
Abstract
Background:
Point-of-care tools are invaluable in the emergency department. Arterial lactate has been used for prognostication in subsets of population in the emergency department but not often for a heterogeneous population.
Objectives:
We aimed to study the use of arterial lactate as a prognostication and disposition tool in an undifferentiated population presenting to the emergency department.
Methods:
We conducted a prospective study among all consenting emergency department patients with age >18 years, who had an arterial blood gas performed as a part of routine care and had a lactate value ⩾2 mmol/L. We collected data on demographics, comorbidities and patient disposition from the emergency department and 28-day mortality as a follow-up telephonically.
Results:
We included 469 patients with a median age of 37 years. Sixteen provisional diagnoses were made in the emergency department, and pneumonia/lower respiratory tract infection was relatively higher (13.6%). The median lactate was 4.6 (interquartile range = 3.2–7) with 155 patients (33%) being transferred to intensive care unit and 62 deaths (13.2%) recorded at 28 days. Furthermore, we observed optimum values for lactates at 5 mmol/L predicted intensive care unit admissions and 6 mmol/L predicted mortality. A unit increase in arterial lactate in the emergency department significantly increased mortality by 66% (95% confidence interval = 1.45–1.88; p < 0.001) and had a 2.15 times (95% confidence interval = 1.63–2.83; p < 0.001) significantly higher chance of being transferred to the intensive care unit.
Conclusion:
Arterial lactate can be used as a prognostication tool for a heterogeneous population presenting to the emergency department.
Clinical significance:
Point-of-care investigations such as arterial lactate can help the emergency physician make quick decisions on the floor and guide prognostication and disposition.
Introduction
Emergency physicians (EPs) often have the unenviable task of working up a case with an unreliable history for life-threatening presentations. In such time-constricted settings, point-of-care investigations help make quick decisions and expedite better patient care.
One of the important biomarkers and point-of-care test is lactate. Lactate is just not an end product of anaerobic metabolism but also a marker of critical illness. 1 There is a direct relationship between increased lactate and mortality and morbidity.2–6 Also, increased lactate may be a silent marker of hypoperfusion such as hypotension.7,8
Knowing its ability to detect patients with hypoxia and increased metabolic stress, we hypothesised the use of arterial lactate as a tool to identify patients with increased mortality risk.
Accordingly, the objective of this study is to determine the use of arterial lactate as a prognostic marker for survival among patients (requiring an arterial blood gas (ABG) analysis) presenting to the adult emergency department (ED) of a tertiary care hospital. Acknowledging the bed crunch situation in most hospitals, we also sought to ascertain whether arterial lactate can be used as a disposition tool (i.e. discharge/ward/high dependency unit (HDU)/intensive care unit (ICU) admissions).
Materials & methods
We conducted a prospective observational study in an ED with 50,000 annual visits that serves an urban academic teaching hospital with 1500 beds. The study was approved by the Institutional Ethics Committee of St. John’s Medical College. We collected data from patients presenting to the ED between January and June 2016, after assessing for eligibility and obtaining written informed consent. We reported all the sections based on TRIPOD checklist. 9 We consecutively included all patients with age >18 years, who had an ABG performed as part of routine care and had a lactate value ⩾2 mmol/L within 1 h of arrival to the ED. There was no preset cut-off value to determine hyperlactemia; however, we chose a value of ⩾2 mmol/L based on evidence from previous studies. 2 A probable diagnosis was made in the ED based on standardised definitions (Supplemental Table 7), and we collected data on demographics, comorbidities, and patient disposition from the ED and 28-day mortality. The patients were followed up telephonically and the data were captured on structured case record forms. As we aimed to obtain data about a heterogeneous population, our only exclusion criterion was non-consenting patients.
For testing arterial lactate, we collected 5 mL of heparinized arterial blood without stasis in vacuum containers and analysed using a standardised ABG machine (ABL800 FLEX analyzer RADIOMETER (India)) in the ED.
The overall mortality among patients presenting to the ED with any lactate value ranged between 8% and 16%.6,7,10,11 We estimated a 13% mortality at 28 days among patients presenting to the ED with an arterial lactate ⩾2 mmol/L. To detect an odds of 1.52,12 of initial lactate ⩾2 mmol/L in the ED predicting mortality, with 80% power and a one-sided alpha of 5%, we needed 469 patients.
