
Abstract
Background:
The treatment of benign paroxysmal positional vertigo (BPPV) has not been well studied. Many clinicians are indifferent about canalith reposition maneuvers and frequently prefer medical treatments.
Objectives:
We aimed to detect efficacy of Epley maneuver in relieving symptoms of benign paroxysmal positional vertigo patients diagnosed in emergency department and if medical treatments are useful in patients whose symptoms were not relieved.
Methods:
The study was conducted as a prospective cohort study in the emergency department of a tertiary hospital. Patients who were over 18 years of age and presented to emergency department with complaints of vertigo symptoms and nausea and had a positive Dix–Hallpike test were included in the study. Patients’ demographic data, possible etiological factors, affected ear, and benign paroxysmal positional vertigo diagnosis in the history were recorded on the study data form. The European Evaluation of Vertigo scale and the Visual Analogue Scale (VAS) score of nausea and vertigo symptoms were graded and recorded for each patient before and after treatment.
Results:
Ninety patients were included in the study in total. Epley maneuver was carried out to all patients. Vertigo symptoms VAS (VASd) score (p < 0.001), nausea and vomiting VAS (VASnv) score (p < 0.001), and European Evaluation of Vertigo scale score (p < 0.001) of all patients showed a statistically significant decrease after Epley maneuver. A combination of dimenhydrinate and metoclopramide helped to reduce VASd (p = 0.048), VASnv (p = 0.031), and European Evaluation of Vertigo scale scores (p = 0.001) at a statistically significant level more than dimenhydrinate treatment alone.
Conclusions:
Epley maneuver may be applied to every patient with benign paroxysmal positional vertigo. Dimenhydrinate and/or metoclopramide helps to control patients’ symptoms whose symptoms remain despite Epley maneuver.
Introduction
Vertigo is an action illness occurring as a result of sudden movement due to the incoordination of the inputs from these systems in which either the person or their surrounding revolves.1,2 The most frequent three reasons for vertigo are acute peripheral vestibulopathy (vestibular neuritis, labyrinthitis), Meniere’s disease, and benign paroxysmal positional vertigo (BPPV). 3 The lifetime prevalence of BPPV is 2.4%; 4 5.6 million people present to hospital with the complaint of dizziness in the United States every year, and 17%–42% of them are diagnosed with BPPV; 5 3% of all emergency department (ED) visits are due to dizziness. 6
BPPV occurs when the small calcium carbonate crystals (otoliths) in the utricle separate from the macula and fall into one of the semi-circular canals. Due to their anatomical localization, otoliths most frequently fall into the posterior canal. 7 This situation, in turn, causes dizziness, nausea, vomiting, sweating, and nystagmus. BPPV is diagnosed via medical history, physical examination, and Dix–Hallpike (DH) test. After the diagnosis, canaliths should be relocated from where they are to where they should be located with the canalith reposition maneuver.7,8 The most frequently used maneuver is Epley maneuver. The first management of BPPV is not a medical treatment, but the application of canalith reposition techniques. There is not any evidence that supports any medical treatment is as effective as canalith reposition maneuvers.8,9,10,11 However, many clinicians are indifferent about these maneuvers and frequently prefer medical treatments. 12
We aimed to detect the efficacy of Epley maneuver in relieving symptoms of BPPV patients diagnosed in ED and if medical treatments are useful in patients whose symptoms were not relieved.
Materials and methods
Study plan. The
Study population. Patients who were over 18 years of age and presented to ED with complaints of vertigo symptoms and nausea and who had a positive DH test and/or BPPV diagnosis were included in the study. The diagnostic criteria accepted for BPPV are 1 vertigo associated with a characteristic mixed torsional and vertical nystagmus provoked by the DH test, 2 a latency between completion of the DH test and the onset of vertigo and nystagmus, 3 paroxysmal nature of the provoked vertigo and nystagmus, and 4 fatigability. The exclusion criteria were as follows: Patients with focal neurologic deficits, central vertigo, pregnancy on admission, allergy history of the medications to be used in the study, and taken any medicine that can affect the result of the study (antipsychotics, antidepressants, opioids, antihistamines) in the last 24 h. Ninety patients who met the criteria between June 1, 2018, and December 31, 2018, were included in the study. The informed consent of the patients was obtained.
Collection of data and the study protocol
Patients’ demographic data, possible etiological factors, and effected ear were recorded on the study data form. The European Evaluation of Vertigo (EEV) scale was recorded for each patient before treatment. 13 Moreover, in order to determine the degree of nausea and vertigo symptoms, the Visual Analogue Scale (VAS) scoring between 0 and 10 was used. The patients were asked to mark a dot to define the severity of the symptom. VAS scores for nausea and vertigo symptoms were recorded separately before the treatment. DH and Epley maneuvers were carried out by physicians with 5 years of emergency medicine specialization training. All the physicians were received standardized training in the maneuver before the study. Epley maneuver was carried out to all patients; 30 min after Epley maneuver was performed, EEV scale, vertigo symptoms VAS score, and nausea VAS score were recorded. Patients whose symptoms were relieved and telling the provider that he or she felt well were discharged; 100 mg of dimenhydrinate was infused intravenously to the patients whose vertigo symptoms, nausea, and vomiting persisted clinically. Patients were re-evaluated 30 min later. Patients whose symptoms were relieved were discharged after their VAS scores, and EEV scales were graded and recorded; 10 mg of metoclopramide was infused intravenously to patients with maintaining symptoms. VAS scores and EEV scales were graded and recorded 30 min after patients’ medical treatments were completed.
