific nature of the NICE definition. 8 Furthermore, the presumed emergency nature of post-chemotherapy fever did not appear to be parallel to our frontline clinical experience. Therefore, a novel term “modified” neutropenic sepsis was proposed in this study to better delineate the outcome, since it was defined more stringently and was expected to be more representative of serious clinical outcomes. It was defined as absolute neutrophil counts <0.5 × 109/L AND sepsis clinically and/or positive blood culture. (N.B. Clinical sepsis was defined as quick sequential organ failure assessment (qSOFA) score of at least two.) 9
The primary objective of this study was to evaluate the incidence of “modified” neutropenic sepsis among post-chemotherapy fever patients after disposal from the Emergency Department (ED). Post-chemotherapy fever patients are a group of heterogeneous population with different background characteristics. They may be receiving different chemotherapeutic agents with different intensities, presenting to A&E at a different timing after the chemotherapy, and so on. Thus, we are interested in the actual portion of them who really deteriorated (represented by the new definition we proposed) as a final outcome during the inpatient stay, in the scope of neutropenic sepsis as a result (where it is considered relating to the myelosuppression effect of chemotherapy). As a result, we may try to explore or propose further adjustment in our current disposals in the ED field based on this finding, for example, feasibility of admitting to Emergency Medicine Ward (EMW) for low-risk case.
Secondary objective of this study is to evaluate selected predictive risk factors (as listed below) toward occurrence of “modified” neutropenic sepsis, that is, clinical deterioration after admission to ward. Different risk factors have already been evaluated in the literature for predicting the severity of the febrile neutropenia episodes and its consequences. 10 Multinational Association for Supportive Care in Cancer (MASCC) score 11 is the most commonly used scoring systems in the literature. An MASCC score of less than 21 indicates a high risk for severe neutropenia. However, this system is not widely adopted for risk stratification in various A&E departments in this locality, as general consensus in terms of case disposal in different A&E departments are largely similar: urgent admission to medical wards (in reverse isolation room if available), after prompt broad-spectrum antibiotic administration, in view of a worrisome of subsequent clinical deterioration in patients with neutropenic fever. Piperacillin-tazobactam is the recommended antibiotic of choice in most EDs for coverage of pseudomonas species. 12 Availability of isolation rooms could be a challenge during winter surge with admission blocks and during massive infectious disease outbreaks such as the recent Coronavirus Disease 2019 (COVID-19) pandemic. Therefore, predictive risk factors, and even a well-validated and accepted scoring system in A&E settings to predict for severe neutropenia or serious clinical outcomes among post-chemotherapy fever patients, may serve a better triage function in the above clinical situations, and hence a better utilization of resources.
Methods
A single-center retrospective longitudinal study was conducted in a medium-sized regional hospital in Hong Kong. With reference to the departmental guideline, post-chemotherapy fever, in this study, was defined as at least a single documented temperature reading of at least 38°C (either by self or by any healthcare worker including upon triage at A&E) within 4 weeks’ post-chemotherapy treatment. Patients attending for “post-chemotherapy fever” are triaged as Category II or above (Cat I = Critical; Cat II = Emergency), according to the departmental guideline. Patients being triaged as Category I and II in the period of January to December 2019 were identified retrospectively using the A&E Information System (AEIS). All patients with diagnoses of post-chemotherapy fever (or other equivalent diagnoses) on the A&E consultation records were retrieved. They were reviewed whether the following inclusion and exclusion criteria were fulfilled. Inclusion criteria were adult Chinese patients with age ⩾18 years, at least a single documented temperature reading of ⩾38°C, and recent chemotherapy treatment (excluding those only on targeted therapy or immunotherapy) within 4 weeks. Exclusion criterion was subjects with critical conditions on presentations, significant missing data because of premature hospital discharge or no prior follow-up in public sector (see Figure 1).
