
Abstract
Introduction:
Coronavirus disease 2019 (COVID-19) has become a pandemic with millions of contagions all over the world. However, as of June 2020, relatively few indigenous cases have been identified in Taiwan.
Case Presentation:
A 34-year-old man presented to our emergency department with progressive rhinorrhoea, a sore throat, and recent travel to the United States (Texas) and Mexico. He was diagnosed with COVID-19 after a positive throat swab test. Even though he was not initially isolated, there was no cluster of infection identified after epidemiological investigation.
Discussion:
This case demonstrates Taiwan’s unique epidemic prevention strategy, including the utilization of face masks, compact screening indications, quarantine arrangements, and the effective disposition of confirmed cases.
Conclusion:
In addition to managing various emergent conditions, emergency physicians should prepare epidemic prevention strategies as soon as possible and provide frontline suggestions.
Introduction
The World Health Organization (WHO) declared a global emergency on 11 March 2020 because the coronavirus disease 2019 (COVID-19) outbreak had quickly spread across the entire world. 1 Taiwan, with 23 million people, is an island with frequent commercial trade and international exchange with the rest of the world. In the early days of the epidemic, Taiwan was considered one of the regions with the highest risk of being impacted by COVID-19.2,3 However, no large-scale community outbreak has occurred in Taiwan. 4 As of 31 May 2020, the latest epidemiological data of COVID-19 in Taiwan revealed a total of 443 confirmed cases, 352 (79.5%, 352/443) of which were imported cases, 55 (12.4%, 55/443) were local cases, and 36 (8.1%, 36/443) were cases in the Navy’s Dunmu Fleet; and the mortality rate was 1.58% (7/443). 5 We aim to share the epidemic prevention strategy implemented in Taiwan through a confirmed case in an emergency department (ED) in order to provide a reference for emergency physicians (EPs) elsewhere.
Case description
A 34-year-old man visited the ED of our community hospital with approximately 20,000 annual visiting patients and 250 hospital beds on 17 March 2020 with chief complaints of a sore throat and rhinorrhoea. The patient had no prior medical history; however, he had travelled from Taiwan to Texas, the United States and Mexico from 23 February to 6 March 2020. Upon his return to Taiwan, the patient received a self-health management notice at the airport due to negative upper respiratory symptoms. He returned to work as usual but wore a surgical mask throughout the day and rode a private motorcycle to the office rather than using public transportation.
At our ED, his national health insurance card was scanned at triage, and our hospital information system (HIS) was alerted of his travel history. His vital signs were as follows: a body temperature of 36.0℃, pulse rate of 76 beats/min, respiration rate of 18 breaths/min, and blood pressure of 128/77 mmHg. His physical examination revealed clear bilateral breath sounds. Neither his laboratory results nor his chest X-ray indicated any obvious abnormal finding. Due to his travel history and positive upper respiratory symptoms, the patient received a SARS-CoV-2 throat swab reverse transcription polymerase chain reaction (RT-PCR) test according to the COVID-19 guidelines established by the Taiwan Central Epidemic Command Centre (CECC). The patient was then discharged and told to self-quarantine at home until the test result came back.
The result was positive on 19 March 2020, and admission was arranged for the patient. The patient was admitted to a negative-pressure isolation room, and supportive treatment was given. The patient’s symptoms and signs improved gradually, and he was discharged after a smooth clinical course and 3 negative SARS-CoV-2 swab tests 10 days later. Ten individuals he had personal contact with after his return to Taiwan also received SARS-CoV-2 swab tests and these test results were all negative.
Discussion
In countries with insufficient resources to perform SARS-CoV-2 throat swab tests, it is reasonable to use travel history as an indication for screening if no community infection outbreak has occurred. However, since patients may not honestly report their travel history, the Taiwan government opted to maintain strict border control measurements at the airports and seaports and enable the HIS to inform triage nurses and EPs about patients’ travel history when their national health insurance cards were scanned through the use of big data analytics which integrated national health insurance and customs databases. 5 Furthermore, in most parts of Taiwan, visitors were asked to present their national health insurance card before entering hospitals in order to prevent in-hospital infections.
