
Abstract
Introduction:
Acute pulmonary embolism is the leading cause of cardiovascular mortality in which only 7% of total suspected cases were correctly diagnosed. Prompt diagnosis is essential to reduce disease burden. 12-lead electrocardiography has become standard of examination in any acute cardiovascular setting. Several abnormalities associated with right ventricular dysfunction include the classic McGinn-White and anterior leads T-wave inversion pattern due to conduction abnormalities. Nevertheless, studies conducting research in evaluating diagnostic values of both patterns have not come to definite conclusion. This review evaluates the diagnostic value of T-wave inversions in anterior leads difference compared to that of McGinn-White sign in patients with suspected acute pulmonary embolism.
Methods:
Literature searching was conducted from medical databases. Inclusion-exclusion criteria and study eligibility were assessed to select the included studies in this systematic review. Three final articles were selected and critically appraised using the Oxford Center of Evidence-Based Medicine appraisal tools for diagnostic study.
Results:
Considering the compared importance of selected studies, T-wave inversion shows better specificity (90.9% vs 88.7%) and sensitivity (35.5% vs 28.9%) although both signs exhibit minor impact in terms of sensitivity index. Analyses suggest higher averaged accuracy (accuracy index) and Youden index found in T-wave inversion than that of McGinn-White sign (accuracy index: 57.97% vs 56.16%; Youden index: 0.16 vs 0.12), providing more meaningful diagnostic value. Furthermore, anterior leads T-wave inversion possesses better diagnostic odds ratio than that of McGinn-White sign (5.52 vs 3.17).
Conclusion:
Anterior lead T-wave inversions present better diagnostic value than that of classic pattern of McGinn-White sign in electrocardiographic presentation of suspected acute pulmonary embolism.
Introduction
Acute pulmonary embolism (PE) is one of the leading causes of cardiovascular mortality accounting to overall incidence up to 200 out of 100,000 cases of chest pain. 1 Moreover, only 7% of total suspected cases were correctly diagnosed with acute PE before death. 2 Its nonspecific clinical presentations ranging from atypical chest pain, dyspnea, and syncope increases the difficulty in diagnosing PE as it can be easily misdiagnosed with other acute cardiovascular disease and thus delay in the initiation of life-saving treatments. 3 Hence, prompt diagnosis is essential to reduce disease burden. Although CT pulmonary angiography (CTPA) is the preferred supporting examination as definitive tool in diagnosing acute PE, 12-lead electrocardiography (ECG) has become initial standard of examination in any acute cardiovascular setting. 3
ECG has become predominant supporting examination in exhibiting differential diagnosis of acute cardiovascular examination, especially PE. Variations of ECG abnormalities associated with right ventricular (RV) dysfunction followed by rapid RV pressure overload have known to be of diagnostic value for pulmonary thromboembolism. The most common findings are sinus tachycardia (42.2%) and any ST-T segment changes (68.2%). 1 The classic “S1Q3T3” McGinn-White pattern is the well-known pathognomonic sign in acute PE, which is based on pathophysiology of electrical conduction abnormalities in RV strain due to pressure overload but not seen in all acute PE cases. Heterogeneity of ventricular strain in PE could also be shown as T-wave inversion pattern of anterior leads. Variations of studies conducting research in evaluating sensitivity and specificity values of both patterns have not come to definite conclusion.2,3 Therefore, this review aims to evaluate the diagnostic value of T-wave inversions in anterior leads difference compared to that of McGinn-White sign in patients with suspected acute PE.
