
Abstract
Tension pneumothorax is one of the commonest life-threatening condition seen in multiple injury or polytrauma trauma victims. Chest tube insertion has been the mainstay treatment for tension pneumothorax since early 1970s until today. Despite being a common procedure performed by an emergency resident, the incidence of complications related to the procedure remains significantly high. Iatrogenic complications are particularly more common in patients that are critically ill, obese or with a flail chest. This report will be discussing on an ectopic chest tube insertion during management of a case of traumatic tension pneumothorax in an obese patient with flail chest. Further discussions are on various recent updates on chest tube insertion procedures in an emergency setting. It is vital to understand that prior to chest tube insertion, it is important to acknowledge a possibility of complicated procedure by stratifying the risk of individual patients. Hence, this may reduce the risk of iatrogenic complications.
Introduction
Chest injuries post motor vehicle accident (MVA) remains one of the commonest reasons for emergency department visits yearly with estimation of almost 15%–20% of total cases post MVA. 1 Tension pneumothorax is a life-threatening condition which remains an important problem post chest trauma and easily treatable with needle thoracostomy followed by tube thoracostomy. Despite being the mainstay treatment, tube thoracostomy has been linked to several complications, such as tube malposition, estimated around 10% of the cases and other complications such as iatrogenic liver injury, thoracostomy site infection and many more. 2 In this case report, we are highlighting the challenges of a chest tube insertion in a morbidly obese patient which has led to malposition of the tube.
Case report
A 37-year-old male lorry driver presented to emergency department after the lorry he was driving hit a large pothole, skidded and fell into a ravine. The driver was not wearing a seat belt and sustained blunt chest trauma. Assessment by the pre-hospital team showed a Glasgow Coma Scale (GCS) of 8/15 (E1V2M5), blood pressure (BP) of 130/78 mm Hg, heart rate of 110 beats per minute (bpm) and oxygen saturation (SpO2) of 89% on room air. There were features of a left flail chest with pneumothorax and bilateral forearm fracture. He was also suspected to have an intracranial bleed as there was a drop in the GCS. He was put on a cervical collar (C-Collar), given supplementary oxygen 15l/min via high flow mask and his bilateral upper limbs were splinted in view of deformity with open wound.
On arrival to emergency department, patient was triaged to the red zone. Primary survey was immediately initialized. Airway was affected as patient had gurgling sounds with pooling of saliva in the oral cavity. During suctioning, there was absence of gag reflex and continuous pooling of saliva despite suctioning. Assessment of breathing showed reduced chest movement on the left side, with flail segments and massive subcutaneous emphysema. There was deviation of trachea to the right side with SpO2 85% on 15 L/min oxygen. Assessment of circulation showed a BP of 90/48 mm Hg and heart rate of 130 bpm. There was no active external bleeding. GCS on arrival was 8/15 (E1V2M5) with reactive pupil of 3 mm bilaterally. Extended Focused Assessment of Sonography for Trauma (eFAST) was conducted which showed an absent sliding sign at the left lung with the presence of barcode sign. Secondary survey showed deformity with an open wound at the distal forearm bilaterally. The distal circulation of the upper limbs was intact. There was no other deformity noted during secondary survey.
During the ongoing primary survey, patient was intubated for airway protection. In view of reduced air entry at the left chest with hypotension and tachycardia, the diagnosis of tension pneumothorax was made. Needle thoracostomy was performed using 14G angiocath without any difficulty over the safety triangle zone on the left chest. Upon advancement of the needle, there was a hissing sound with improvements in the heart rate (105 bpm) and blood pressure (100/58 mm Hg). In view of suspected internal injuries, two large bore intravenous cannulas were inserted on arrival. Fluid resuscitation was immediately initiated with 500 mL of sodium chloride 0.9% which was completed within 30 min while awaiting for cross-matched blood.