We entered data on Epi Info 7 and performed statistical analysis using SPSS ver 16.0 (SPSS Inc., Chicago, IL, USA). We presented continuous data as mean (SD) or median (interquartile range (IQR)) depending on the sample distributions and categorical variables as frequency (percentage). We considered pairwise deletions for missing data. We performed univariate binary logistic regression analysis for mortality with age, sex, arterial lactate, comorbidities and smoking. All the variables were considered for the multivariate logistic regression model. We then constructed a receptor operating characteristics (ROC) curve to discriminate whether the multivariate mortality model was good enough to discriminate between the two categories of outcome (dead/ alive). We also performed a multinomial logistic regression analysis for patient disposition and included age, sex and serum lactate as variables. We also constructed ROC curves for lactate and mortality and ICU disposition and calculated Youden’s index to determine the optimum lactate cut-off values for both. All the tests were interpreted at a significance level (p ⩽ 0.05).
Results
Patient characteristics
We recruited 469 patients with a median age of 37 (IQR = 28–51) years and a higher proportion of males (55.2%). We categorised our patients to 16 different diagnoses in the ED, of which lower respiratory tract infection (LRTI)/pneumonia (13.6%) and polytrauma (12.6%) were the majority. Diabetes mellitus (DM) (39.4%) and hypertension (31.6%) were the most common comorbidities seen in our patient group. In our sample, we noted that 17.9% were active smokers and 13% consumed alcohol. We also explored the use of concomitant medications that could influence arterial lactate and found 24.8% of our population were on metformin and 61% among the patients who died were on this medication. The median lactate in our study was 4.6 (IQR = 3.2–7). We recorded 62 deaths (13.2%) at 28 days and a higher proportion of patients were transferred to HDU (39.7%) and ICU (33%) after an ED admission. Patients with polytrauma and pulmonary oedema were significantly higher among the non-survivors and influenza-like illness and LRTI/pneumonia were higher in the survivor group (Table 1).
Overall characteristics of patients.
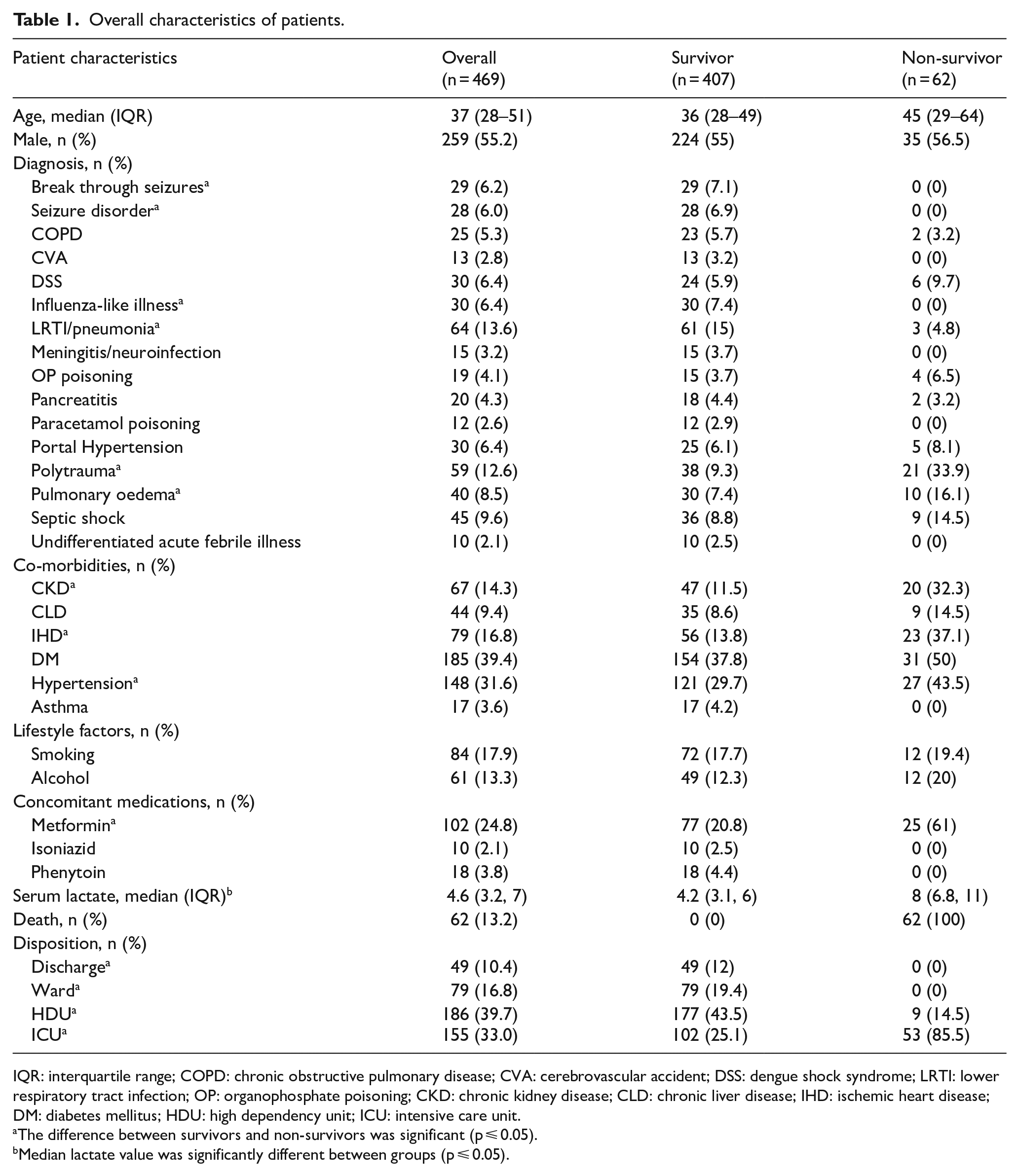