The case patient had been in contact with several people, including family members and office colleagues before his COVID-19 diagnosis. The patient and his contacts wore face masks throughout the day, and no cluster of infection was identified in the epidemiologic survey. Most East Asians encountered severe acute respiratory syndrome (SARS) 17 years ago, and people in Taiwan remember the suffering it caused. Therefore, many Taiwanese believe that wearing face masks in public places could have prevented droplet infections at the beginning of the COVID-19 outbreak in China in January 2020. Conversely, the WHO at the time suggested that people should not wear face masks unless they were sick or needed to care for someone who was sick.6,7 With the increasing demand for face masks, the Taiwanese government initially prohibited the export of face masks and declared the rationing of face masks on 6 February. Since then, people were permitted to buy 9 masks every 14 days with their national health insurance card at contracted pharmacies. Workers who were unable to buy face masks from pharmacies during business hours could alternatively access a centralized online system to order face masks. These measurements ensured that every Taiwanese person had the opportunity to wear a face mask while using public transportation, visiting crowded places, and when a respiratory infection was suspected. 4
The present case returned from Texas, United States, on 6 March 2020, when the confirmed COVID-19 cases in the United States were still mainly sporadic and imported. The patient therefore only received the self-health management suggestions of avoiding public transportation and maintaining social distance. The policy was humane and allowed for the patient to continue to go to work under adequate self-protection measurements. According to the risk of contagion, the CECC established three categories of management of suspected