Patients were divided into three groups according to the response to the treatment received. Group 1, patients whose symptoms were relieved with only Epley maneuver; Group 2, patients whose vertigo symptoms, nausea and vomiting were not relieved with Epley maneuver and who received intravenous dimenhydrinate after Epley maneuver; Group 3, patients whose symptoms still remained after Epley maneuver and dimenhydrinate thus intravenous metoclopramide was added to their treatment. Flow chart of the patients included in the study is given in Figure 1.
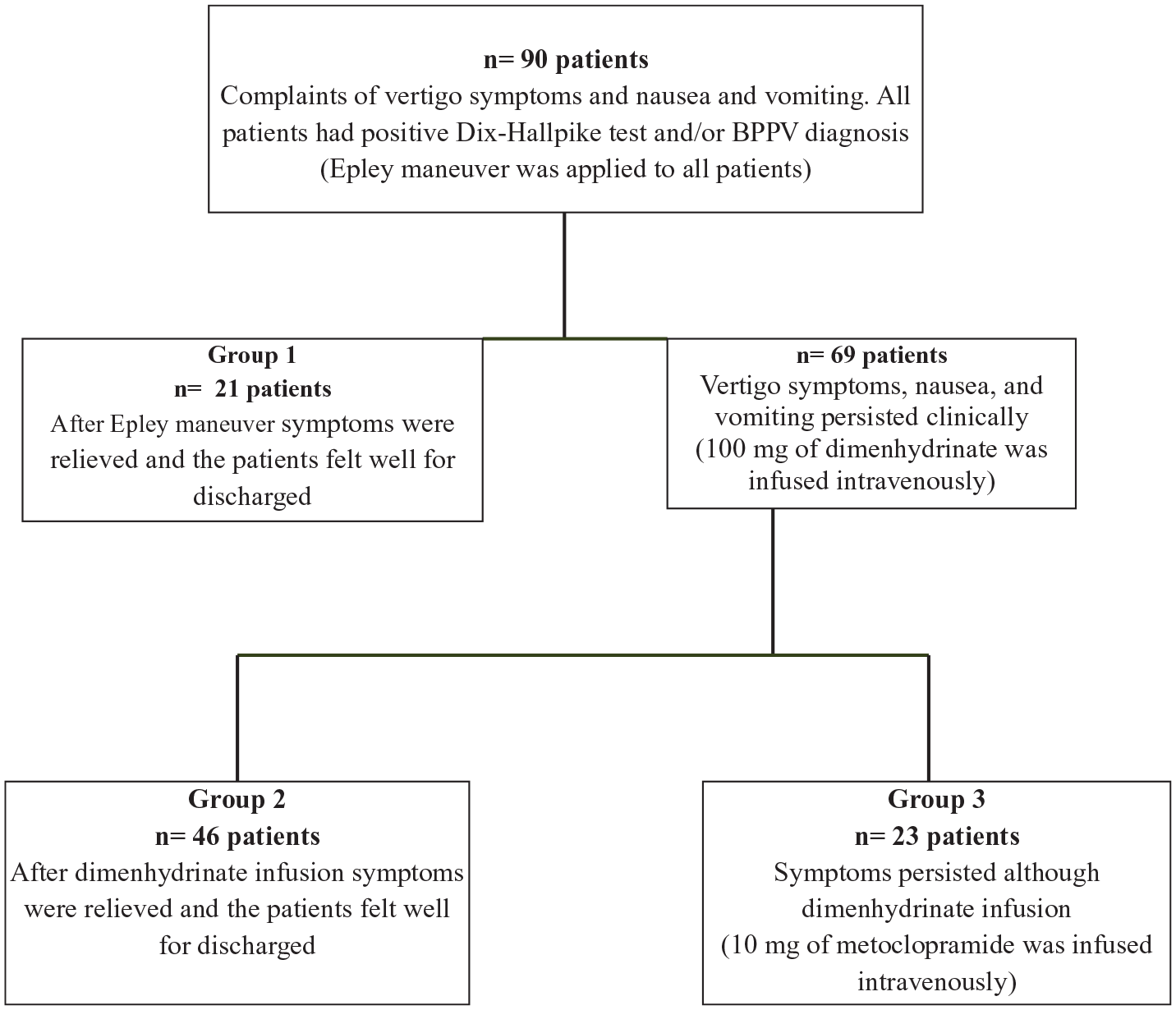
Flow chart of the patients included in the study.
Primary outcome. Relief of the patients’ symptoms (decrease in VAS and EEV scores) after Epley maneuver was accepted as the primary outcome. Secondary outcome is to ascertain the efficacy of single or combined medical treatment on the relief of symptoms.