IQR: interquartile range; COPD: chronic obstructive pulmonary disease; CVA: cerebrovascular accident; DSS: dengue shock syndrome; LRTI: lower respiratory tract infection; OP: organophosphate poisoning; CKD: chronic kidney disease; CLD: chronic liver disease; IHD: ischemic heart disease; DM: diabetes mellitus; HDU: high dependency unit; ICU: intensive care unit.
The difference between survivors and non-survivors was significant (p ⩽ 0.05).
Median lactate value was significantly different between groups (p ⩽ 0.05).
On further exploring the patient subgroups, the median age groups were different for different diagnoses, with higher age groups presenting with pancreatitis, portal hypertension, pulmonary oedema and septic shock. We noted that more patients who presented with meningitis (53.3%), organophosphate poisoning (OP) (52.6%), pulmonary oedema (57.5%) and septic shock (66.7%) required an ICU disposition after admission. Higher mortality rates than the overall mortality were observed in patients with DSS (20%), OP poisoning (21.1%), polytrauma (35.6%), pulmonary oedema (25%) and septic shock (20%) (Supplemental Table 5).
Serum lactate and patient mortality & disposition:
We categorised serum lactates into subgroups (Table 2), based on its median values obtained from patient disposition subgroups. We observed a median increase in age and arterial lactate levels on patient disposition, with the highest levels observed in ICU cases (Supplemental Table 6). We saw an increase in mortality, the HDU and ICU admissions, with an increase in lactate groups. We observed a higher proportion of ward admission in lactate subgroup >6.5 mmol/L due to seizures and this probably would have diluted the ICU admission and mortality proportions. We also observed that 20% of the hyperlactatemia patients with values between 2 and 4.2 mmol/L are likely to be discharged from the ED (Table 2). A cut-off lactate value of 5 mmol/L was better in predicting ICU admissions (Figure 1) and an optimum value of 6 mmol/L had a higher sensitivity, specificity and better negative predictive value for mortality (Figure 2).
Patient disposition, mortality and risk stratification according to hyperlactatemia subgroups.
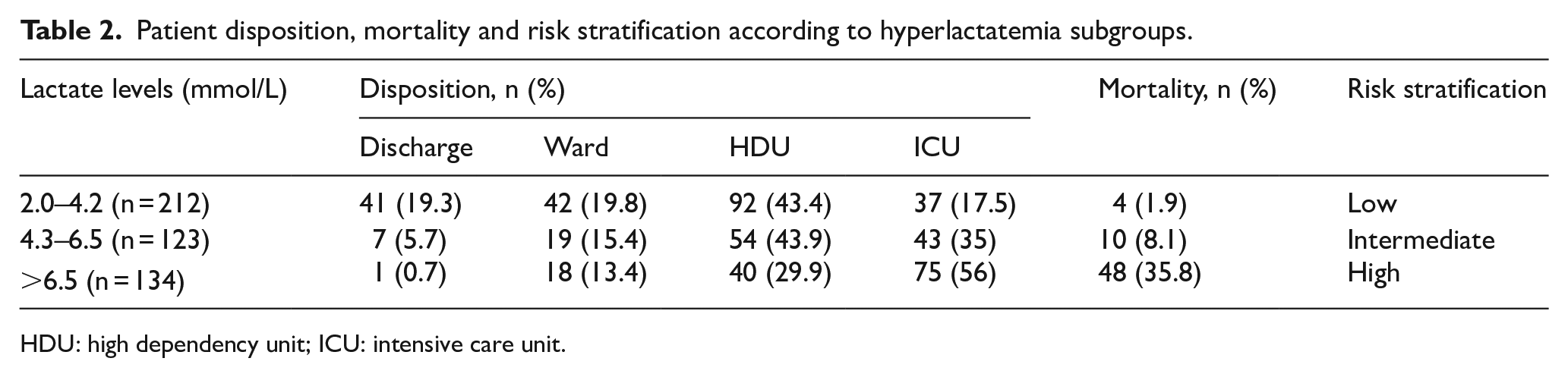
HDU: high dependency unit; ICU: intensive care unit.