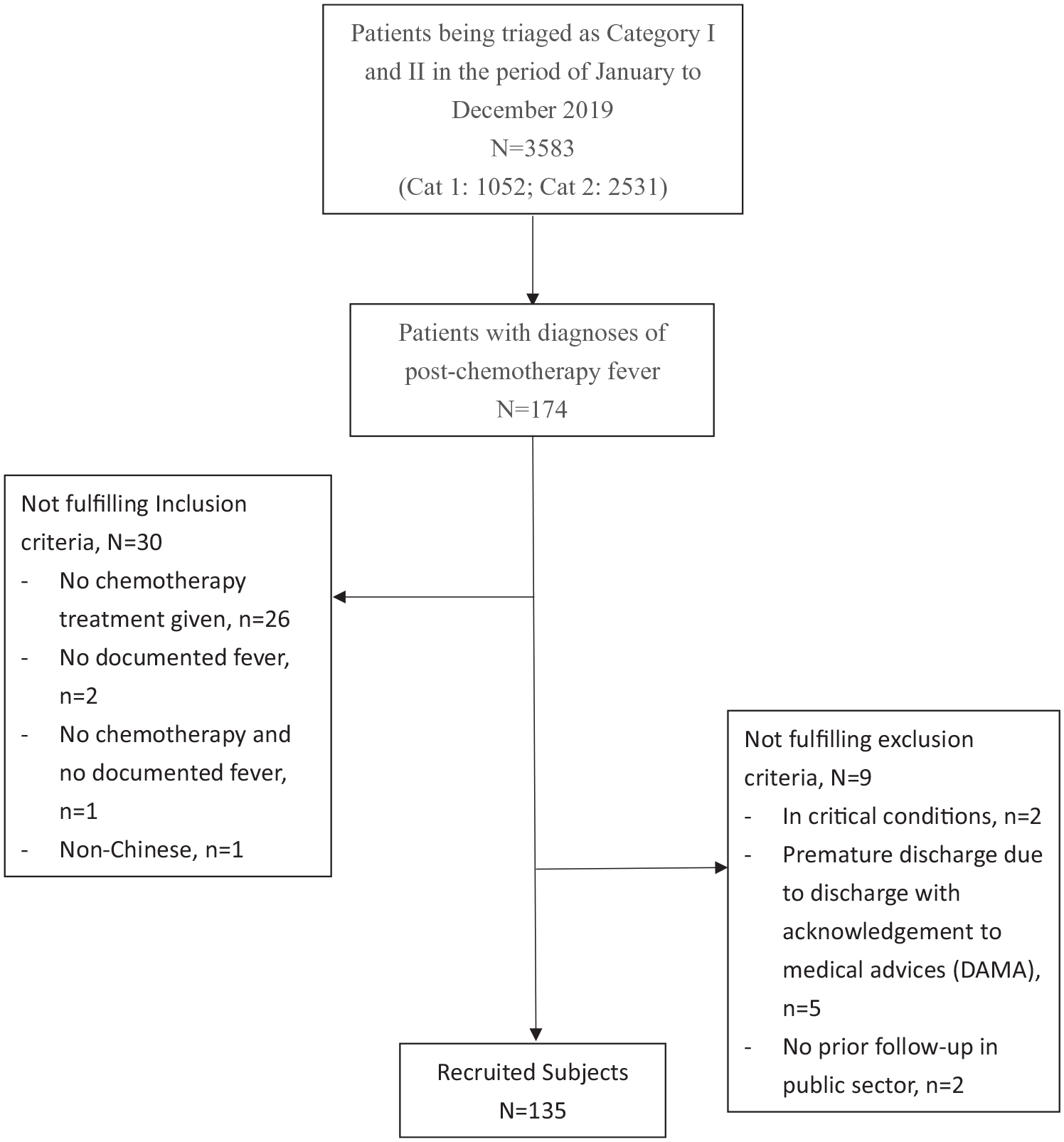
Recruitment flowchart.
Sample size was calculated using PASS 13 two-sided confidence intervals (Wilson score) for a proportion. Assuming the rate of neutropenic sepsis is 10%, 13 a sample size of 117 would be required to produce a two-sided 95% confidence interval (CI) with a precision of 5.5%. Estimation of caseloads of post-chemotherapy fever cases in our center was 180 cases per year, while estimation of cases not fulfilling inclusion and exclusion criteria was 20%. So based on the above two assumptions, the expected number of cases required was 144. It is slightly more than the calculated sample size (i.e. 117) as above, since it is anticipated there may be a problem of significant missing data where more cases may be excluded during the data entry procedure.