Statistical analysis. Data were analyzed via IBM SPSS V22. Categorical data were presented as frequency (percentage); quantitative data were presented as mean ± standard deviation and median (min.–max.). These data were compared through chi-square, t-test (variables with normal distribution). Groups were compared through the analysis of variance (ANOVA) method in terms of repetitive measurements (nausea and vertigo symptoms VAS scores, EEV scale scores) Post hoc tests were conducted in order to compare groups within themselves. Statistical significant level was accepted as p < 0.05 in all statistical analyses.
Results
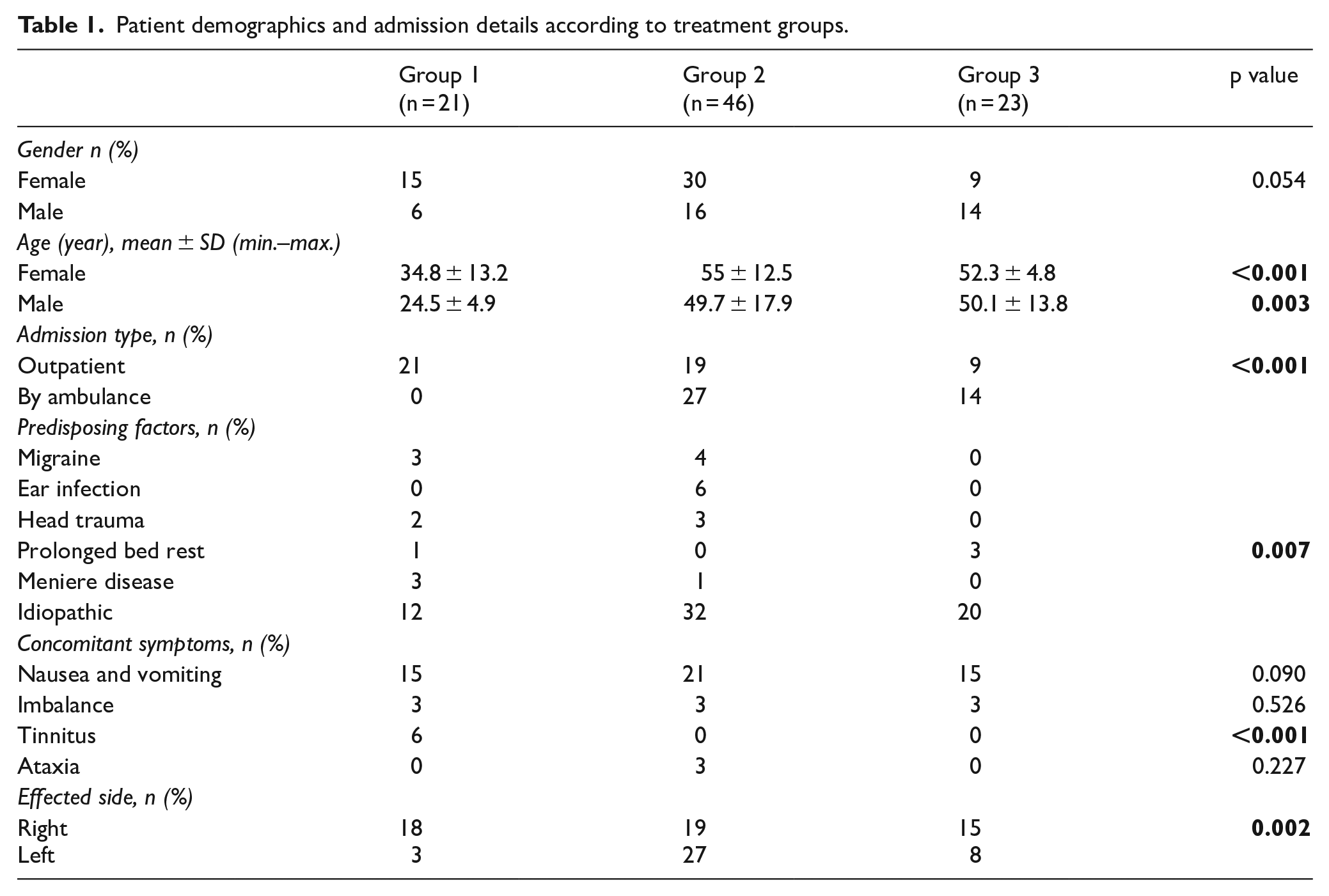
Ninety patients were included in the study in total; 60% of the patients (n = 54) were female and40% of them were (n = 36) male. The mean age of women was 48.9 ± 14.6, the men was 45.7 ± 17.4, and there was no statistically significant difference between genders regarding age (p = 0.338); 81.1% of patients (n = 73) presented to the hospital within the first 24 h of the onset of symptoms, and 55.6% of them (n = 50) were previously diagnosed with BPPV. According to the response to the treatment received, 23.3% of them (n = 21) were in Group 1, 51.1% of them (n = 46) were in Group 2, and 25.6% of them (n = 23) were in Group 3. Characteristics of the patients according to the treatment groups are given in Table 1.