After initial stabilization, decision for chest tube insertion was made for definitive management of his pneumothorax. In view of an obese body habitus with estimated weight of around 130 kg and height of 170 cm (body mass index: 44.9 kg/m2), a thick chest wall was anticipated with an estimated tube depth of 24 cm. Incision of around 7 cm was made over the left safety triangle. Blunt dissection was performed using an artery forceps until the pleural lining was reached. Penetration of the pleura was made with the tip of the artery forceps and a ‘giving way’ sensation was felt. There was no active spurting of blood upon breaching the pleura. A 32Fr chest tube was introduced along the dissected tissues. However, the attempt to guide in the chest tube with artery forceps failed due to the patient’s thick chest wall and massive subcutaneous emphysema. This is despite utilizing adjunct manoeuvres such as abduction of his shoulder joint and flexion of elbow joint. Following failure of multiple attempts via the open method, chest tube insertion was then performed using the trochar with its sharp tip withdrawn slightly to prevent injury. Upon connection of the tube to the underwater seal, air bubble was noted and the chest tube was anchored at 24 cm mark with silk 1/0 suture.
Patient subsequently underwent a contrasted computed topography (CT) imaging of the brain, cervical spine, thorax and abdomen. CT thorax (Figure 1) showed an ectopic chest tube placement as it was seen coursing anterior to the posterior part of the left first rib, transversing the mediastinum posterior to the oesophagus, trachea and left carotid sheath with its distal tip at the right supraclavicular fossa. There were flail segments on the left third to sixth ribs with bilateral lung contusions, pneumopericardium and pneumohemothorax of the left lung with a suspected oesophageal tear. However, there was no contrast leak during the arterial and venous phases of the CT imaging. Upon returning to the emergency department, the chest tube was no longer fluctuating. A repeated chest x-ray showed the tube was dislodged into the subcutaneous tissue. The general surgical and otorhinolaryngology team were called in to assist with bronchoscopy and oesophago-gastro-duodenoscopy (OGDS) which were performed in the emergency department in view of suspected iatrogenic injury. However, there was no evidence of oesophageal or tracheobronchial tree injury.
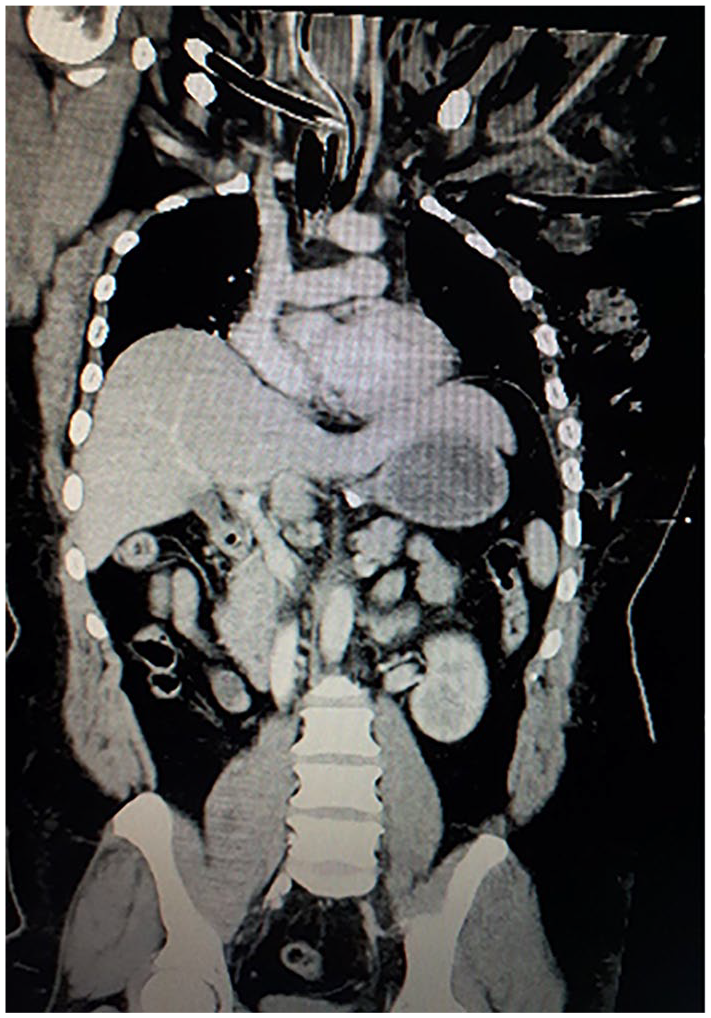
CT image of a thorax showing ectopic chest tube passing through from the left side insertion point to tip on the right supraclavicular region with large subcutaneous emphysema can be seen.