Baseline characteristics and outcome variables of each case subject with respect to the particular A&E attendance episode were collected. The data were collected by reviewing the A&E consultation notes, the inpatient discharge summaries, and the laboratory parameters via electronic patient record (ePR). With reference to the literature, six variables were chosen as potential predictive risk factors for further analysis: age ⩾65 years old, 14 female sex, 15 past history of diabetes, 16 recent lymphopenia 17 (which was defined as last lymphocyte count <1.0 × 109/L), background hematological malignancy, 18 and no recent administration of granulocyte colony-stimulating factor (G-CSF) prior to presentation. 19 Case subjects were followed up for the inpatient progress and outcomes to assess the following parameters: occurrence of “modified” neutropenic sepsis, severe neutropenia (absolute neutrophil counts <0.5 × 109/L) without sepsis (i.e. no clinical sepsis and negative blood culture), length of stay, and admission to intensive care unit (ICU). Relative risks of each risk factor to “modified” neutropenic sepsis with 95% CI were calculated. Baseline characteristics were compared using Pearson’s chi-square test, Fisher’s exact test, independent t-test, and Mann–Whitney U test, as appropriate. Data analysis was conducted using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corporation, Armonk, NY, USA) and statistical significance was set at p < 0.05.
Results
There were altogether 174 post-chemotherapy fever case subjects in the cohort. Thirty-nine of them were them were excluded (see Figure 1). In particular, two of them were excluded because of critical condition upon presentation to A&E. Concerning the baseline characteristics of the 135 case subjects recruited (see Figure 1), gender ratio was approaching 1:1. Mean age of the subjects was 60.43 years. Background of non-hematological malignancies was the majority (77%). More patients (69.7%) were in an advanced stage of their background malignancies. Only 23.0% of the subjects had history of diabetes. The mean last lymphocyte count was 1.528 × 109/L. G-CSF administration was noted in 24.6% of case subjects prior to presentation to A&E.
Concerning the outcome of “modified” neutropenic sepsis, only five among total of 135 case subjects developed this outcome during the inpatient progress, that is, incidence 3.70% (95% CI = 1.59%–8.38%). In contrast, incidence of severe neutropenia (with fever), that is, literally equivalent to the term “neutropenic sepsis” by NICE guideline, was 23% (n = 31) (see Table 1). In other words, only 5 out of 31 severely neutropenic patients, that is, 16.1% developed a clinical sepsis and/or bacteremia.
Primary and secondary outcomes.
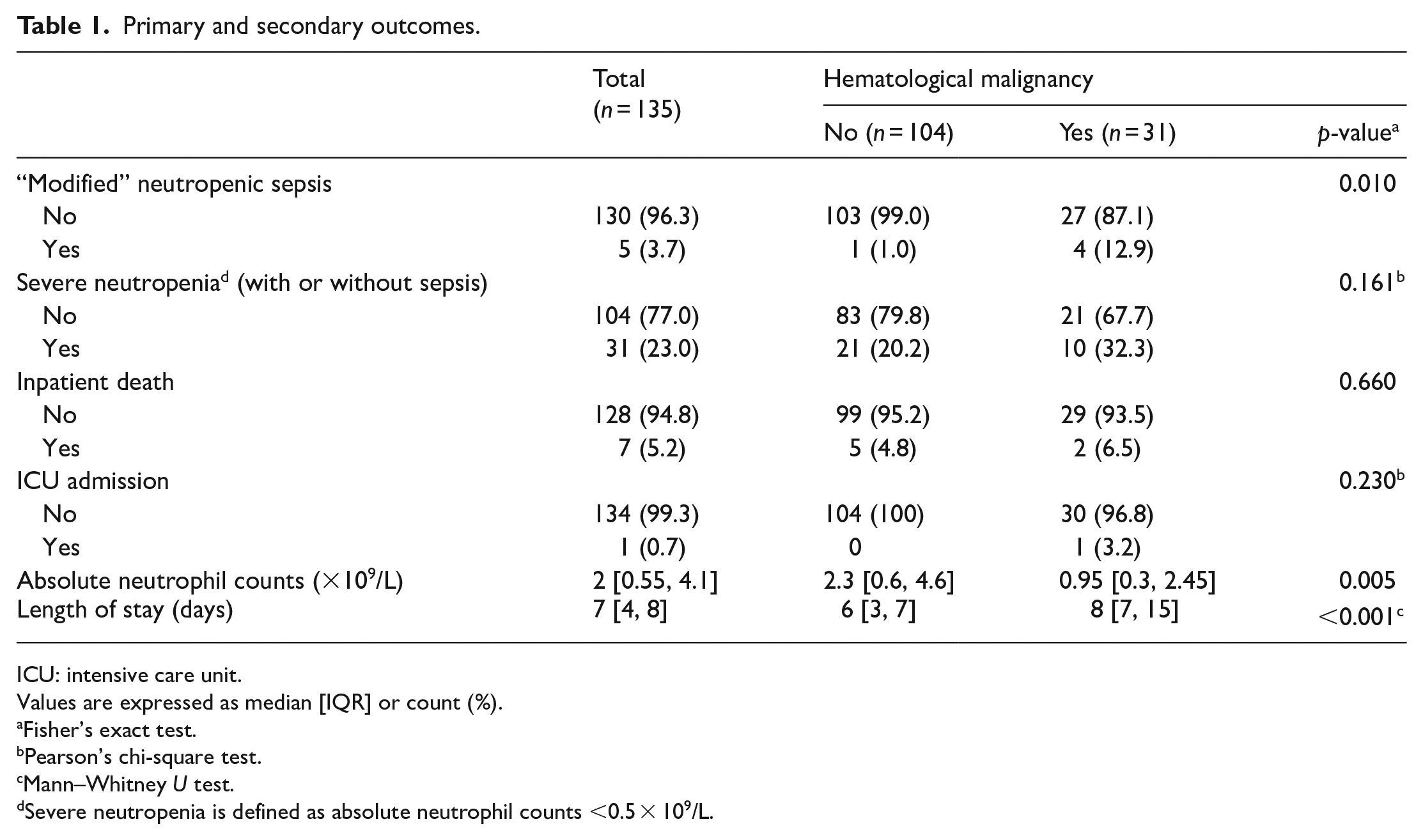
ICU: intensive care unit.
Values are expressed as median [IQR] or count (%).
Fisher’s exact test.
Pearson’s chi-square test.
Mann–Whitney U test.
Severe neutropenia is defined as absolute neutrophil counts <0.5 × 109/L.
Among the predictive risk factors selected for analysis, background hematological malignancy was found to be significantly associated with the outcome of “modified” neutropenic sepsis (RR = 13.42, 95% CI = 1.56–115.70, p = 0.010). Attributable risk of hematological malignancy to “modified” neutropenic sepsis was 11.94% (95% CI = 1.79%–22.10%) while its number-needed-to-treat (NNT) was 8.38 (95% CI = 4.52–55.9) (see Table 2). Incidence of “modified” neutropenic sepsis in the hematological malignancy group was 12.9% (95% CI = 5.14%–28.85%), while incidence in the non-hematological malignancy group was 0.96% (95% CI = 0.17%–5.25%) (see Table 2). Other chosen risk factors were not found to be significantly associated with “modified” neutropenic sepsis (see Table 2). Further to “modified” neutropenic sepsis, background hematological malignancy was also found to be significantly associated with lower median absolute neutrophil counts (0.95 × 09/L vs 2.3 × 109/L, p = 0.005) and longer median hospital stay (8 days vs 6 days, p < 0.001). However, neither rates of severe neutropenia (with or without sepsis), inpatient mortality nor admission to ICU was found to be significantly higher in the hematological malignancy group (see Table 1).
Baseline characteristics and association with “modified” neutropenic sepsis.
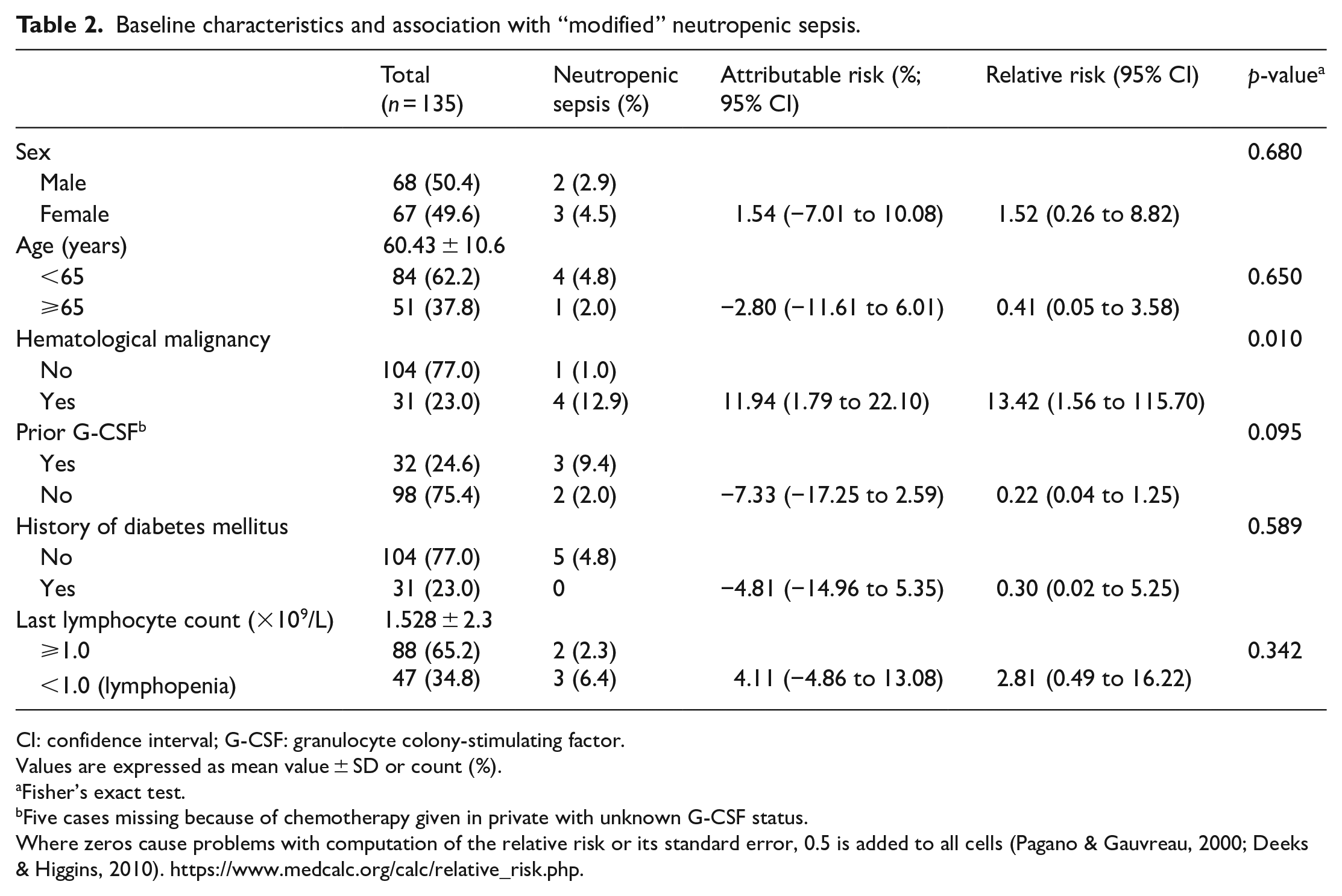
CI: confidence interval; G-CSF: granulocyte colony-stimulating factor.
Values are expressed as mean value ± SD or count (%).
Fisher’s exact test.
Five cases missing because of chemotherapy given in private with unknown G-CSF status.
Where zeros cause problems with computation of the relative risk or its standard error, 0.5 is added to all cells (Pagano & Gauvreau, 2000; Deeks & Higgins, 2010). https://www.medcalc.org/calc/relative_risk.php.
Discussion
Neutropenic fever has been more acknowledged as an oncological emergency since the incident of mortality due to post-chemotherapy septicemia after a 5-h delay of antibiotic dated in 2011. 20 Various emergency departments in Hong Kong developed protocols for this specific entity to improve the door-to-antibiotic time. However, one local study 21 suggested that shortening of door-to-antibiotic time did not result in significant reduction in adverse outcomes, possibly due to a relatively low incidence of serious clinical outcomes among post-chemotherapy fever patients as a whole. With a more stringent term “modified” neutropenic sepsis, which was expected to have a better reflection of adverse clinical outcomes, employed in this study, a low overall incidence of “modified” neutropenic sepsis was found among the post-chemotherapy fever patients attending A&E. Moreover, only 31% among all the subjects developed a severe neutropenia (which is defined as absolute neutrophil counts <0.5 × 109/L), which may indirectly predict a low incidence of “modified” neutropenic sepsis.
Background hematological malignancy was suggested in the literature 18 to be a predictor to neutropenic fever. With more stringent criteria termed “modified” neutropenic fever employed in this study, it still appears parallel to previous finding in the literature. However, during the analysis, the baseline characteristics, namely, age (p = 0.004), prior G-CSF status (p < 0.001), and prior history of diabetes (p = 0.059) were found unadjusted between the hematological malignancy group and non-hematological malignancy group (see Table 3). The prior G-CSF status was found to have a possible association with “modified” neutropenic sepsis, although a statistical significance was not yet reached (p = 0.095) (see Table 2). So, in order to better delineate the relationship between background hematological malignancy and the outcome of “modified” neutropenic sepsis, a further study adjusting the prior G-CSF status if not the above three baseline characteristics would be suggested.
Comparison of baseline characteristics between subjects with and without hematological malignancy.
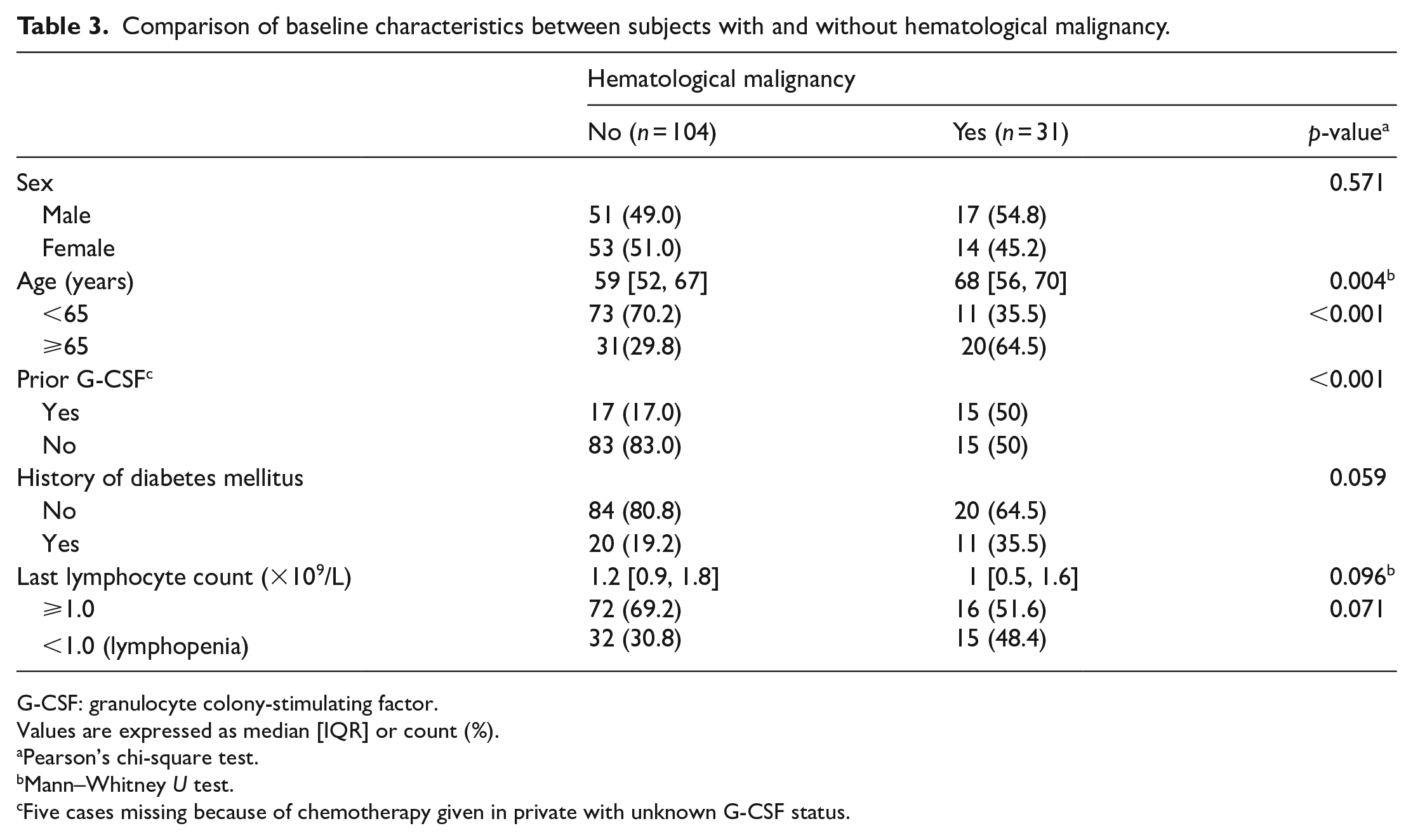
G-CSF: granulocyte colony-stimulating factor.
Values are expressed as median [IQR] or count (%).
Pearson’s chi-square test.
Mann–Whitney U test.
Five cases missing because of chemotherapy given in private with unknown G-CSF status.
In reviewing the cohort with outcome of “modified” neutropenic sepsis, three had clinical sepsis (all with qSOFA = 2) during their inpatient courses. One had positive blood culture while the remaining one had both clinical sepsis (qSOFA = 2) and positive blood culture. Concerning the bacteriology in this subset, one had methicillin-sensitive Staphylococcus aureus isolated while the other one had Escherichia coli and Klebsiella isolated in blood culture. All the above isolated organisms were sensitive to piperacillin-tazobactam.
A mortality rate of 5.19% (n = 7) were recorded in this cohort of total 135 post-chemotherapy fever case subjects. Only one of the mortalities developed severe neutropenia. Therefore, it remained uncertain whether the degree of neutropenia correlates with the outcome of mortality. The total number of mortalities in the non-hematological group was observed to be higher (n = 5). It could be partly explained by the much greater number of patients in the non-hematological group (104 vs 31). And, in fact, we were rather interested in the mortalities related to severe neutropenia since the mortality due to non-neutropenic infections may not be related to the myelosuppression effect caused by chemotherapy. There was only one mortality caused by severe neutropenia and this happened in the hematological group, while the mortalities in the non-hematological group had normal or elevated white cell counts. Further study with a larger cohort may further delineate the relationship between mortality due to neutropenic infections and background hematological malignancies.
Overall bacteriology of the cohort was also reviewed. Positive growths on blood culture were found in 9.63% (n = 13) of case subjects in the cohort. E. coli was the most prevalent bacteria (n = 7) isolated, where majority (n = 6) of them were non-extended-spectrum beta-lactamase (ESBL) producing. Two had poly-microbial bacteremia. None of them had pseudomonas nor fungus isolated from blood culture. Piperacillin-tazobactam still appeared to be an effective antibiotic of choice where only two out of the 13 positive blood cultures yielded organisms resistant to piperacillin-tazobactam (namely, one with enterococcus requiring vancomycin and one with ESBL producing E. coli requiring meropenem). However, non-pseudomonal agents with good coverage of gram-negative bacilli, such as third-generation cephalosporins, appear to be a safe option when stepping down antibiotic treatment is considered.
One local study 22 performed by a team of specialty nurses in an oncology center also proposed that patients with low-risk febrile neutropenia (with the use of MASCC score for risk stratification) can be managed as outpatient effectively and safely. This study also echoes a similar conclusion with finding of a low incidence of “modified” neutropenic sepsis after admission, and an association between “modified” neutropenic sepsis and background hematological malignancies, that is, higher risk of subsequent deterioration among this patient group. Hematological malignancy was also found to be associated with a significantly longer median hospital stay (8 days vs 6 days, p < 0.001). On further review of the lengths of stay (LOS) of the cohort, 23.0% (n = 31) were discharged after a short inpatient stay (LOS ⩽3 days), where 27 of them belonged to non-hematological malignancy group.
Having a preliminary conclusion of a predictive relationship between background hematological malignancies and outcome of “modified” neutropenic sepsis, it is possible to postulate patients with background non-hematological malignancies as a “relative” low-risk group. If this postulation can be furthered confirmed by subsequent studies, a new model of management with short stays in EMW may be a possible safe disposal option, where resource allocations may be more optimized. Post-chemotherapy fever patients with background non-hematological malignancy may be considered admitting to EMW instead of medical ward after the prompt broad-spectrum antibiotic treatments in A&E, if the result of first absolute neutrophil count is normal (which is usually available within 1 h). Further study to validation of MASCC score in ED setting would also be helpful in risk stratification in further clarifying the EMW admission criteria. In our cohort, among the patients in non-hematological malignancy group developing severe neutropenia (n = 21), 19.0% (n = 4) of them developed severe neutropenia only during the inpatient stays instead of on presentations. Routine rechecking of cell counts can serve as a safety net to pick up the delayed appearances of severe neutropenia, and therefore ensure a safe EMW discharge.
Having aimed to study the adverse outcome among post-chemotherapy fever patients, a more stringent definition was set to the term “modified” neutropenic sepsis, where fewer patients fulfilling were expected. This exactly reflects the suspicion that the serious clinical outcomes only occur sparsely in the group of post-chemotherapy fever patients. However, this low positive outcome rate strongly impedes the power of this study, which is considered as a major limitation of this study. The reason behind is mainly because our hospital is neither an oncological center (meaning the situation in our case recruitment period; but new oncological outpatient service has recently started) nor bone marrow/renal transplant center. This significantly limits our caseloads of post-chemotherapy fever patients. To improve the study, maximizing the cases recruited may probably reduce this problem. With the limited caseloads as a non-oncological center (around one case every 2 days), few more years of case recruitment may be needed to improve the power of this study. Further expansion of recruited case numbers would allow the feasibility of logistic regressions for data analysis. Adjustment of other risk factors becomes possible, and hence, a better predictive relationship may be yielded.
Second, the study design allowed a good recruitment of post-chemotherapy fever patients in the selected time frame with a minimal chance of case missing (in a remote possibility of under-triage). However, the recruitment of case subjects was counted as per each A&E attendance episode. This implies one single patient may be recruited for multiple times, and hence, each patient may exert different influence toward the outcome of analysis. Increasing number of cases recruited may help balance the heterogeneity of baseline characteristics and minimize the effect contributed by each single patient.
Conclusion
Overall incidence of “modified” neutropenic sepsis is low. Background hematological malignancy is associated with significantly higher rate of “modified” neutropenic sepsis. New disposal pathway with admission to EMW may be a possible safe alternative for the patients with non-hematological malignancies. Further study to delineate this group of patients as low-risk group and to validate MASCC score in A&E settings would be considered important in developing this new disposal options.
Footnotes
Acknowledgements
The authors thank Ms Ellen Yu for her guidance throughout the statistic processing in this research.
Author contributions
All authors contributed to the concept or design. W.Y.H.M. contributed to the acquisition of data and the analysis or interpretation of data. W.Y.H.M. and P.T.S. contributed to the drafting of the manuscript. All authors contributed to the critical revision for important intellectual content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data
The data sets generated and/or analyzed during this study are available from the corresponding author.
Informed consent
Informed consent was not sought for this study because of the nature of a retrospective study, that is, the data collection happens after the cases were finished clinically.
Ethical approval
Ethical approval for this study was obtained from the Research Ethics Committee (Kowloon Central/Kowloon East; reference no. KC/KE-20-0133/ER-2).