Patient demographics and admission details according to treatment groups.
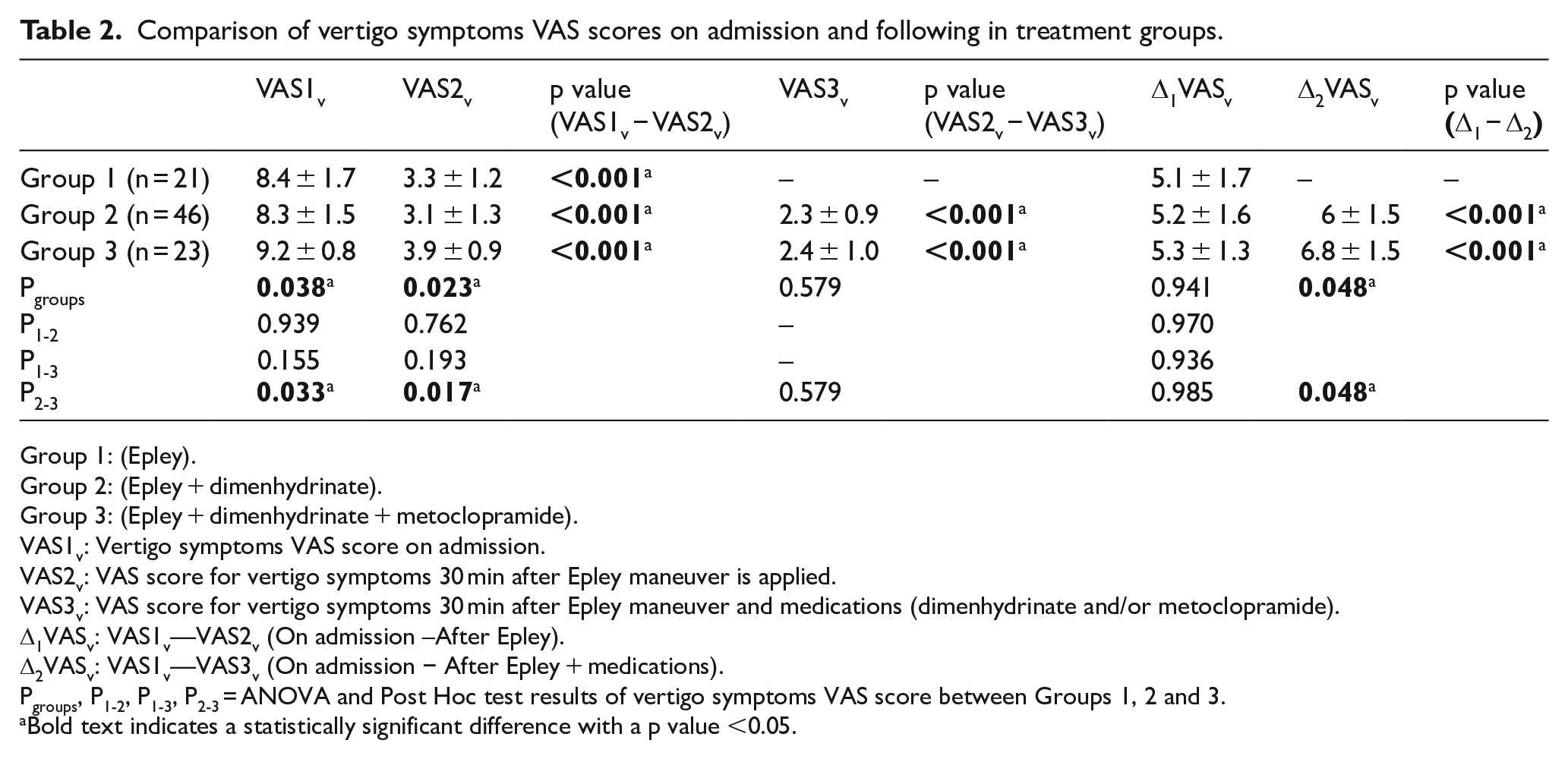
VAS score was used in the evaluation of response to the treatment of patients’ vertigo symptoms. Treatment groups’ comparison of vertigo symptoms VAS scores (VASv) on admission time and after the treatments are given in Table 2. The highest VASv on admission belongs to Group 3, and there was a statistically significant difference among groups (p = 0.038). VASv of all patients showed a statistically significant decrease after Epley maneuver (p < 0.001). When groups were compared, there was no statistically significant difference between Groups 1 and 2 (p = 0.762) and Groups 1 and 3 (p = 0.193). Δ1VASv result was calculated by the mathematical difference between VASv scores on admission (VAS1v) and VASv after Epley maneuver (VAS2v). There was no statistically significant difference among groups in Δ1VASv (p = 0.941). Δ2VASv result was calculated by the mathematical difference between VAS1v and dizziness VAS score after Epley maneuver and medical treatment (VAS3v). There was a statistically significant difference between Δ2VASv of Groups 2 and 3 (p = 0.048). A combination of dimenhydrinate and metoclopramide helped to reduce VASv at a statistically significant level more than dimenhydrinate treatment alone (Table 2).