Patient was then admitted to the intensive care unit (ICU) for continuous care of his lung injuries. During the initial 48 h of admission, patient required high ionotropic support and high setting ventilator. There was a multi-disciplinary team discussion among the intensivist, general surgeon and interventional radiologist on options of transferring the patient to a nearby hospital with a cardiothoracic team for removal of chest tube and reinsertion or for removal in the present hospital under CT guidance. However, due to his critical condition, decisions were made to keep the chest tube and stabilize the patient first. He was then reviewed by a visiting cardiothoracic surgeon on day 3 of admission, who promptly removed the ectopic chest tube in ICU. As patient showed improvement with reducing inotropic support and a repeated chest radiograph showed expanded lungs, a new chest tube was not inserted.
On day 6 of ICU admission, in view of a significant amount of persistent subcutaneous emphysema, patient was subjected for a repeat bronchocopy and OGDS which were unremarkable. As the intensivist encountered challenges in weaning off the ventilation, a decision was made to insert a CT-guided chest tube on the eighth day of admission. However, upon repeat of an oral and intravenous contrasted CT abdomen and thorax, there was only a residual small left apical pneumothorax with healing lung contusions. There was also no evidence of contrast leak to suggest any hollow organ injury. In view of these findings as well as gradual improvements in the ventilatory settings, the cardiothoracic surgeon did not reinsert a new chest tube. In the following days, he was able to be weaned off his ventilatory support and extubated on day 11 of admission. He was discharged 3 weeks post trauma upon completion of early rehabilitation for his limb injuries. Patient was reviewed 2 months post trauma and was recovering well with no residual respiratory issues.
Discussion
Chest tube thoracostomy is one of the commonest life-saving procedure performed in the emergency department. It serves to monitor thoracic blood loss, evacuate blood in the pleural cavity, prevent tension pneumothoraces and promote lung re-expansion, thereby tamponading low-pressure pulmonary vessels and improving any respiratory compromise. 3 In literature, the early description of chest tube thoracostomy was done by Hippocrates. The procedure further evolved over the years until Hewitt in 1876 incorporated the usage of underwater seal. 4 Although chest tube insertion was regularly practised during World War II, emergency tube thoracostomy for acute trauma was not widely practised until the Korean war. 4
Despite the familiarity of chest tube insertion among the emergency trainees, the incidence of significant morbidity and occasional mortality unfortunately remains high with around 18%–30% 5 of the total number of cases. Published complications in adult patients include ectopic chest tube, lacerations of the lung, injuries to intercostal artery, oesophagus, stomach, liver, spleen, diaphragm, pulmonary artery, and atrium as well as right ventricular compression. 5 Despite the different types of complications published, ectopic placement of chest tubes remains the commonest 2 complication occurring in approximately 10% of the total number of cases. The incidence is higher in the cases of critically ill patients, 6 obesity and in patients with multiple rib fracture. 2 It was further explained in the literature that the challenge in inserting chest tube for patients with multiple rib fractures with subcutaneous emphysema and obese patients is in the difficulty in identifying the safety triangles of the chest. 7 The mobility of ribs in patients with concurrent rib fractures or flail chest also contributes to this challenge during blunt dissection for chest tube insertion. 8
In this patient, the initial indication for a chest tube insertion was clear as the classical features of tension pneumothorax were present. However, anticipation of a difficult chest tube insertion by having a multidisciplinary team approach prior to insertion with the assistance of radiographic-guidance procedure may have yielded a better outcome. The failure to estimate the depth of the subcutaneous fat and tissue as well as the presence of flail segments may have contributed for the deep chest tube insertion. It should be properly measured with the tip of the chest tube at or around the second intercostal space to the safety triangle. The use of a trochar during insertion may have resulted in the ectopic placement of the tube as well. Improvement in chest tube insertion techniques as well as the ability to identify red flags in chest wall injuries will improve the chances of a safe and successful chest tube insertion. A low threshold in involving radiological aid is recommended in difficult cases.