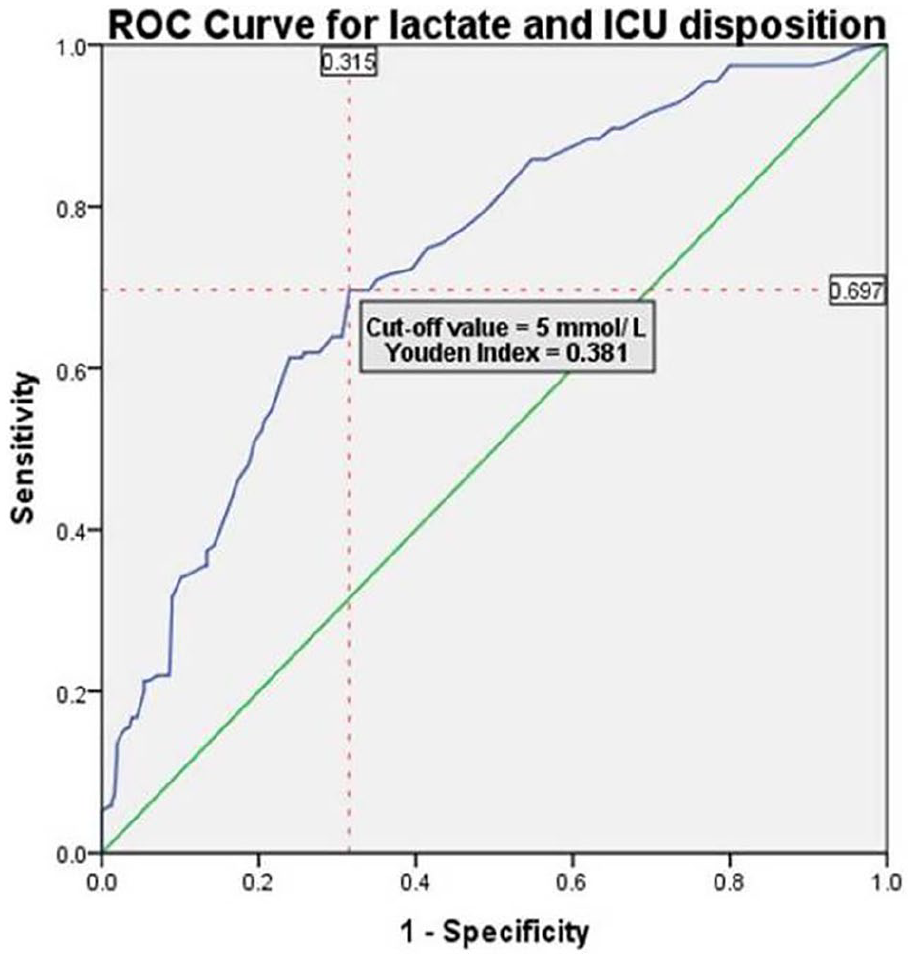
ROC curve for lactate and ICU disposition.
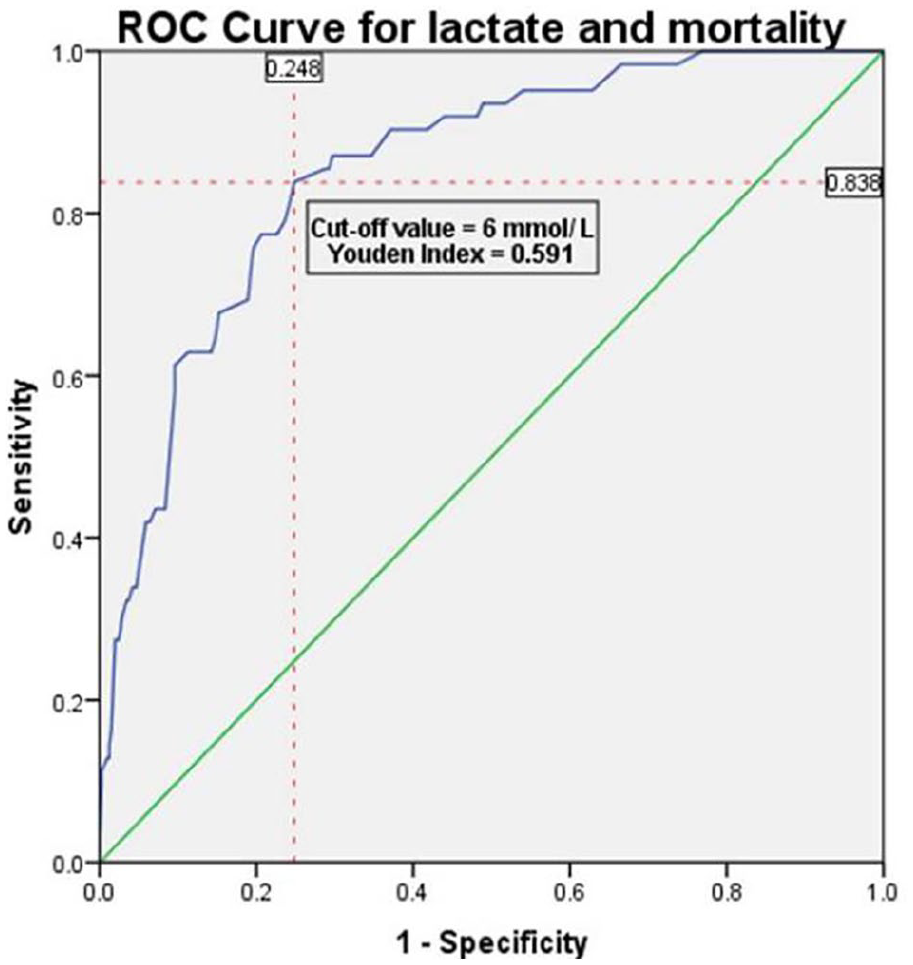
ROC curve for lactate and mortality.
Table 3 shows the univariate and multivariate logistic regression to determine whether arterial lactate was a predictor of mortality at 28 days. A unit increase in arterial lactate levels beyond 2 mmol/L significantly increased mortality by 66% (95% confidence interval (CI) = 1.45–1.88; p < 0.001). A patient with a past history of ischemic heart disease had 6.17 times (95% CI = 2.02–18.85; p = 0.001) higher risk of mortality. Although age, chronic kidney disease (CKD), and hypertension were independent predictors of mortality, it was not significant in our multivariate model. Our multivariate logistic regression model classified mortality significantly better than by chance. The ROC area under the curve was 0.867 (95% CI = 0.817–0.918), p < 0.001 (Supplemental Figure 1).
Serum lactate as a predictor of mortality (Nagelkerke R2 44.6%).
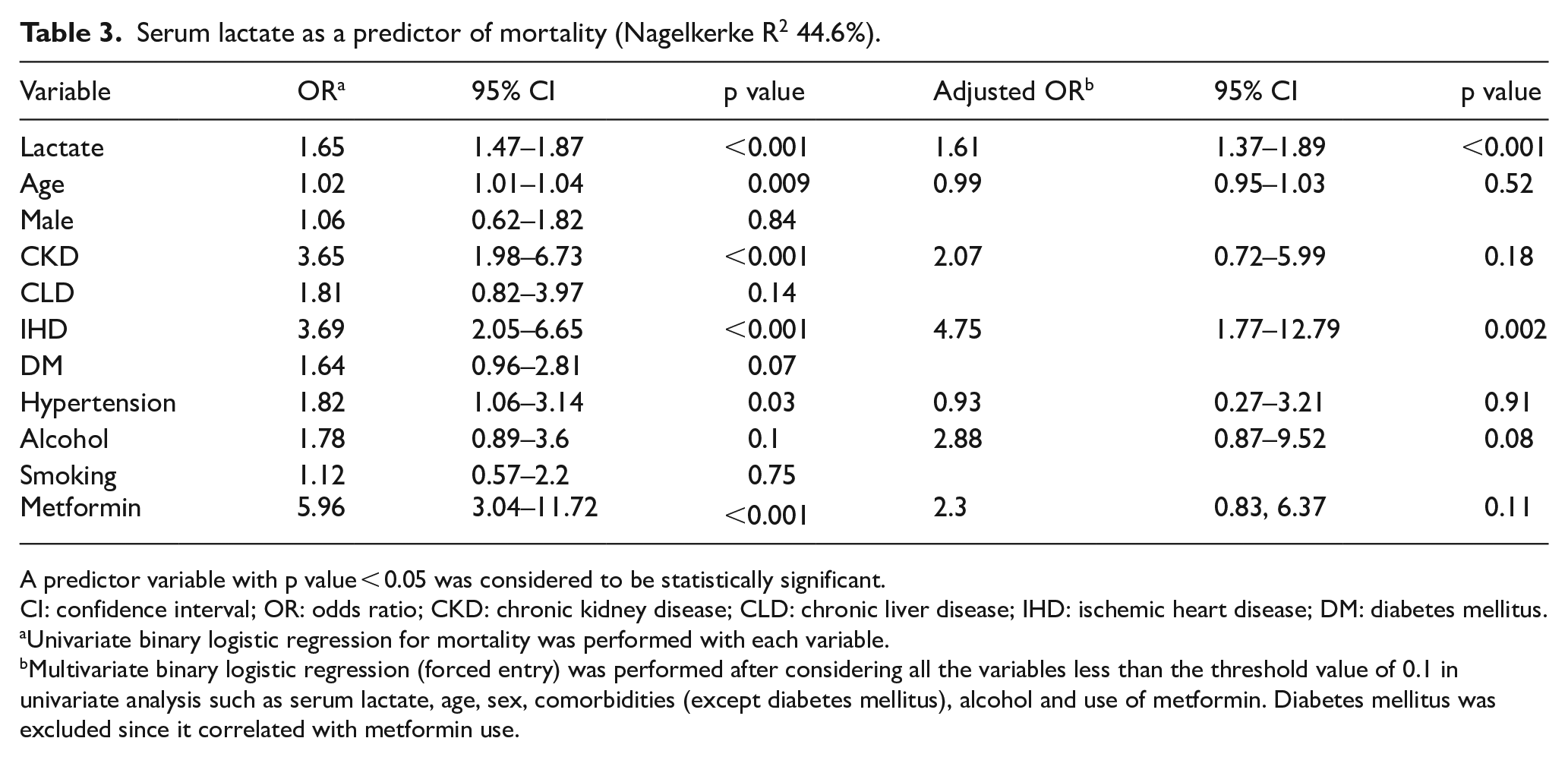
A predictor variable with p value < 0.05 was considered to be statistically significant.
CI: confidence interval; OR: odds ratio; CKD: chronic kidney disease; CLD: chronic liver disease; IHD: ischemic heart disease; DM: diabetes mellitus.
Univariate binary logistic regression for mortality was performed with each variable.
Multivariate binary logistic regression (forced entry) was performed after considering all the variables less than the threshold value of 0.1 in univariate analysis such as serum lactate, age, sex, comorbidities (except diabetes mellitus), alcohol and use of metformin. Diabetes mellitus was excluded since it correlated with metformin use.
We also performed a multivariate multinomial logistic regression to determine the use of arterial lactate as a disposition tool. A unit increase in arterial lactate measured on admission to the ED had a 2.15 times (95% CI = 1.63–2.83; p < 0.001) significantly higher chance of being transferred to the ICU or a 62% significantly higher chance of being admitted to either the ward (95% CI = 1.23–2.13; p = 0.001) or HDU (95% CI = 1.23–2.1; p < 0.001). Similarly, as age increased the chance of being admitted to the ward, HDU and ICU significantly increased in this order (Table 4).
Serum lactate as a predictor of patient disposition.