Comparison of vertigo symptoms VAS scores on admission and following in treatment groups.
Group 1: (Epley).
Group 2: (Epley + dimenhydrinate).
Group 3: (Epley + dimenhydrinate + metoclopramide).
VAS1v: Vertigo symptoms VAS score on admission.
VAS2v: VAS score for vertigo symptoms 30 min after Epley maneuver is applied.
VAS3v: VAS score for vertigo symptoms 30 min after Epley maneuver and medications (dimenhydrinate and/or metoclopramide).
Δ1VASv: VAS1v—VAS2v (On admission –After Epley).
Δ2VASv: VAS1v—VAS3v (On admission − After Epley + medications).
Pgroups, P1-2, P1-3, P2-3 = ANOVA and Post Hoc test results of vertigo symptoms VAS score between Groups 1, 2 and 3.
Bold text indicates a statistically significant difference with a p value <0.05.
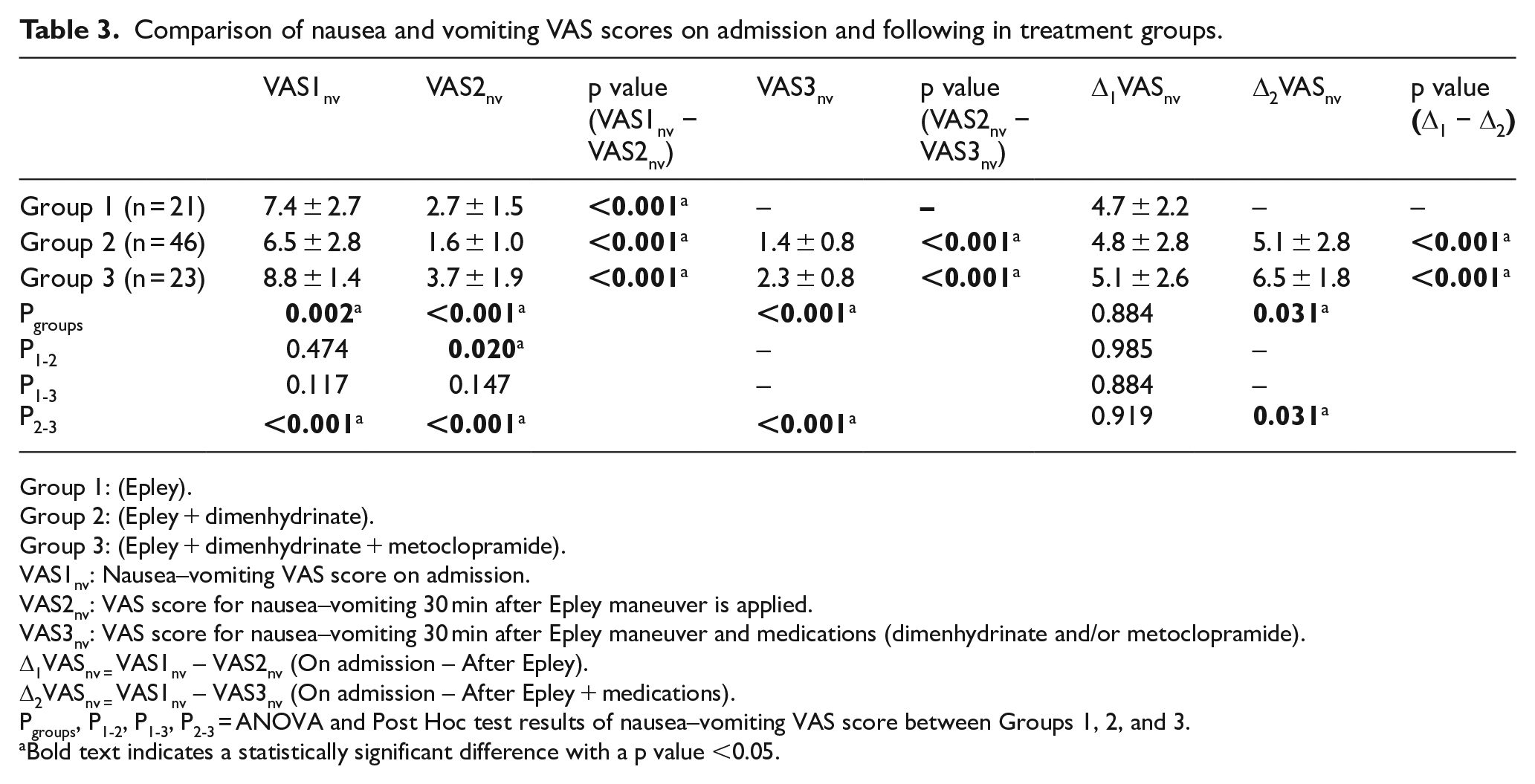
VAS score was used to evaluate the treatment response of patients’ nausea and vomiting. Treatment groups’ comparison of nausea, vomiting VAS scores (VASnv) on admission and after the treatment is given in Table 3. The highest VASnv on admission belongs to Group 3, and there was a statistically significant difference among groups (p = 0.002). VASnv of all patients showed a statistically significant decrease after Epley maneuver (p < 0.001). Δ1VASnv result was calculated by the mathematical difference between VASnv on admission (VAS1nv) and VASnv after Epley maneuver (VAS2nv). The lowest VAS2nv belonged to Group 2 with 1.6 ± 1.0. There was no statistically significant difference among groups in Δ1VASnv (p = 0.884). Δ2VASnv result was calculated by the mathematical difference between VAS1nv and nausea vomiting VAS score after Epley maneuver and medical treatment (VAS3nv). There was a statistically significant difference between Δ2VASnv of Groups 2 and 3 (p = 0.031). Combination of dimenhydrinate and metoclopramide helped to reduce VASnv with a statistically significant level higher than dimenhydrinate treatment alone (Table 3).