Any malpositioned chest tube needs to be removed promptly and replaced with a functioning chest tube. 8 There are numerous removal techniques which have been documented in literatures; however, the emphasis has been on the importance of chest tube reinsertion techniques rather than on removal. The techniques considered for our patient were either a CT-guided removal or an open removal technique. Both techniques have merits; however, the choice needs to be decided according to patient’s general condition and the facilities available at the treating hospital. As the treating hospital does not have cardiothoracic surgical expertise and it was hazardous to transfer an unstable patient to the nearest cardiothoracic facility, a decision was made to remove and reinsert the chest tube under CT guidance. Another consideration for this decision was the risks of coagulopathy and acidosis post polytrauma which were significant at that time. This may have led to uncontrollable haemmorhage during a blunt dissection and exploration and may harm the patient even more.
In literature, there are various methods which can be used to improve chest tube insertion in difficult cases. One of the commonest methods that have been widely used worldwide is the open method. However, despite being relatively safe, study has shown it is not faultless. 9 Methods, such as a video assisted thoracostomy or CT-guided thoracostomy, were considered in our patient during his stay in ICU to facilitate insertion directly into the pocket of pneumothorax and subcutaneous emphysema. However, it was not conducted as patient has improved conservatively. The main issues encountered for both these methods are the lack of resources and facilities in most of the hospitals in Malaysia as well as the time delay during transfer to a readily equipped centre, which are important considerations in cases such as a massive haemothorax and tension pneumothorax. Ultrasound (US) can be used as a guide as well during chest tube insertion whereby real-time imaging can help in detecting the movement of the chest tube in the intrapleural region. 10 Unfortunately, usage of US-guided chest tube insertion is limited by the operator’s skill set and not suitable for patients with a thick chest wall. Bougie-assisted chest tube insertion has been suggested in a study for patients that are suspected of having a difficult chest tube insertion. 11 However, further studies need to be conducted prior to validation of this technique.
A peculiarity in this patient was the ventilatory improvements despite there were no reinsertion of chest tubes. Multiple studies have shown a significant sized pneumothorax with positive pressure ventilation (PPV) do require chest tube insertions. Failure of insertion may cause tension pneumothorax which may lead to mortality if left untreated. However, there were arguments on requirements of chest tube thoracostomy for occult pneumothorax with PPV. An initial study by Enderson et al. 12 in 1993 described the reference points used by clinicians to come upon a decision that a chest tube insertion is indicated in all pneumothoraces with PPV regardless of size. However, Brasel et al. 13 in 1999 have proved not all ventilated pneumothoraces need chest tubes. Furthermore, it is valuable to note that the study conducted by Enderson was carried out in an operating theatre, while Brasel et al. performed theirs in a critical care setting. Ventilation strategies, in general, have also changed substantially over the past decade. Decreased airway pressures and tidal volumes are now routine in the critically ill patients. Contemporary ventilatory management stresses more attention to controlling the peak and mean airway pressures, limiting the pressure below than the level suggested in previous routine. 14 In our patient, insertion of initial needle thoracostomy may have led to release of air leak caused by the flail chest. During the initial CT thorax with the malpositioned chest tube, only a small pneumothorax was found. Despite being on PPV subsequently, the patient did not develop tension pneumothorax, which further justified the decision for conservative management. As repeated chest radiographs and the CT thorax showed gradual resolution of the pneumothorax with an overall clinical improvement of the patient, a reinsertion of a chest tube was unnecessary and may even cause more harm.
Conclusion
Chest tube insertion is a vital procedure in traumatic chest tube injuries. Despite being the mainstay of management for tension pneumothorax, recognition of the factors associated with a difficult chest tube thoracostomy is equally important to reduce the risks of iatrogenic complications related to chest tube insertion. Thus, following a standard chest tube insertion protocol that has been tailored to the Hospitals’ resources and facilities may minimize the risks of procedure-related mortality and morbidity.
Footnotes
Acknowledgements
The authors would like to express their deepest gratitude to the patient for the cooperation and consent. Many thanks to Selayang Hospital for providing the platform to investigate and treat the patient.
Authorship
S.A.K.M.S. is the main author. I.M.S. and M.A.A. are the co-authors.
Author contributions
All authors were involved in majority of writing this article which includes the patient summary, literature search and the discussion.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This study did not involve in patient’s management and treatment.
Informed consent
The patient filled and signed in separate document and obtained.