Methods
Search strategy
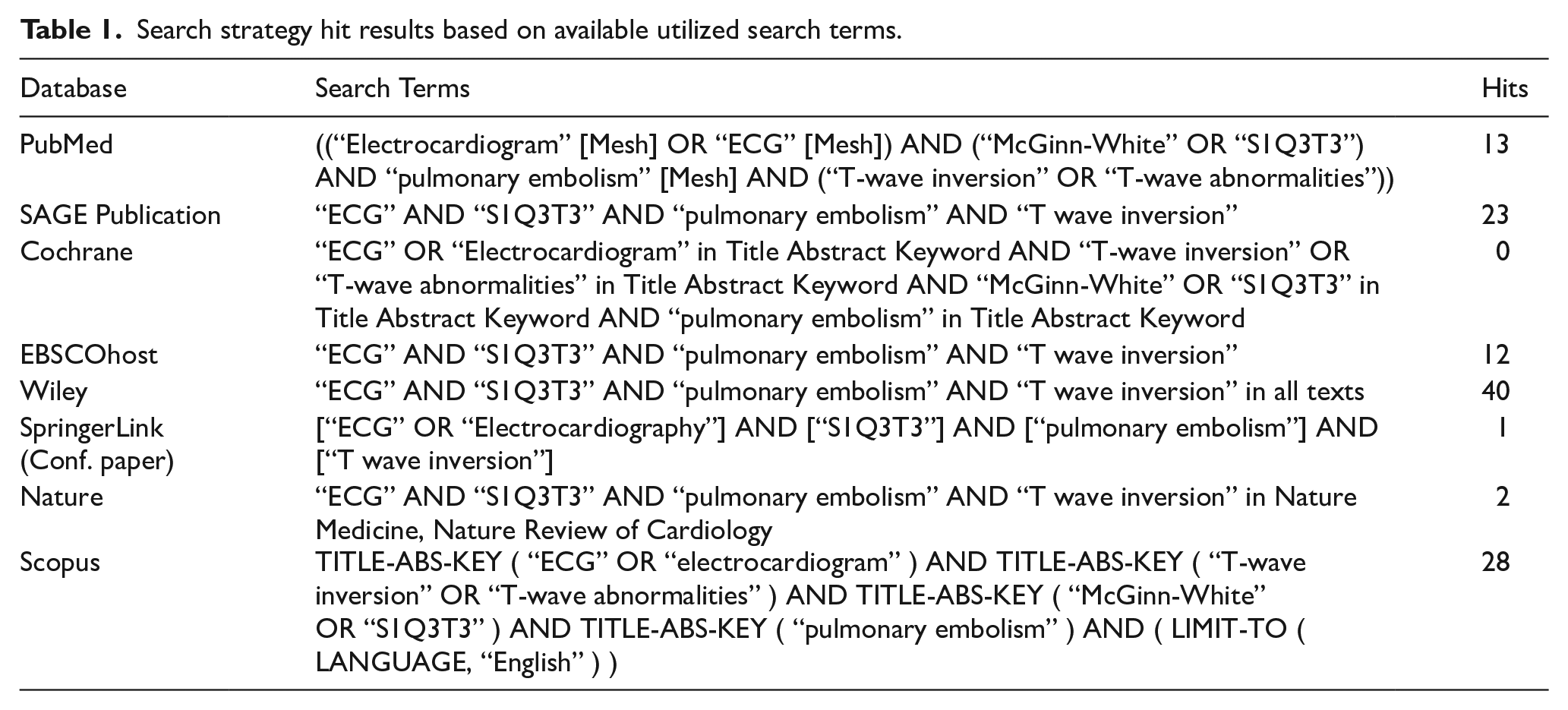
The search was done on March 2020. Eight databases were used, including PubMed, Scopus, and Cochrane Library using terminology listed in Table 1. The utilized keywords for literature searching are previously listed. Search strategy is summarized in the following Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) flowchart.
Search strategy hit results based on available utilized search terms.
Eligibility criteria
Studies involving adult patients aged > 18 years old who were pre-diagnostically examined with ECG prior to computed tomography pulmonary angiography (CTPA) were systematically included. Preferred type of study would be either prospective or retrospective cohorts comprising PE and non-PE diagnosis grouping following initial 12-lead ECG recording. Studies that involve patients with other cardiorespiratory comorbidities (e.g. pulmonary hypertension, congenital heart disease) were excluded, as well as studies older than 5 years old. The obtained search results were screened via title and abstract skimming, double-checked for full-text availability, and finally selected based on inclusion-exclusion criteria.
Critical appraisal
The eligible studies were appraised using the Critical Appraisal for Diagnostic Studies checklist from www.cebm.net, developed by Oxford University. 4 Critical appraisals for all selected articles were conducted by two authors independently to ensure unbiased assessments. Ad hoc piloted forms were used to extract data and assess risk of bias. Results of the critical appraisal were then discussed by both authors to achieve unanimous consensus conducted on this systematic review and meta-analysis.
Data extraction
Data extraction from the selected articles included authorships, study year and design, population characteristics (age and treatment they received), population size, and chosen diagnostic modalities. Furthermore, results of ECG abnormalities were tabulated with variables comprising anterior leads T-wave inversions and McGinn-White sign based on PE and non-PE groups. Values of result prevalence were transposed into tables to aid the diagnostic calculation of sensitivity and specificity, as well as interstudy forest plot comparison, via Review Manager 5.3 and Microsoft Office Excel software. Random-effects model was used to pool extracted data in the meta-analysis with 95% confidence intervals and odds ratios. Statistical heterogeneity was assessed using overall effect Z-score.
Results
Search selection
A comprehensive search was done using eight different journal databases. All search terms are provided in Table 1. To increase the specificity of this study, all studies concerning ECG presentation of acute PE in adult patients were included. A number of studies were found and selected by screening their abstracts and then their full texts. Sequential steps in systematic studies selection is described through developing the PRISMA diagram (Figure 1). From the collected articles, preliminary title and abstract screening would exclude both the unrelated discussion toward concerns of this review and unfound specific keywords. After assessing 13 full-text articles for eligibility, authors decided to include three articles in the final analysis.
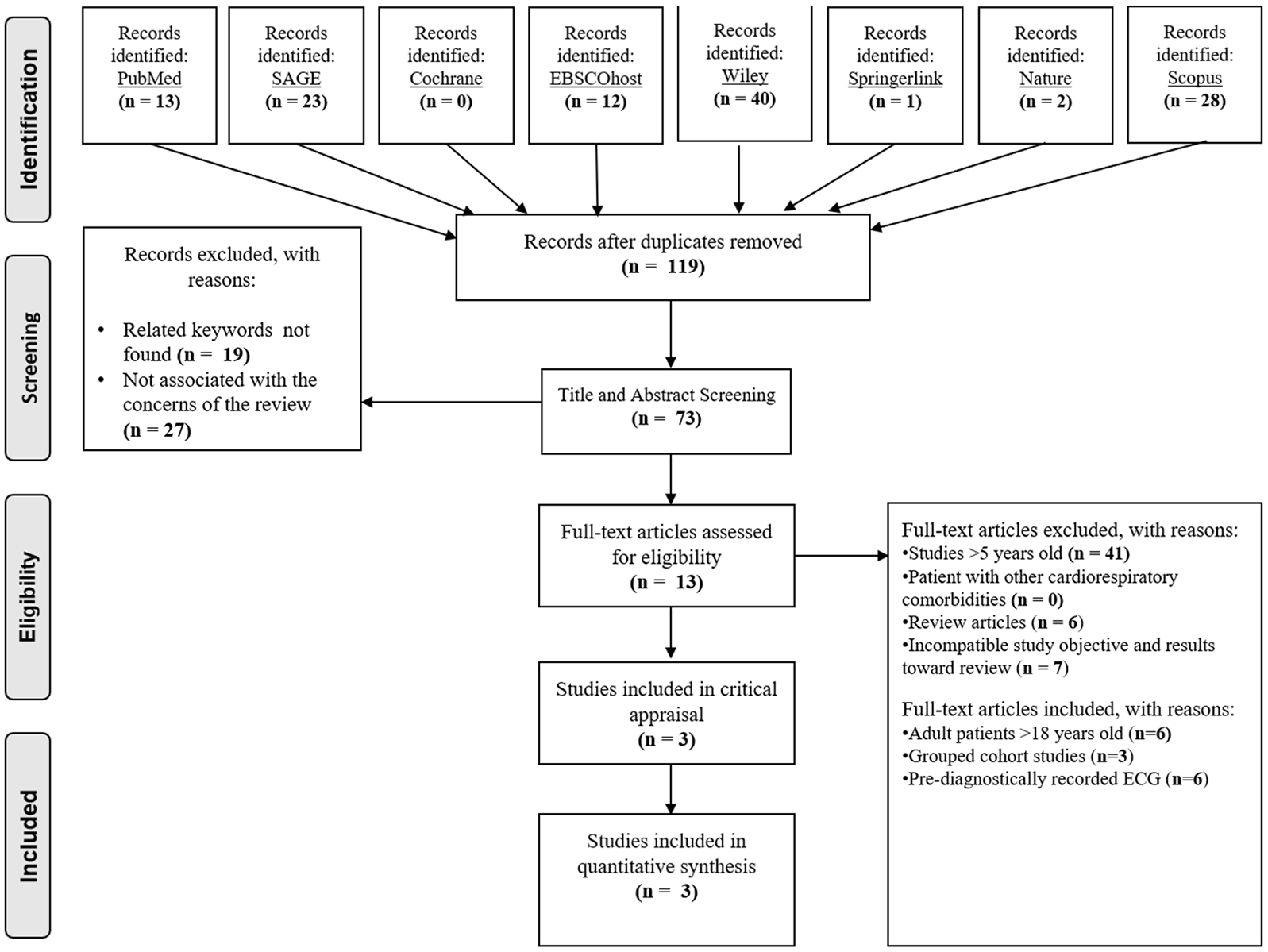
Search strategy using PRISMA flowchart.
Critical appraisal
Critical appraisal was extensively conducted on three observational studies via diagnostic study appraisal tools from Oxford Center of Evidence-Based Medicine. The results are included in Table 2.
Critical appraisal results of the selected observational studies.
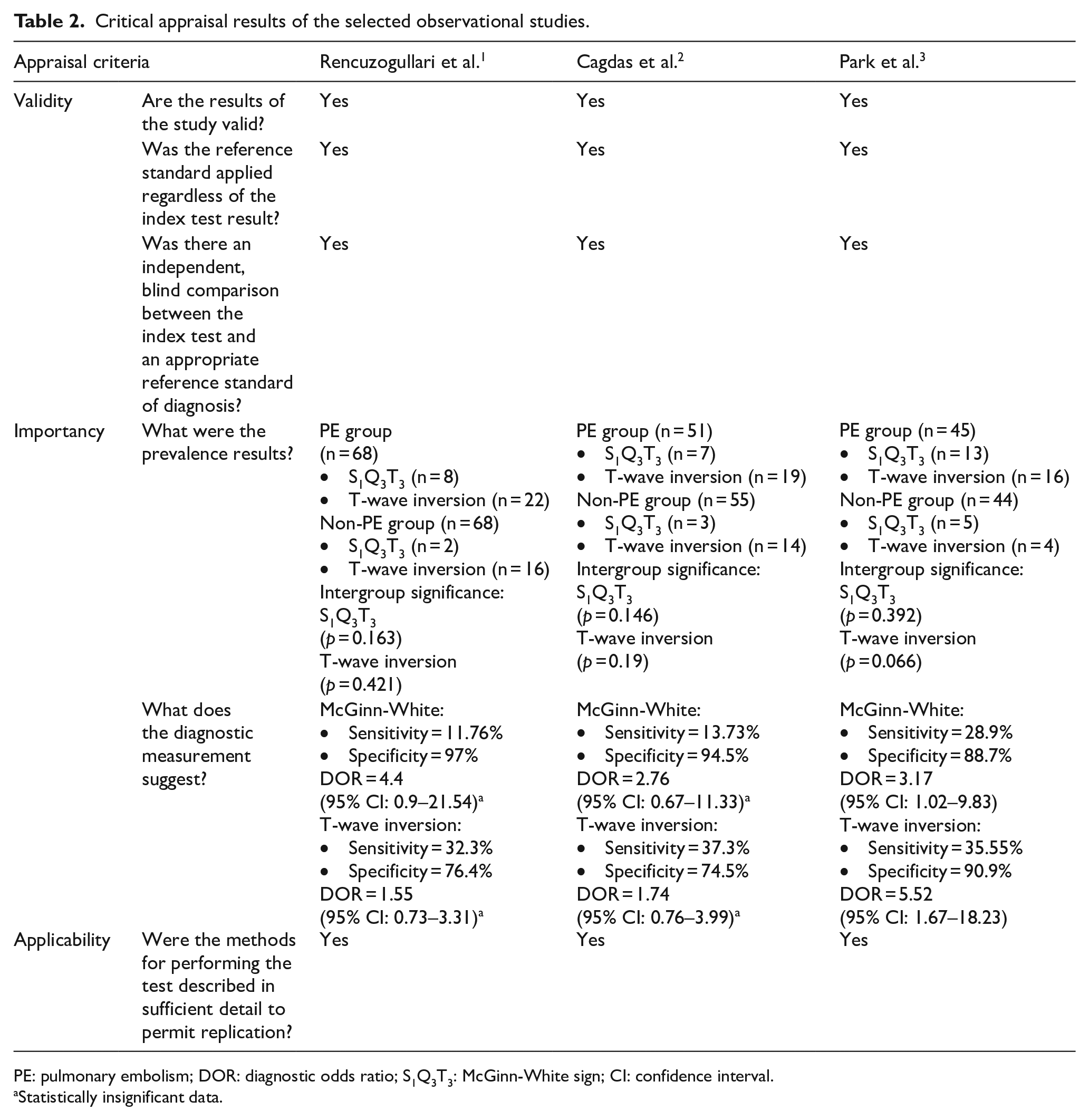
PE: pulmonary embolism; DOR: diagnostic odds ratio; S1Q3T3: McGinn-White sign; CI: confidence interval.
Statistically insignificant data.
Study results
Based on all three observational studies, a study population with suspected symptoms of PE, such as atypical chest pain, blood oxygen desaturation, and increased effort of breathing, underwent CTPA test for further confirmatory diagnosis. A number of the tested populations were finally diagnosed with acute PE with no statistically significant difference in terms of Wells Score between groups of PE and non-PE. Examination of initial 12-lead ECG parameters was done in both groups prior to CTPA testing. The summarized study characteristics comprising population characteristics and sample size is shown in Table 3.
Summarized study characteristics.
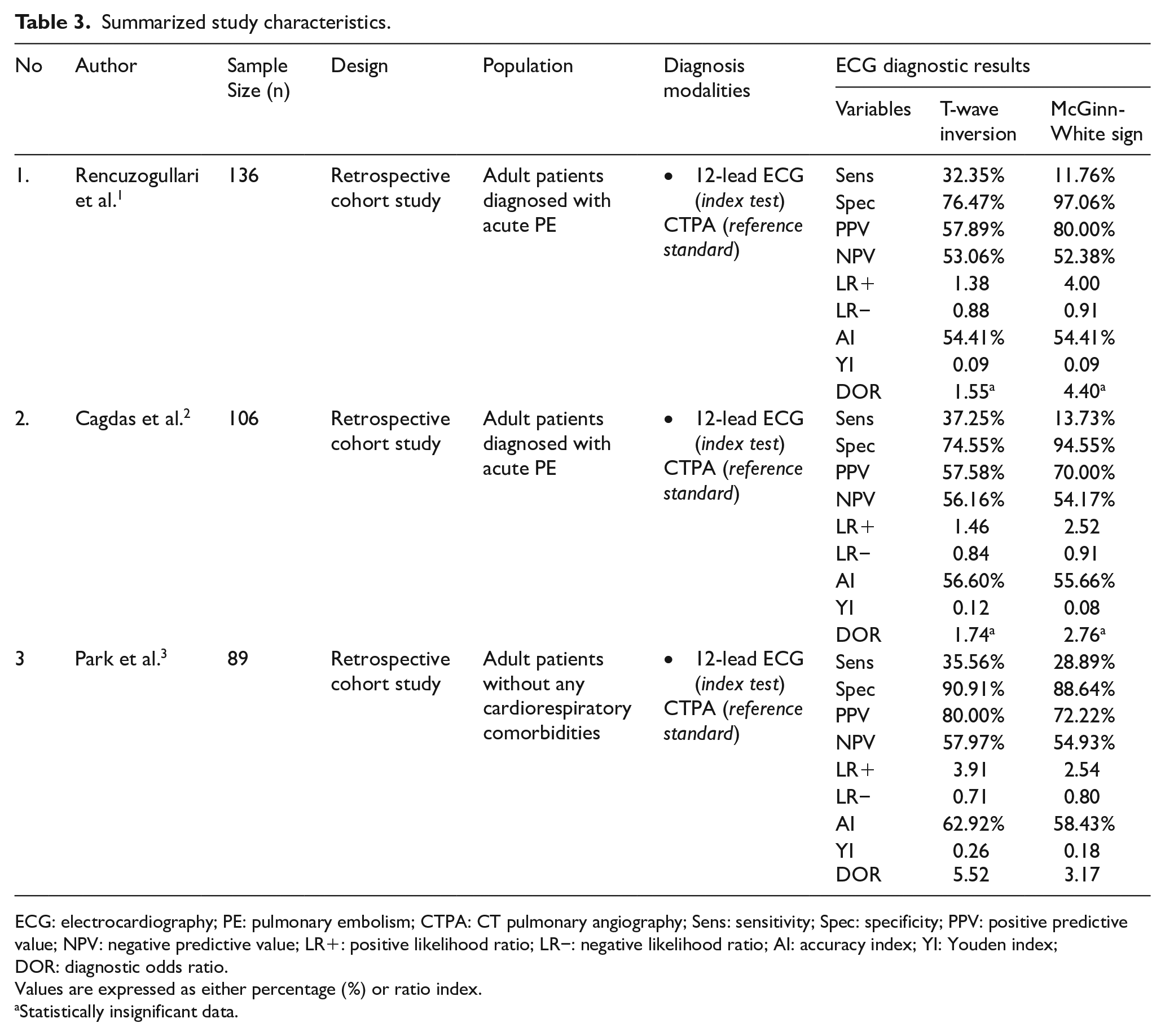
ECG: electrocardiography; PE: pulmonary embolism; CTPA: CT pulmonary angiography; Sens: sensitivity; Spec: specificity; PPV: positive predictive value; NPV: negative predictive value; LR+: positive likelihood ratio; LR−: negative likelihood ratio; AI: accuracy index; YI: Youden index; DOR: diagnostic odds ratio.
Values are expressed as either percentage (%) or ratio index.
Statistically insignificant data.
Following diagnostic calculation on both McGinn-White sign and T-wave inversion on anterior precordial leads, each study provides different acquired values based on prevalence of the aforementioned ECG signs in suspected PE patients. According to Rencuzogullari et al., 1 McGinn-White sign exhibits higher specificity value than that of T-wave inversion (97.06% vs 76.47%). The same concluding diagnostic results could also be found in Cagdas et al. 2 showing higher specificity value of McGinn-White sign. Nevertheless, the most sensitive marker for acute PE could be found in all observational study with less specific discovery of McGinn-White sign, except in Park et al. 3 study. Therefore, plotting of the diagnostic results in diagram would provide wider point of views in analyzing their vast patterns, which is shown in Figure 2.
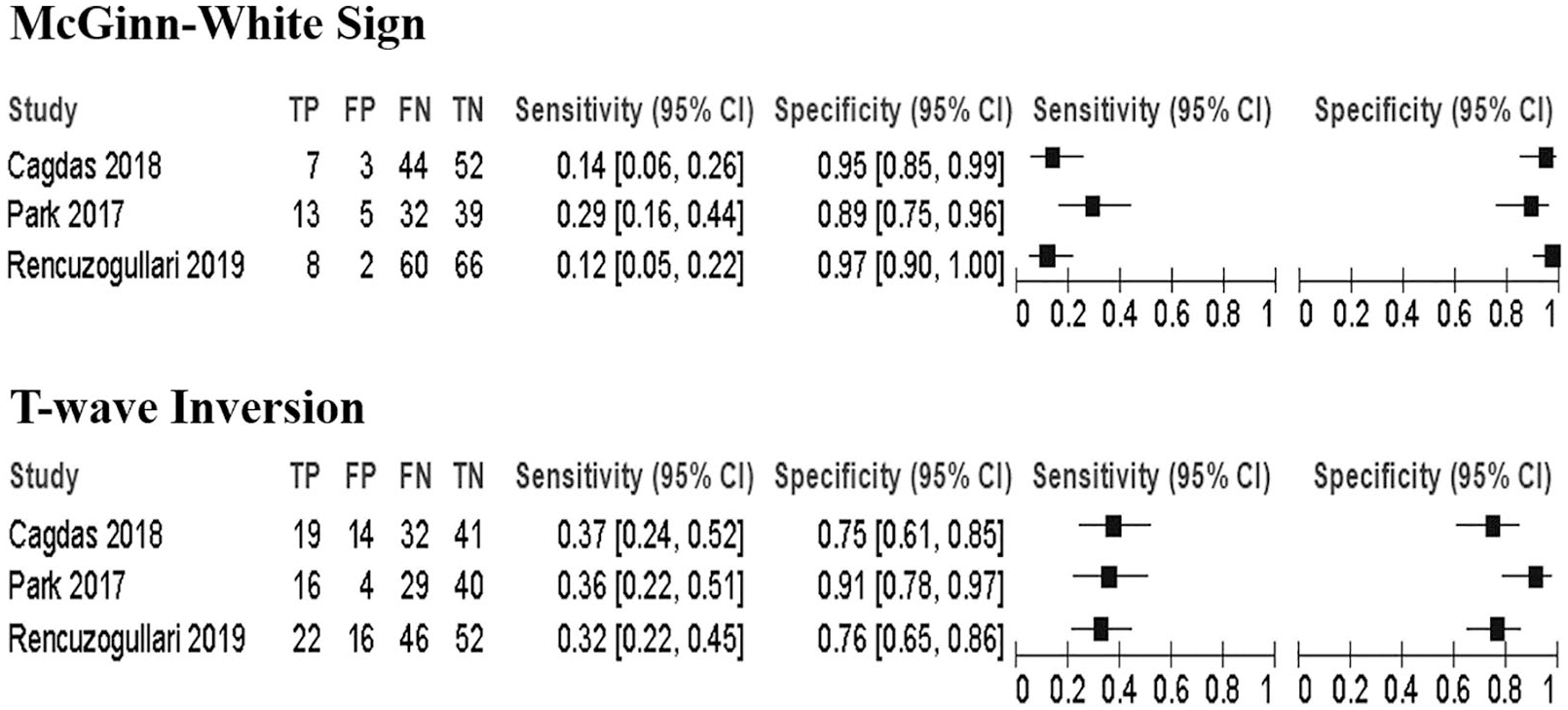
Plotted sensitivity and specificity values of McGinn-White sign and T-wave inversion in all summarized studies.
T-wave inversion has higher average of sensitivity in diagnosing ECG abnormalities, but not pathognomonic to acute PE; on the contrary, McGinn-White sign was more specific to acute cardiovascular disease involving RV dysfunction due to pulmonary embolus. Both signs actually exhibit minor impact in terms of sensitivity index. However, further diagnostic analyses of both signs suggest higher averaged accuracy and Youden index (YI) found in T-wave inversion in anterior leads than that of McGinn-White sign (accuracy index (AI): 57.97% vs 56.16%; YI: 0.16 vs 0.12), suggesting more meaningful diagnostic value. To execute clear overall calculation, diagnostic odds ratio (DOR) values were performed based on ratio of sensitivity/specificity of both signs in every study. Studies conducted by Rencuzogullari et al. 1 and Cagdas et al. 2 show insignificant DOR results due to its zero-value inclusion in their 95% confidence interval (Figure 3). Thus, both studies exhibit less important effect toward the conclusion of the diagnostic result.
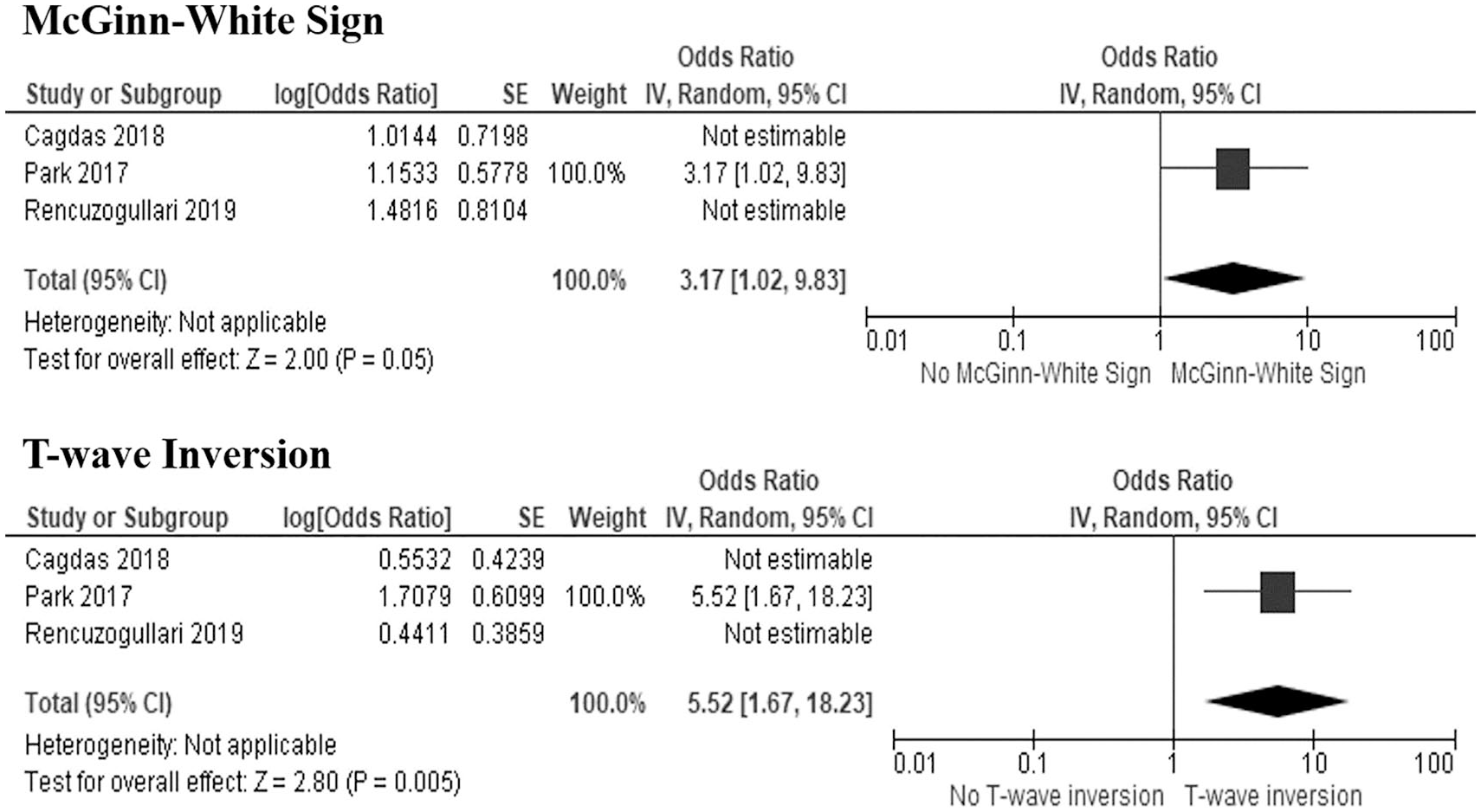
Plotted diagnostic odds ratio of McGinn-White sign and T-wave inversion in the included non-insignificant studies.
Discussion
This systematic review and meta-analysis demonstrates that T-wave inversion was associated with better diagnostic value than McGinn-White sign in diagnosing patients with suspected acute PE. Furthermore, this review encourages general physicians, as well as fellow internists and cardiologists, to propose prompt diagnosis of pulmonary embolus for early treatment of emergency cardiovascular events. PE is a challenging diagnosis for its various unspecific clinical presentations. Suspected patients are ought to be evaluated based on detailed history taking, systematic physical examination, and specific laboratory findings in addition with validation risk scoring system based on Wells or modified Geneva score.5,6 Usage of high-quality multi-sliced imaging of computed tomography (CT) scan has become gold standard in diagnosing any anatomical defects in terms of pulmonary vascular obstructive disease. Injection of blood-soluble iodine contrast into main pulmonary artery branch could aid findings of obstructed pulmonary blood flow via chest CT scan. European Society of Cardiology has proposed guidelines regarding recommendation on grading clinical risk of patients with positive D-dimer test based on scoring system prior to CTPA testing. 5 In addition, RV dysfunction or strain with increased systolic pulmonary artery pressure were found to be closely related to acute PE with previous studies. 7 ECG finding of McGinn-White sign has become well-known pathognomonic sign for acute PE based on its pathophysiology in generating RV strain due to pressure overload. Acute pressure overload affects right-sided dominance of cardiac conduction and repolarization than does chronically elevated RV pressure.8,9 In the past studies, the McGinn-White sign did not have any confirmed diagnostic value for acute PE regardless of its pathophysiological reasoning. Inconsistent previous studies have brought this sign to controversial debate. Therefore, searching of other specific signs in ECG could help in diagnosing acute PE. Another underlying mechanism associated with PE-related ECG changes involves right coronary arteries compression due to increased intraventricular cavity pressure, further disrupting subendocardial perfusion and exacerbating catecholamine-mediated myocardial ischemia. 10 This is when anterior leads T-wave inversion could appear in the most beginning event of acute PE. This review presents the factual data that anterior leads T-wave inversion possesses better DOR than that of McGinn-White sign (DOR = 5.52 vs 3.17). Considering the compared importance of selected studies, T-wave inversion shows better sensitivity and specificity than that of McGinn-White sign along with higher 4.5% AI.
All studies present similar limitations which include retrospective-based medical record analysis as this condition does not fully represent with real-life acute events. Inadequate sample size is the main problem found within these three studies, for data significance is extremely important to deliver prompt results into conclusion. Insignificant prevalence of both ECG signs in PE and non-PE groups are mainly due to unfiltered patients with past cardiorespiratory diseases history in the groups; therefore, they account for the possible heterogeneity of ECG evidences in both groups.1–3
To conclude, present systematic review and meta-analysis demonstrate that anterior lead T-wave inversions present better diagnostic value than that of classic pattern of McGinn-White sign in ECG presentation of patients with suspected acute PE. Non-invasive and fast initial diagnostic tool would be one of the main reasons that ECG is employed in the emergency settings. Regarding the elaborated findings of ECG signs in diagnosing acute PE, anterior leads T-wave inversion suggests higher sensitivity and specificity percentage than that of McGinn-White sign. Hence, future recommendation involving larger studies on both signs is important to represent the overall diagnostic values toward patients with suspected PE.
Footnotes
Acknowledgements
Authors are grateful to have had excellent work during this and other related project. The authors would especially like to thank chief of Division of Non-Invasive Diagnostic Cardiovascular Imaging in National Cardiovascular Center Harapan Kita, who has provided extensive personal and professional guidance and taught the author a great deal about scientific research in cardiovascular medicine.
Author contributions
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated equally in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, revision, or final approval of the manuscript. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All data generated or analyzed during this study are included in this published article (and its supplementary information files).
Ethical approval
No ethical approval will be needed because data from previous published studies in which informed consent was obtained by primary investigators will be retrieved and analyzed.
Human rights
This article does not contain any studies with human subjects performed by the any of the authors.
Informed consent
Written informed consent will not be needed as consent had been obtained from previous published studies by primary investigators.