Comparison of nausea and vomiting VAS scores on admission and following in treatment groups.
Group 1: (Epley).
Group 2: (Epley + dimenhydrinate).
Group 3: (Epley + dimenhydrinate + metoclopramide).
VAS1nv: Nausea–vomiting VAS score on admission.
VAS2nv: VAS score for nausea–vomiting 30 min after Epley maneuver is applied.
VAS3nv: VAS score for nausea–vomiting 30 min after Epley maneuver and medications (dimenhydrinate and/or metoclopramide).
Δ1VASnv = VAS1nv – VAS2nv (On admission – After Epley).
Δ2VASnv = VAS1nv – VAS3nv (On admission – After Epley + medications).
Pgroups, P1-2, P1-3, P2-3 = ANOVA and Post Hoc test results of nausea–vomiting VAS score between Groups 1, 2, and 3.
Bold text indicates a statistically significant difference with a p value <0.05.
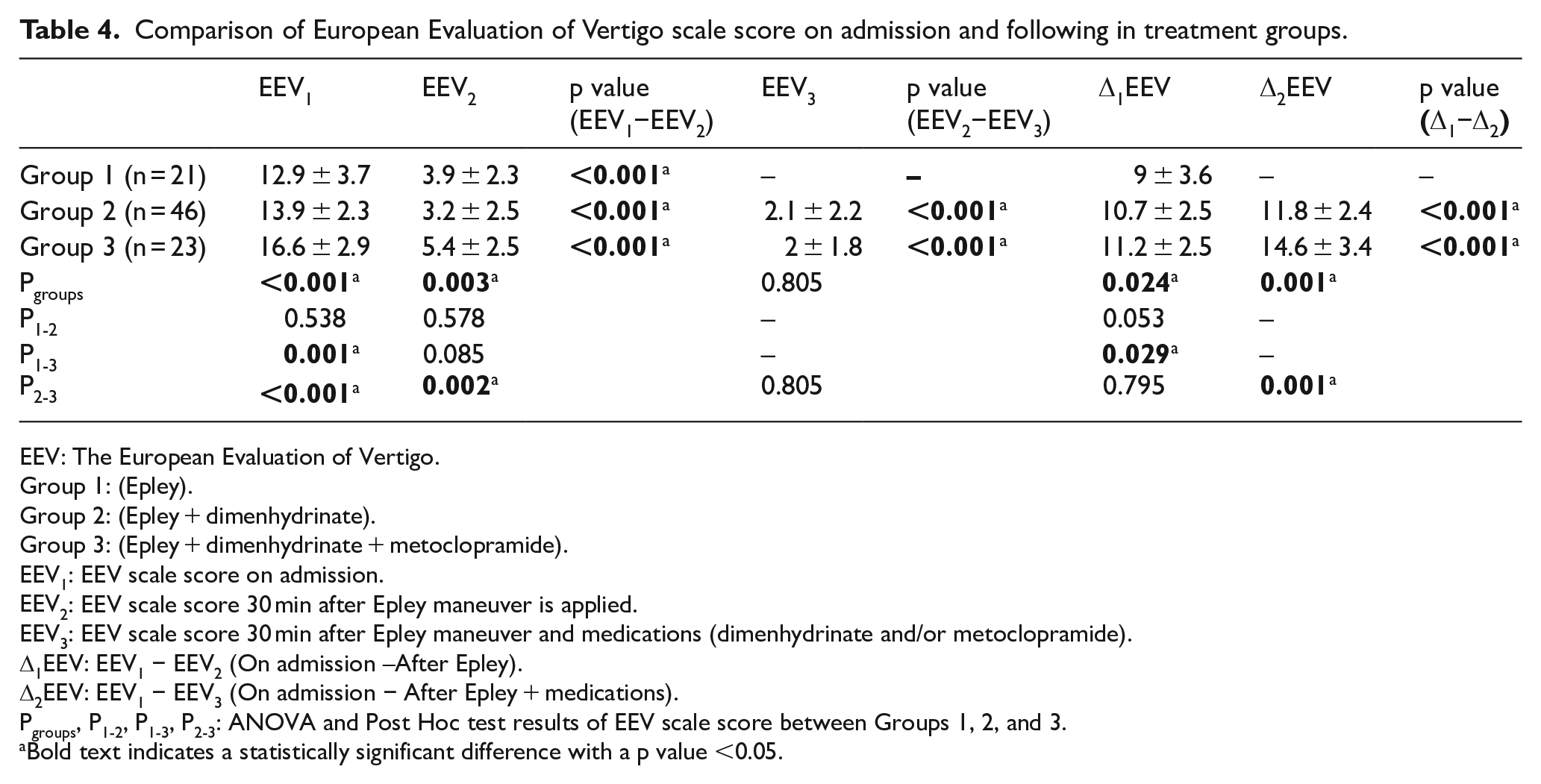
EEV scale was used in the evaluation of patients’ treatment response. Treatment groups’ comparison of EEV scales on admission and after the treatment is summarized in Table 4. According to this, there was a statistically significant difference among groups in terms of the EEV score on admission (EEV1) (p < 0.001). When groups were compared, there was a statistically significant difference between Groups 1 and 3 (p = 0.001) and Groups 2 and 3 (p < 0.001). The EEV score of all patients showed a statistically significant decrease after Epley maneuver (p < 0.001). When groups were compared to each other, post-Epley maneuver scores (EEV2) of Groups 2 and 3 showed a statistically significant difference (p = 0.002). Group 3 had higher EEV2 score. EEV3, which was scored after medical treatment, did not show a statistically significant difference between the groups received medical treatment (p = 0.805). This shows to the combination of metoclopramide and dimenhydrinate eliminated the statistical significant difference of between EEV scores. Δ1EEV result was calculated by the mathematical difference between EEV1 and EEV2. There was a statistically significant difference between Δ1EEV of Groups 1 and 3 (p = 0.029). Δ2EEV was calculated by the mathematical difference between EEV1 and EEV3. There was a statistically significant difference between Δ2EEV of Groups 2 and 3 (p = 0.001). A combination of dimenhydrinate and metoclopramide helped to reduce the EEV score at a statistically significant level higher than dimenhydrinate treatment alone (Table 4).
Comparison of European Evaluation of Vertigo scale score on admission and following in treatment groups.
EEV: The European Evaluation of Vertigo.
Group 1: (Epley).
Group 2: (Epley + dimenhydrinate).
Group 3: (Epley + dimenhydrinate + metoclopramide).
EEV1: EEV scale score on admission.
EEV2: EEV scale score 30 min after Epley maneuver is applied.