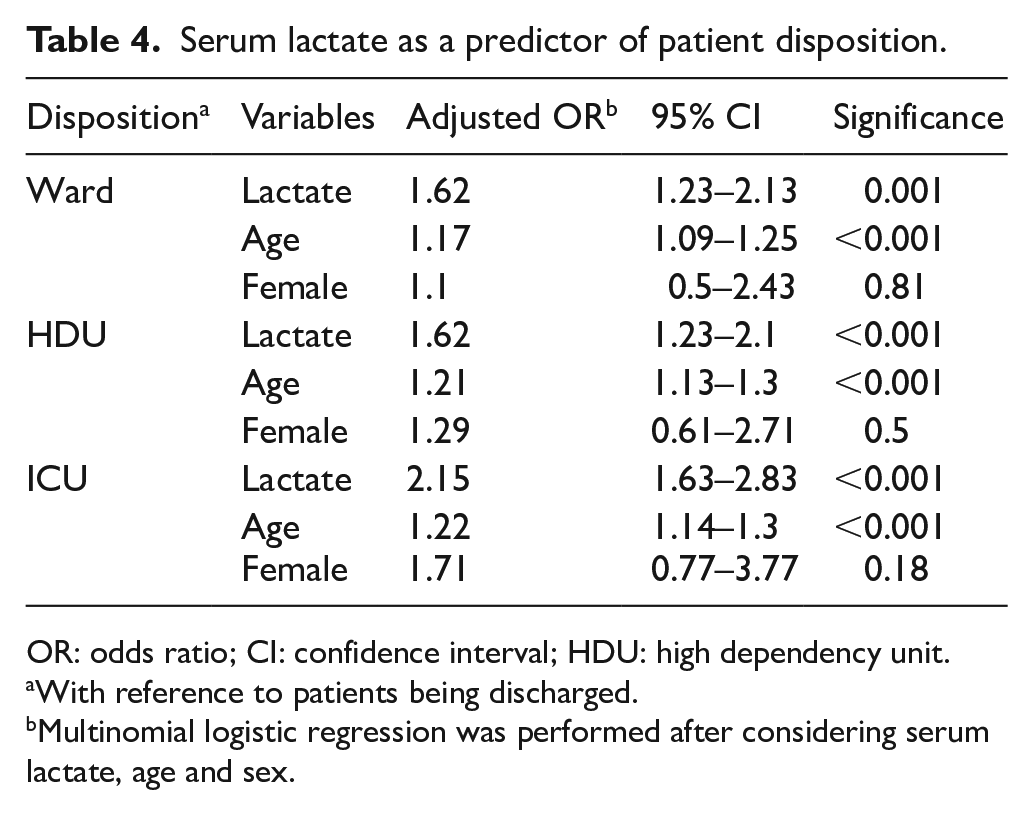
OR: odds ratio; CI: confidence interval; HDU: high dependency unit.
With reference to patients being discharged.
Multinomial logistic regression was performed after considering serum lactate, age and sex.
Discussion
Many biological parameters have been evaluated as prognostic tools in different settings. However, lactate over the last decade has proved to be a useful biomarker to predict mortality among patients presenting to the ED.2,3,6 Although its utility had been proven, Contenti et al., 5 in their retrospective study, demonstrated that lactate measurements were not based on any specific protocol, but were at the discretion of the treating physician. An arterial blood sampling was associated with a 2.77 times higher risk of a composite of death, ICU admission or emergency surgery. 5 Our study evaluated the prognostic utility of an initial admission arterial lactate among an unselected ED population, as a predictor of 28-day mortality and also as a disposition tool. Our patient population was of a lower age when compared with other studies where the range was between 54 and 73.4,11,13–15
Prognostic utility of arterial lactate has been evaluated in disease-specific population in different settings. Bou Chebl et al., 16 in their retrospective study which had 80% of the population with infection, predicted a higher odds of mortality with lactate values >4 mmol/L. In pneumonia/LRTI, the use of lactate as an independent prognostication tool is still under question; however, when combined with recognised scoring systems such as qSOFA (quick sequential organ failure assessment) and CURB-65 (confusion, urea, respiratory rate, blood pressure, and 65 years of age or older), it predicted outcomes better.13,17 Among patients presenting with trauma, serum lactate correlated well with 24-h mortality. 18 A value >4 mmol/L had a very high sensitivity and specificity in predicting mortality and ICU admissions. 18 Baxter et al., 3 in their systematic review, found that initial lactate and lactate clearance were associated with mortality, need for massive blood transfusion and need for emergency operations among trauma patients. But lactate was inconsistent as a predictor of ICU admissions. An obvious confounder to the premise of high lactates equates to increased morbidity or mortality is patients presenting with seizures. Patients with seizures are known to have high lactate values due to local muscle tissue hypoxia, and also have a higher rate of lactate clearance that does not correlate with mortality or ICU admissions. 5 In OBSERVE-LACTATE study, mortality was very low in people with seizures and toxic exposures and overdose. 15
Mortality from recent studies in an unselected ED population11,12 ranged between 16% and 18.4%, while that for pneumonia patients13,17 was 21% and 33% and for trauma was around 18%, 16 which are much higher compared with our study in an undifferentiated population. Elevated lactate and low mean arterial pressure/shock significantly predicted mortality in different population, and the odds ratio was similar to our study. 11–13 A lactate value >8 mmol/L caused mortality in more than 45% of the patients presenting to the ED.12,15 Our study showed similar results, but on excluding patients presenting with seizures, the mortality in the lactate subgroup >6.5 mmol/L was more than 55%. Type A hyperlactemia which occurs due to poor tissue perfusion or oxygenation had significantly higher mortality when compared with type B hyperlactemia, further classified as B1 type–related failure of clearance such as hepatic insufficiency; B2 related to drugs or toxins (e.g. metformin); B3 related to inborn errors of metabolism. 19 However, it is important to note that the median lactate values in both the groups were not significantly different; hence, there is a possibility of under-estimating the mortality rate in our study due to concomitant use of metformin. Our proposed cut-off value for mortality was 6 mmol/L which had a higher prognostic value, while in a study by Edward et al., 14 3.8 mmol/L predicted 24-h mortality better and Freund et al. 20 determined 2 mmol/L to be highly predictive of a severe outcome.
The hyperlactemia subgroups in our study were categorised to risk stratify and aid patient disposition. Lactate values predicted similar odds for ward or HDU admission but the chances were significantly higher for ICU admissions, similar to the study by Chen et al. 13 After dichotomising data for ICU admissions and mortality, we estimated an optimum lactate cut-off value of 5 and 6 mmol/L respectively. However, our proposed hyperlactemia subgroups are inclusive of the cut-off values and could be further explored for its clinical utility in different populations. Among patients with pneumonia, a lactate value ⩾4 mmol/L had a higher specificity for mortality and a value ⩾6 mmol/L had a high sensitivity, specificity and positive predictive value for ICU admissions. 13 Lactate could be used as vital biomarker in routine patient care who show signs of deterioration and it would be prudent to shift the patient to the ICU with a lactate value of >5 mmol/L. 21 Puskarich et al., 6 in their systematic review, identified intermediate lactate values between 2 and 4 mmol/L to be associated with a significant risk of mortality irrespective of blood pressure status, among patients presenting with early sepsis. Several studies established that lactate cut-off value between 4 and 4.25 mmol/L had a significantly higher prognostic value in predicting mortality/deterioration/complications than a value <4 mmol/L, which is lower than the optimal cut-off values in our study.5,8,15,19,22,23
Limitations and strengths
Our study had a few limitations. We did not screen all the patients in our ED and there is a possibility of selection bias for select disease conditions. The cut-off parameters for mortality and ICU predictions could be overestimated as we have not included patients with serum lactates <2 mmol/L. We did not include diagnoses based on type A or B hyperlactemia and did not take initial vitals into consideration, which are well known to influence lactate. However, from an extensive literature search in various databases, our study is one among a few evaluating the utility of serum lactate among a variety of presentations in a tertiary hospital ED in India. We also characterised the patient disposition in a heterogeneous population.
Conclusion
In conclusion, we proved that admission arterial lactate values can be used as a prognostication tool in the ED in all patients except those presenting with seizures or influenza-like illness. Coupled with disease-specific prognostic scores, arterial lactates could be used as a vital biomarker to predict mortality and aid patient disposition. However, the potential of risk stratification for patient disposition and mortality based on lactate values could be explored in further multicentric studies.
Supplemental Material
Supplementary_material – Supplemental material for Arterial lactate as a prognostic tool to predict mortality and disposition in the emergency department: A prospective observational single-centre study
Supplemental material, Supplementary_material for Arterial lactate as a prognostic tool to predict mortality and disposition in the emergency department: A prospective observational single-centre study by William Wilson, Dhiraj Ravindran Selvaraj, MV Ramya Kumar, Vinayak Jain, Simran Umra and Shakuntala Murty in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
We acknowledge the support of the hospital technical and non-technical staff for the study.
Author contributions
W.W. and D.R.S. researched literature, conceived the study and wrote the first draft. S.M. was involved in protocol development, gaining ethical approval. V.J., S.U. and M.V.R. were involved in data acquisition and data analysis. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Availability of data and materials
Data will be made available on request to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The St. John’s Medical College Institutional Ethics Committee consent was taken (Ref. 157/2015).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Human rights
All study participants were provided with the Participant Information sheet and due consent was taken as per the Institution Ethics Committee requirements.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article. All data were kept confidential and were coded.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.