cases: home isolation, home quarantine, and self-health management. Details regarding these categories are demonstrated in Table 1.5,8 This management strategy may be adjusted according to changes in the global epidemic. At present, any citizen can call the hotline 1922 or access telemedicine from their homes to report suspicious symptoms or seek related advice. Once a COVID-19 diagnosis is confirmed, arrangements are made to admit the patient to a negative pressure isolation room in a hospital. Patients are admitted to hospitals according to the severity of their illness: the medical centres are responsible for treating severe confirmed cases, while the regional and community hospitals treat mild confirmed cases and are tasked with setting up community screening stations.
Comparison between home isolation, home quarantine, and self-health management in Taiwan.
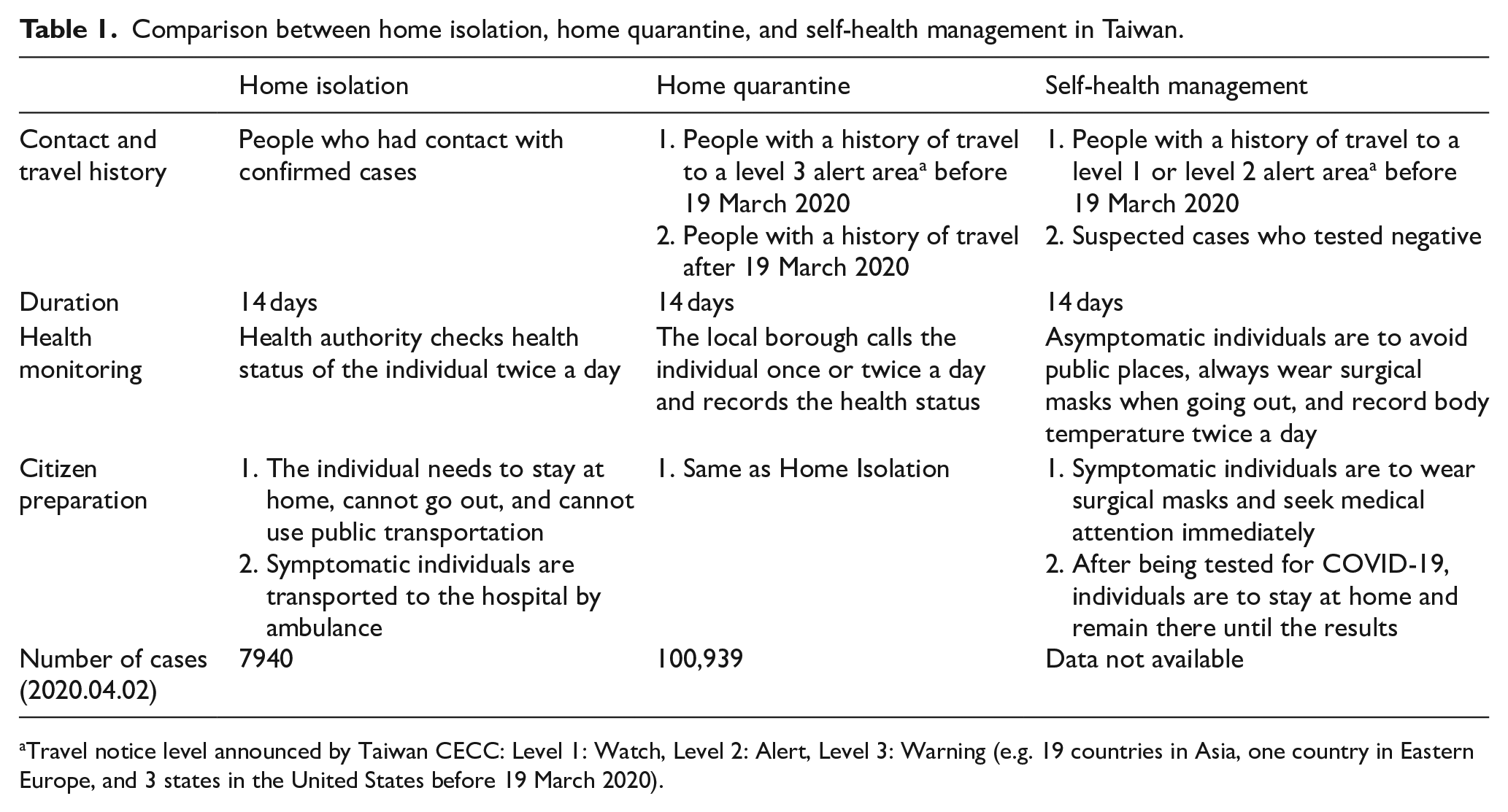
Travel notice level announced by Taiwan CECC: Level 1: Watch, Level 2: Alert, Level 3: Warning (e.g. 19 countries in Asia, one country in Eastern Europe, and 3 states in the United States before 19 March 2020).
Taiwan, Korea, Hong Kong, and Singapore were all considered exemplary models of preventing COVID-19 outbreaks during the first 3 months of the epidemic.9–12 In our case report, we described key measurements including indications for the SARS-CoV-2 throat swab test, supply patterns for face masks, quarantine arrangements, and the disposition of confirmed cases. In order to understand different approaches that have been used to decrease the spread of this pandemic, we compared the measurements taken by these four countries in Table 2.5,9–12 However, future research needs to be undertaken to prove the efficacy of these preventive measurements, as the COVID-19 pandemic continues to strain health systems worldwide.
Comparison of epidemic prevention strategies in Taiwan, Korea, Hong Kong, and Singapore.
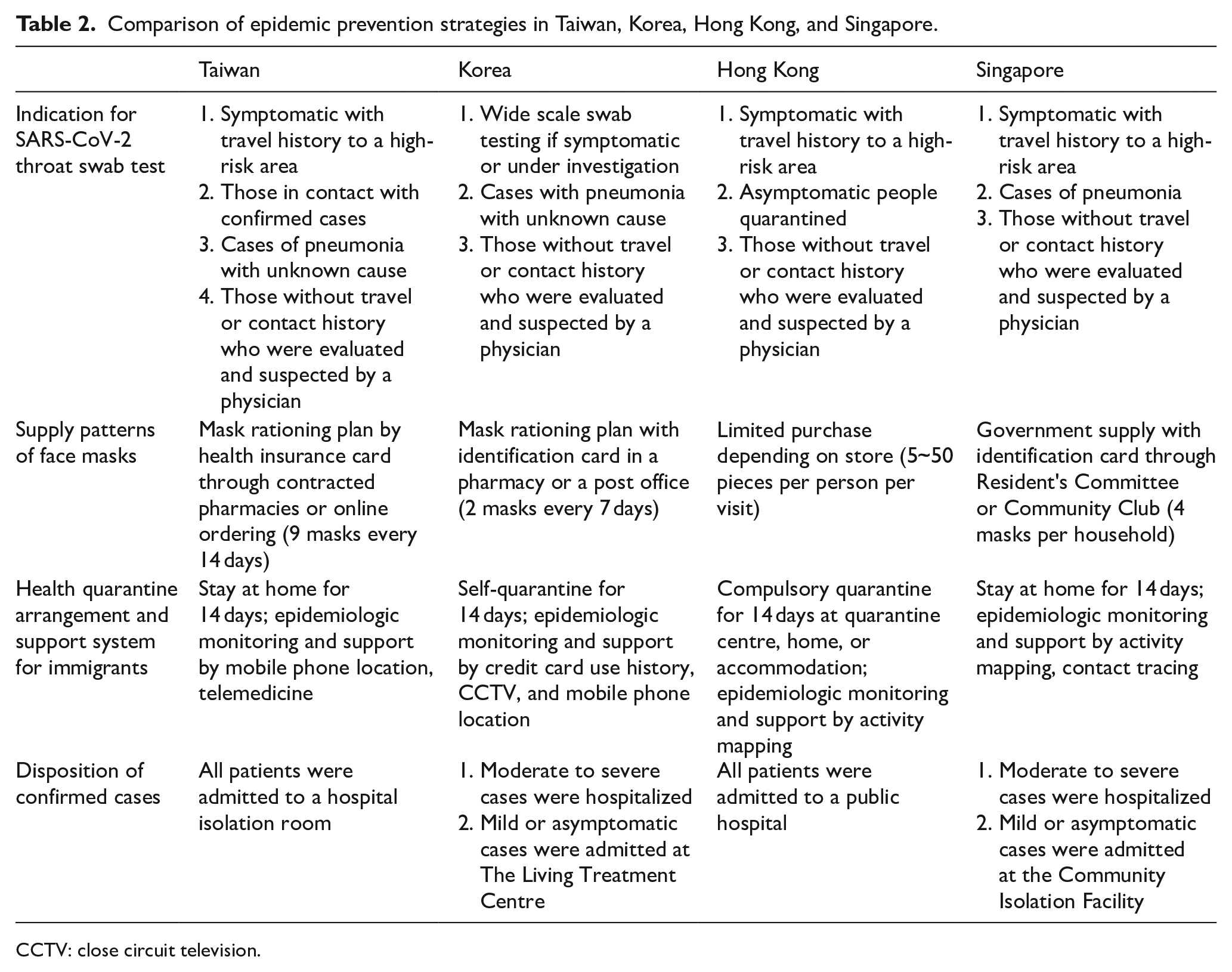
CCTV: close circuit television.
Footnotes
Acknowledgements
We thank Dr. Jui-Yuan, Chung for typesetting and expert recommendations.
Authorship
C.P. Hsu and Y.T. Lin conceived of the presented idea and drafted the manuscript. W.L. Cheng and C.S. Lin encouraged C.P. Hsu and Y.T. Lin to investigate epidemic prevention in infection of COVID-19 and supervised the findings of this work. All authors discussed the results and contributed to the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Medical records.
Ethical approval
This study was approved by the institutional Review Board in the Cathay General Hospital.
Human rights
Subjects’ participation in this research is entirely voluntary. It is their choice whether to participate or not. Whether they choose to participate or not, all the services they receive at this clinic will continue and nothing will change. If they choose not to participate in this research project, we will still offer the treatment that is routinely offered in this hospital for disease, and they can choose to withdraw from the study at any time.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.