EEV3: EEV scale score 30 min after Epley maneuver and medications (dimenhydrinate and/or metoclopramide).
Δ1EEV: EEV1 − EEV2 (On admission –After Epley).
Δ2EEV: EEV1 − EEV3 (On admission − After Epley + medications).
Pgroups, P1-2, P1-3, P2-3: ANOVA and Post Hoc test results of EEV scale score between Groups 1, 2, and 3.
Bold text indicates a statistically significant difference with a p value <0.05.
With the applied treatment protocols, there was not any need to hospitalize any of the patients; all patients were discharged from the ED.
Discussion
Our study evaluated the efficacy of the Epley maneuver, which is the most frequently used BPPV treatment in the ED, and whether certain medications were also beneficial in the management of this condition. Although dimenhydrinate use in addition to Epley maneuver is a frequently preferred protocol, a similar study advising metoclopramide use in addition to this combination in patients with severe symptoms could not be found in the literature. In our study, symptoms of all patients were relieved in statistically significant level. A combination of dimenhydrinate and metoclopramide is more effective at a statistically significant level than only dimenhydrinate treatment in patients with high VAS and EEV scores whose symptoms remain despite Epley maneuver. All patients, including those with severe symptoms, were discharged from ED after Epley maneuver, dimenhydrinate, and metoclopramide treatment, respectively.
BPPV is a common complaint in patients presenting to the ED among all ages. 14 The frequency of BPPV increases in advancing age. The prevalence of BPPV is 7.4% between the ages of 18 and 79 years. 15 Previous studies have shown that BPPV is seen more frequently in women and in elder patients.16,17 It was shown that aging causes a tendency toward developing BPPV due to degenerative changes resulting in otoconial separation. 16 Similarly, BPPV was more frequently seen in women patients who were older than 40 years in our study as well. The etiological cause cannot be detected in half of the cases. Vestibular neuritis, viral labyrinthitis, head trauma, migraine history, prolonged bed rest, Meniere’s disease, inner ear operations, hypertension, hyperlipidemia, and aging are within predictable predisposing factors;4,7 71% of cases were idiopathic in our study as well.
The posterior canal is the most frequently affected canal in BPPV, and the right posterior canal is effected predominantly since patients often lie on their right. 18 Determination of the effected side is based on whichever side has more intense amplitude of nystagmus in DH test or whichever side causes dizziness more severely when the patient rolls on his or her back. 7 The right ear was affected in 57.8% of the cases in our study.
