
Abstract
X-ray interpretation is a fundamental skill in emergency practice. Post-operative eyes with implants may sometimes pose clinical challenges on post-traumatic event diagnosis and differentiation from organ wasting. Recommended by authorities and guidelines, computed tomography is indicated for evaluation of head injury cases, yet incidental abnormal findings such as radiopacity in the eyeball might create dilemma to diagnosis. History taking and clinical examinations are essential for the interpretation of the radiopacity in orbital imaging. Subtle and uncommon radiological findings of the eye will be discussed.
Keywords
Clinical picture
A 67-year-old lady suffered from a facial injury after a fall. She had facial abrasions and epistaxis that stopped spontaneously. Palpation over frontal sinuses, orbital rims, maxillary sinuses and mandible were non-tender without any discontinuity. Denture was present, and chewing was normal. Her eyes appeared normal on slit-lamp examination, with preserved red reflex. Direct fundoscopy could clearly identify the optic disc, macula and normal viewable retina. Point-of-care ultrasound (POCUS) of the right eye revealed poor B-scan images; eyeball configuration was unclear despite adjustment of different parameters. Systemic examinations did not reveal any focal neurological signs. X-rays were ordered for local hospital’s triage purpose.
Questions
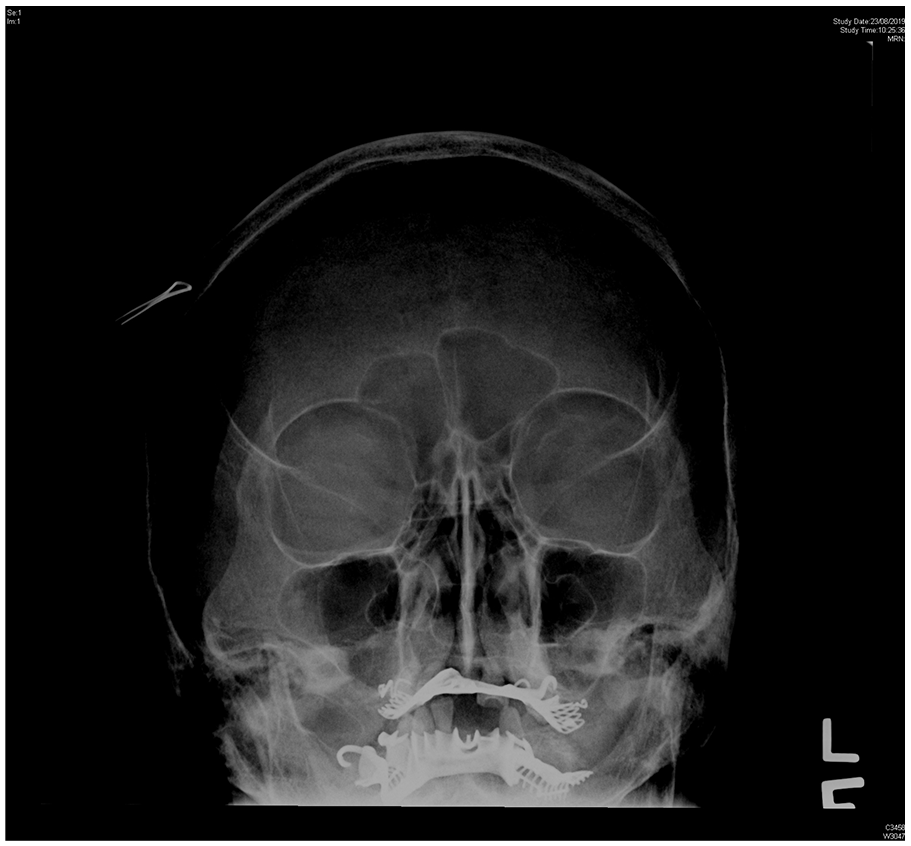
What was the subtle abnormality over the orbital X-ray (Figure 1)? (Contrast adjusted film (Figure 2) is attached.)
What are the possible causes of poor visualization of the posterior chamber in ocular ultrasound?
An orbital computed tomography was done in view of the finding in question 1 (Figure 3), what are the possible differential diagnoses?

Orbital X-ray (anteroposterior view).
Contrast adjusted film for the same orbital X-ray in Figure 1.
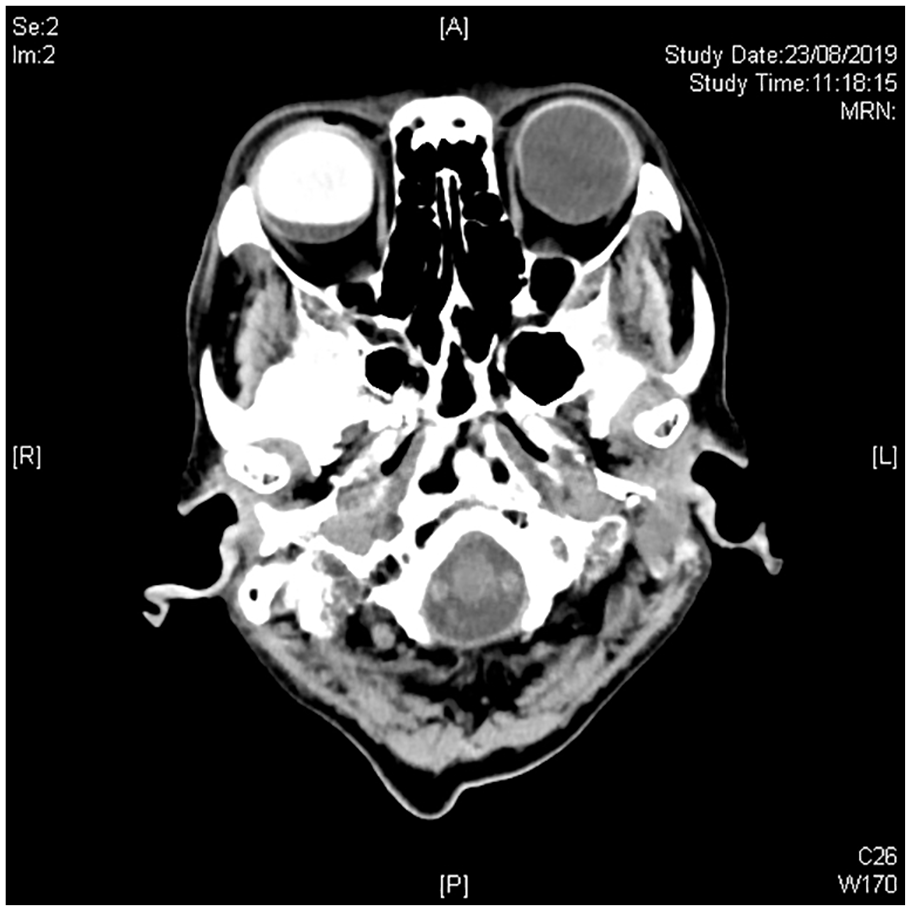
Follow-up computed tomography scan of the orbit with transverse cut over the eyes.
Answers
Subtle circular homogeneous radiopacity over the central right orbit was evidenced. The edge was indistinct, with no attachment over the orbital rim.
Causes can be divided into operator and diseased eye factors. Operator factors include insufficient coupling gel between the eye and the probe, or air bubble trapped within the coupling gel, which causes reverberation artefacts. Besides, poorly orientated probe can cause angle of incidence artefact. These causes are adjustable with operator manoeuvres. Diseased eye factors include gas or silicone oil (SO) filled cavities within the eye, no matter over the anterior chamber or the vitreous cavity. The difference in acoustic impedances (density X velocity of sound in medium) across the two different substances (biological tissues vs. iatrogenic implanted substitutes) causes change in reflection of the ultrasound beam and generation of artefacts.
Radiopacity over the right eyeball was evidenced. Calcium, blood, silicone and some types of resin for prosthesis are radiopaque on computed tomography (CT). The differential diagnoses are SO-filled eye, dense vitreous haemorrhage (VH), calcification in eyes with phthisis bulbi and artificial eye orbital implant following enucleation or evisceration surgery. The configuration of the eyeball, intensity of radiopacity and orbital content are all essential for establishing the diagnosis, with correlation to clinical examination findings.
Discussion
Supported by the normal clinical findings, this patient had no orbital or ocular injury. She had right eye retinal detachment (RD) surgery years ago. There was no orbital fracture on X-ray, and the radiopacity over the right eyeball was contributed by the injection of SO into vitreous cavity for RD repair. This also explained the failure on eyeball visualization on POCUS (Supplementary Figure 4), as the acoustic impedances across the interface between the aqueous humour/intraocular lens complex and the SO globule were huge, thus generated artefact and appeared as non-penetrable. 1
Sitting could displace the intravitreal SO to anti-gravity dependent position (specific gravity lighter than water of 0.97 g/cm3), 2 and in underfilled SO eyes may allow some visualization of the posterior chamber. 1 Most ultrasound machines in Emergency Rooms are not equipped with SO mode, and ultrasound imaging of the SO-filled eyeball appears elongated on display by a factor of ~1.5, 3 given the fact that ultrasound travels were slower (~2/3 of normal) in SO (980 m/s (Supplementary Figure 4) compared to 1532 m/s (Supplementary Figure 5) through normal vitreous). Other than the intrinsic eye pathologies causing poor visualization of its content on ocular ultrasound, operators’ skills are also potential pitfalls for generating artefacts. These operator-dependent adjustable factors include insufficient coupling gel between the eye and the probe, or air bubble trapped within the coupling gel, which causes reverberation artefacts. Besides, poorly orientated probe can cause angle of incidence artefact.
SO is a longer lasting (compared to different medical gases such as C3F8 and SF6) 4 and optically transparent vitreous substitute widely used in RD surgery. Its non-expansile property is superior to gases to facilitate patient’s air or underwater travel shortly after RD operation, because variable pressurized cabin would not change its intraocular volume. With a specific gravity lighter than water of 0.97 g/cm3, 2 SO floats on top of water. 5 Containing the metalloid element of silicon, SO’s atomic number offset its physical density, 6 giving a significant X-ray attenuation and a higher Hounsfield unit (HU) than water, thus appearing radiopaque on CT. This was confirmed objectively by the HU measurement on CT (Supplementary Figure 6), which showed that the right SO-filled eye had multiple times higher HU than the contralateral unoperated left eye with natural vitreous. Reported HU for SO in the literature ranges from 50 to 130; 7 which in our case, it had a mean value of 118 ± 7.94 HU (Supplementary Figure 6), ranged from 80 to 140 HU by manual measurement over different points of the SO-filled eye (Supplementary Figure 7).
With SO placed inside the confined vitreous cavity intra-operatively, patients are instructed to practice prone posturing as much as possible post-operatively to allow the SO globule floats up, and presses on the detached retina, thus promoting retinal adhesion. This helps to achieve surgical success while waiting for the retinal barrier lasers to secure in a few weeks’ time. However, with prolonged placement over a few months, SO (especially lower centistoke ones) may emulsify to form small droplets, which could migrate to anterior chamber through the lens zonules, causing rise in intraocular pressure and the clinical sign of ‘inverted hypopyon’. Other clinical signs of long-standing SO in eye are band keratopathy, decompensated bullous keratopathy, subconjunctival SO slippage, secondary glaucoma and electoretinogram changes.
The key on differentiating causes of vitreous radiopacity lies on clinical history and examination findings, eyeball configuration and associated orbital radiological findings (Supplementary Figure 8). Artificial eye or eyeball prosthesis would be revealed from history taking, and obviously detected by the lack of natural eye movement with visual acuity of no light perception. CT would demonstrate homogeneous opacity, without the natural eyeball tissue. Optic nerve would be attached to the scleral shell containing the prosthesis in evisceration cases, but not in enucleation cases. In contrast, extraocular muscles are present in both post-evisceration and post-enucleation cases, attaching to the orbital implant.
Phthisis bulbi is calcification and shrinkage of the globe caused by persistent lowish intraocular pressure. Phthisical eye in early stage appears shrinking, with haze and blur cornea and poor anterior chamber view. Visual acuity is usually down to around light perception only. With progressive shrinkage to end stage, phthisical eyeball is difficult to be recognized with just remnant calcification. Radiological images would show enophthalmos resulting from loss in globe volume, with irregular radiopacity inside caused by the calcification.
Normal looking eyes with symmetrical red reflexes are suggestive of post-operative SO-filled eye as in this case, which fundus and optic disc could be seen through the optically clear SO as normal. Upon CT scanning in supine position, SO in vitreous cavity would float upwards. A small crescent posterior to the SO globule within the intact eyeball (scleral shell) could be seen. 5
VH gives no or very blur view of the retina on fundoscopy with a loss of red reflex from the concerned eye. Unless very dense haemorrhage caused by significant trauma, VH is usually not detected on CT, not to say X-ray. There is no role of radiological imaging with X-ray unless suspect orbital fracture or globe rupture associated with the trauma. Instead, dilated fundus examinations for aetiology and POCUS for retina status are essential for establishing the diagnosis.
In conclusion, SO in eye may sometimes pose clinical challenge on diagnosis. However, thorough history taking and clinical examinations are significant for the interpretation of the opacity in orbital X-ray.
Supplemental Material
Supplementary_material – Supplemental material for Opacity in orbital X-ray
Supplemental material, Supplementary_material for Opacity in orbital X-ray by Sunny Chi Lik Au and Simon Tak Chuen Ko in Hong Kong Journal of Emergency Medicine
Footnotes
Author contributions
S.C.L.A. researched the literature, conceived the study, patient recruitment, data extraction, clinical photos retrieval and wrote the manuscript. S.T.C.K. revised the manuscript critically for intellectual content. S.C.L.A. contributed for the concept and design of study, acquisition of image and drafting the article. S.T.C.K. contributed for revising article critically for important intellectual content, final approval of version to be published.
Availability of data and materials
Data sharing is not applicable to this article as no data sets were generated or analysed during this study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: The authors declare that there is no conflict of interest. Dr. S.C.L.A. and Dr. S.T.C.K. are employee of Hospital Authority, under Hong Kong East Cluster Ophthalmic Service.
Ethical approval
Hospital Authority does not require ethical approval for reporting individual cases because patients were consented upon receiving treatment from Hospital Authority.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for the anonymized information to be published in this article.
Trial registration
It is not applicable because only one case is reported in this work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.