Epley maneuver is a considerably effective method in relieving symptoms of BPPV, and it is advised to be applied before medical treatment as the first step of treatment. 10 However, repositioning maneuvers are still not performed by most of the clinicians. 12 In a meta-analysis on the efficacy of Epley maneuver, it has been shown that Epley maneuver is effective and has 6.5 times more chance of improving their clinical symptoms and the likelihood of having a negative Dix–Hallpike (DH) test is 5 times greater in patients who had the Epley maneuver performed than in those who did not. 19 Epley maneuver was tested in a large number of randomized placebo-controlled studies; its success rate was shown between 32% and 90% even in a single application. 7 In a study where canalith reposition maneuvers were performed on 965 patients in BPPV treatment, symptoms of 85% of patients were relieved in a single reposition maneuver; more than three maneuvers were performed only in 2% of the cases. 20 In our study, an Epley maneuver was performed in all cases, and statistically significant relief was observed in all of the patients. While 23.3% of the cases were discharged with only Epley maneuver, additional medicine was needed in 76.7% of them. Since the tendency of BPPV’s spontaneous relief after Epley maneuver has been known, the administration of post-maneuver medications may improve Epley maneuver’s tendency to relieve symptoms. 21 However, current enormous admissions to the ED did not allow the physicians to follow patients for long hours to see Epley’s maneuver effect in our study. The reason why the medication rate is so high might be the concern for reducing the ED crowd.
Epley maneuver is the most effective treatment method for patients with BPPV. In addition to this, patients complain about residual symptoms even after a successful Epley maneuver. 22 Medications used in addition to Epley maneuver are vestibular suppressant and antiemetic. 23 Dimenhydrinate fundamentally affects the vestibular system through inhibition of histamine and cholinergic receptor functions in the vestibular nucleus and vomiting center. 24 Metoclopramide, however, shows its antiemetic effect through dopamine receptor antagonism in the chemoreceptor trigger zone. It does a negligible sedative effect. 25 In a study conducted on the effect of vestibular suppressant agents after canalith reposition maneuver, it has been shown that dimenhydrinate treatment following a successful maneuver may help to alleviate residual complains. 22 It was shown in a conducted study that the combination of metoclopramide and dimenhydrinate is more effective than the usage of these drugs individually in the treatment of postoperative nausea and vomiting. 26 In our study, the usage of dimenhydrinate and metoclopramide on BPPV treatment arose due to the need of symptomatically alleviating dizziness and nausea, which are cardinal symptoms of vertigo; 30 min after Epley maneuver 23.3% of patients, 60 min after Epley and dimenhydrinate treatment 74.4% of patients, and 90 min after Epley, dimenhydrinate, and metoclopramide treatment, the rest of the case were discharged from ED. In ED where patient density is high, 30 min of follow-up after Epley maneuver, and using supportive medication when necessary, it will shorten the waiting duration in the ED. Feeling of dizziness and nausea might maintain in especially elderly and anxious patients due to underlying disorders and predisposing factors despite an effective reposition maneuver.27,28 In these patients, supportive medications may improve patient comfort by taking symptoms under control.
Limitations
There are some limitations to our study. About our study population, a larger sample size and stronger power would allow us to identify more subtle differences in treatment efficacy between the Epley maneuver and medications.
One primary endpoint of the study was the subjective patients whose telling to the doctor that he or she felt well were discharged. These patients ambulation was required to allow discharge to home, although mild symptoms of vertigo might still exist. Another limitation of the study was the evaluation of vertigo patients initially and then after only period of 30–90 min. The 30-min period was used to prevent the ED patient from waiting longer for rescue medicine to be administered, during this uncomfortable and often debilitating condition. The symptoms of these patients should be followed longer but the emergency crowd does not allow it. Also, another limitation is no follow-up of patients after leaving the ED.
For a better comparison of the effectiveness of the Epley maneuver, a group of patients could receive medication(s) first and then underwent the Epley maneuvers, or compare the difference of the two groups “with Epley” and “without Epley.”
Conclusion
As a result, an Epley maneuver is such a maneuver that may be applied to every patient with BPPV quickly in ED. While the data suggest that the patients felt symptomatically improved after the Epley maneuvers, this improvement was apparently not enough to facilitate a discharge in the majority of patients. It could be said that some patients may need medications following Epley maneuver for complete relief of symptoms.
Highlights
Epley maneuver is such a maneuver that may be applied to every patient with BPPV quickly in emergency department. Some BPPV patients may need medications following Epley maneuver for complete relief of symptoms.
Our study evaluated the efficacy of the Epley maneuver, which is the most frequently used BPPV treatment in the ED, and whether certain medications were also beneficial in the management of this condition.
Although dimenhydrinate use in addition to Epley maneuver is a frequently preferred protocol, a similar study advising metoclopramide use in addition to this combination in patients with severe symptoms could not be found in the literature.
Footnotes
Author contributions
All authors read the manuscript and agreed to the content and data. All authors played a significant role in the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Approval from an ethical review board of the hospitals was obtained before commencing the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data and materials are reachable from hospital automation information systems.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Human rights
This manuscript was carried out in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines.