
Abstract
Background:
Patients who have successful return of spontaneous circulation after cardiac arrest may experience post-cardiac arrest syndrome. Procalcitonin can be used to assess the severity of post-cardiac arrest syndrome. The association between procalcitonin and outcomes in Asian patients with post-cardiac arrest syndrome has not been extensively studied.
Objective:
This study aimed to investigate the predictive value of serum procalcitonin level in the prognosis of patients hospitalized after out-of-hospital cardiac arrest.
Methods:
A retrospective observational study using the multicenter Korean Cardiac Arrest Research Consortium registry between October 2015 and June 2018 was performed. Serum procalcitonin level at the early phase of hospital presentation was obtained from the patients hospitalized after out-of-hospital cardiac arrest. In-hospital mortality and neurologic outcomes at hospital discharge were estimated. The relationship between serum procalcitonin level and in-hospital mortality and neurologic outcomes of patients was analyzed.
Results:
A total of 254 patients hospitalized after out-of-hospital cardiac arrest were included. Serum procalcitonin level was significantly elevated in non-survivors compared to survivors (0.17 (0.05–0.18) ng/dL vs. 0.10 (0.05–0.39) ng/dL, p = 0.017, respectively). In addition, serum procalcitonin level was significantly elevated in patients with unfavorable outcomes at hospital discharge compared to those with favorable outcomes (0.16 (0.06–1.10) ng/dL vs. 0.07 (0.04–0.22) ng/dL, p < 0.001, respectively). However, serum procalcitonin level had a weak predictive value for in-hospital mortality (area under the receiver operating characteristic curve: 0.587, 95% confidence interval: 0.517–0.657, p = 0.017, cut-off = 0.12 ng/dL, specificity = 57.4%) and unfavorable outcomes (area under the receiver operating characteristic curve: 0.646, 95% confidence interval: 0.571–0.721, p < 0.001, cut-off = 0.11 ng/dL, specificity = 62.3%).
Conclusion:
Elevated serum procalcitonin level in patients hospitalized after out-of-hospital cardiac arrest at the early phase of hospital presentation is associated with poor outcomes. However, serum procalcitonin level had weak diagnostic accuracy for predicting in-hospital mortality and unfavorable outcomes.
Introduction
Patients who have successful return of spontaneous circulation (ROSC) after cardiac arrest may experience multiple organ failure owing to complex pathophysiological changes caused by systemic ischemia/reperfusion; this is referred to as post-cardiac arrest syndrome (PCAS). 1 Given that PCAS is closely associated with poor prognosis in patients who had ROSC after cardiac arrest, systematic approach and treatment to improve neurologic outcomes of these patients are necessary. 1 Prognostication of neurologic outcomes in comatose post-cardiac arrest patients is important, and the American Heart Association (AHA) guidelines recommend the use of clinical findings, electrophysiological and imaging modalities, and blood markers to predict and evaluate the neurologic outcomes of patients. 2 Of these, blood markers are influenced less by the drugs administered to the patients and are easier to access compared to other tests. 3 Neuron-specific enolase (NSE) and S-100B are the two most commonly examined blood markers; however, NSE and S-100B have low sensitivity and an inconsistent threshold for predicting neurologic outcomes after ROSC. 2
Procalcitonin (PCT) is known to be a blood marker specific for bacterial infection in septic patients. 4 The prognosis of patients with PCAS is closely associated with the duration of systemic ischemia and the secretion of various inflammatory mediators during reperfusion. 1 Systemic ischemia/reperfusion activates the immune system and coagulation pathways, which increase the risks of multiple organ failure and bacterial infection. 1 Such state of responses is similar to sepsis; 5 hence, PCT can be used to assess the severity of PCAS. A recent meta-analysis has reported the association between serum PCT level and outcomes of patients with PCAS. 6 However, most studies in this meta-analysis were reported in Europe (one study included Europe and the United States), and most were conducted on relatively small samples or at single centers. Moreover, patient characteristics in the meta-analysis were heterogeneous; arrest location of patients was out-of-hospital and/or in-hospital.
Therefore, this study aimed to identify the predictive value of serum PCT level as a prognostic marker for outcomes in patients hospitalized after out-of-hospital cardiac arrest (OHCA), using the data from the Korean Cardiac Arrest Research Consortium (KoCARC) registry, which is a multicenter research network registry with a relatively large sample size that well represents South Korea. Moreover, the study also sought to estimate the diagnostic accuracy of serum PCT level for predicting in-hospital mortality and unfavorable outcomes at hospital discharge of patients.
Methods
Study design
This retrospective observational study used a prospectively collected multi-center data registry. The KoCARC registry, which is a multicenter hospital-based collaborative research network registry, is a data-collecting system composed of risk and prognostic factors of patients after OHCA. The registry aims to improve the effectiveness and professionalism of research to produce evidence to strengthen the chain of survival for patients. 7 The KoCARC registry includes records of patients, who presented to the emergency department (ED) under pre-hospital resuscitation by emergency medical services (EMSs) after OHCA. Patients who had cardiac arrest of definite non-medical etiology, such as trauma, drowning, and poisoning, were excluded, as well as patients with terminal-stage illnesses without active treatment plan, those with documented do-not-resuscitate (DNR) orders, and those who were under hospice care at the time of onset of cardiac arrest. The KoCARC registry included 7576 patients after OHCA who presented to 36 participating hospitals across South Korea between 1 October 2015 and 30 June 2018.
Participants
The population of the present study comprises patients who presented to the ED in the hospital after OHCA. The following patients were included in the present study: (1) adult patients aged > 18 years, (2) patients hospitalized after OHCA who had successful ROSC pre-hospital or at the hospital, and (3) patients whose serum PCT levels were measured upon hospital presentation. This study excluded (1) patients aged < 18 years, (2) patients who did not survive at hospital admission, and (3) patients whose serum PCT levels were not measured upon hospital presentation.
Data collection
The KoCARC registry includes seven research fields classified based on the risk and prognostic factors of OHCA (epidemiology and prevention research, community resuscitation research, EMS resuscitation research, hospital resuscitation research, hypothermia and post-resuscitation care research, cardiac care resuscitation research, and pediatric resuscitation research), and each field has core and supplemental variables. In-hospital mortality and neurologic outcomes at hospital discharge are core variables of the patient information and outcome, and serum PCT level is a supplemental variable of the hospital resuscitation research field.
The neurologic outcome scores were divided into favorable (CPC (cerebral performance categories) 1 and 2) and unfavorable (CPCs 3–5) outcomes. Serum samples for PCT were collected immediately after ROSC in the hospital or upon hospital admission from patients who had successful ROSC at pre-hospital. We tried to exclude elevation of serum PCT level due to complications including bacterial infection after ROSC. Single measurement of serum PCT level was comparatively analyzed according to in-hospital mortality and neurologic outcomes at hospital discharge of patients hospitalized after OHCA. The following blood markers were also investigated: lactate, which has been found in a previous study to be associated with the prognosis of patients requiring intensive care; 8 NSE, which is a neurologic prognostic marker recommended in the AHA guidelines; 2 and white blood cell count (WBC), which is known to be associated with bacterial infections. C-reactive protein (CRP) was not investigated; CRP is not a core and supplemental variable in the KoCARC registry.
Among the variables studied in the registry, covariates were prognostic factors that have been reported to be significantly correlated to the survival and ROSC of patients after OHCA.6,9–13 The covariates used for univariate analysis were age, sex, presence of hypertension and diabetes, whether the cardiac arrest was witnessed, bystander CPR (chest compression), and shockable rhythm (ventricular fibrillation or pulseless ventricular tachycardia) on initial electrocardiogram (EKG) after cardiac arrest. Pre-hospital ROSC, the duration of cardiac arrest including the no-flow time (onset of cardiac arrest—onset of CPR) and low-flow time (onset of CPR—time of ROSC), the total amounts of epinephrine used in hospital, and the application of targeted temperature management (TTM) were also used. Initial vital signs, Glasgow Coma Scale (GCS), cause of arrest, patients’ premorbid states, and acute physiology as well as chronic health evaluation (APACHE II) or simplified acute physiology score (SAPS II) after ROSC were not investigated in the registry. Although history of patients including smoking, alcohol ingestion, and application of extracorporeal membrane oxygenation (ECMO) were investigated, they were excluded from the analysis as the data input rate was low.
The sample size was calculated based on a pilot study, which examined and compared the mean serum PCT level between non-survivors and survivors at hospital discharge among the patients hospitalized after OHCA. The mean serum PCT level of non-survivors and survivors were 6.35 ± 20.02 ng/dL and 1.25 ± 3.67 ng/dL, respectively. The estimated sample size calculation (G-power 3.1.9.2; Heine Heinrich University, Düsseldorf, German) revealed a required sample of 200 participants (effect size: 0.35, a-error: 0.05, power: 0.8); hence, at least 220 participants were needed for the analysis to account for a 10% dropout rate.
Statistical analysis
To investigate the predictive value of serum PCT level as a prognostic marker of adult patients hospitalized after OHCA, this study used in-hospital mortality as the primary outcome and neurologic outcome at hospital discharge as the secondary outcome.
All statistical analyses were performed with the SPSS software (version 21.0, IBM, Armonk, NY). Continuous variables were presented as median (quartile), and categorical variables were presented as number (percentage). Chi-square tests were conducted on categorical variables for univariate analysis, and differences were considered statistically significant when the p-value was less than 0.05. Independent samples t-tests were conducted when variables had normal distribution in both groups, whereas Mann–Whitney’s tests were conducted when the continuous variables were not normally distributed. For both independent samples t-tests and Mann–Whitney’s tests, the differences were considered significant when the p-value was less than 0.05. A multivariable logistic regression was conducted to investigate the independent influence of serum PCT level as a prognostic marker excluding the influence of already known prognostic factors for OHCA patients. Univariate analysis was conducted first to select covariates to be included in the multivariate regression model; here, variables with a p-value less than 0.10 and those selected by the researchers were included.
In addition, the diagnostic accuracy of serum PCT level for predicting in-hospital mortality and neurologic outcomes at hospital discharge of patients hospitalized after OHCA was determined through an analysis of receiver operating characteristic curves with area under the curve (ROC with AUC).
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board of Hanyang University Guri Hospital (IRB No. GURI 2015-12-001-001), which waived the requirement of informed consent. Approval for this study was obtained from the institutional review boards of each of the participating hospitals.
Results
Basic characteristics of the patients hospitalized after OHCA whose serum PCT levels were measured
The data of 7576 patients after OHCA were included in the KoCARC database between 1 October 2015 and 30 June 2018 (Figure 1). Among these, 254 patients were hospitalized with successful ROSC after OHCA and their serum PCT levels were measured and analyzed in this study (Table 1). The median age of the patients included in this study was 63.5 years (interquartile range (IQR): 53.0–76.0), and 64.6% were male. Out of the 254 patients, 139 (54.7%) died in the hospital and 185 (72.8%) showed unfavorable outcomes at hospital discharge. The median hospital length of stay was 8.0 days (IQR: 3.0–15.0).
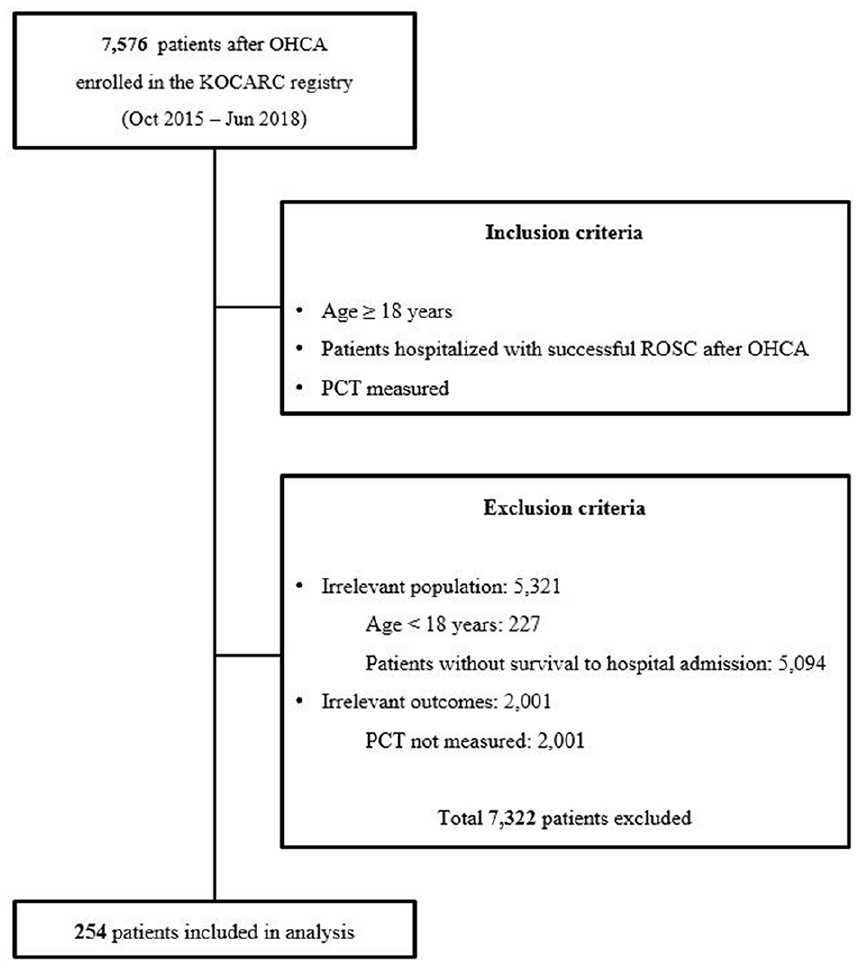
Flow diagram of included patients whose serum procalcitonin levels were examined and those who had neurologic outcomes recorded at hospital discharge.
Comparison of the characteristics between patients included in this study with serum procalcitonin level measured and those who did not, in total patients with return of spontaneous circulation after out-of-hospital cardiac arrest.
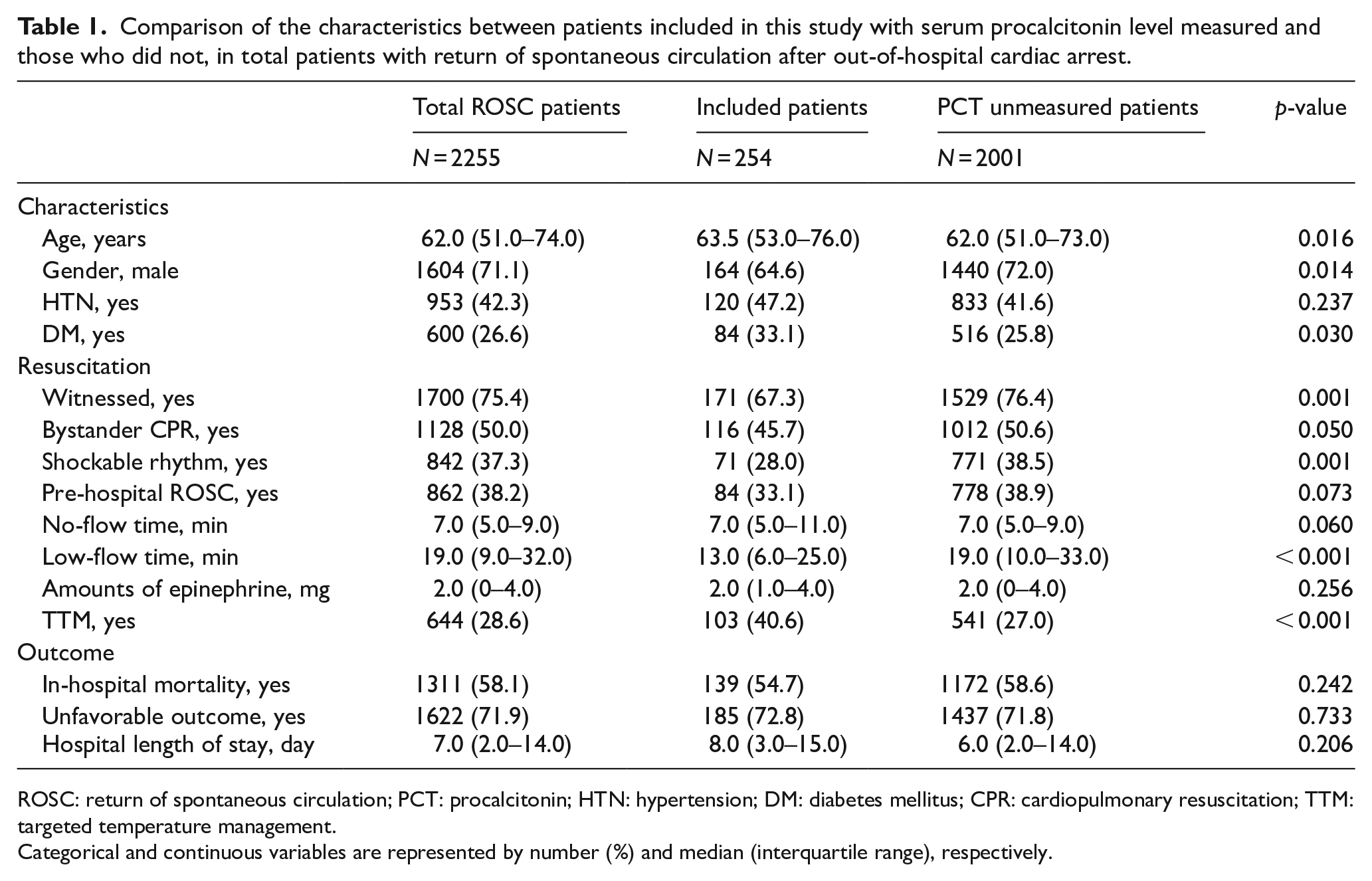
ROSC: return of spontaneous circulation; PCT: procalcitonin; HTN: hypertension; DM: diabetes mellitus; CPR: cardiopulmonary resuscitation; TTM: targeted temperature management.
Categorical and continuous variables are represented by number (%) and median (interquartile range), respectively.
Relationship between serum PCT level and in-hospital mortality of patients hospitalized after OHCA
The association of serum PCT level measured upon hospital presentation with in-hospital mortality of patients hospitalized after OHCA was analyzed (Table 2). Serum PCT level was significantly elevated in non-survivors compared to survivors (0.17 ng/dL (IQR: 0.05–0.18) vs. 0.10 ng/dL (IQR: 0.05–0.39), p = 0.017, respectively). Moreover, non-survivors had higher NSE and lactate levels compared to survivors. WBC did not differ significantly between the two groups (p = 0.316).
Univariate analysis for factors associated with in-hospital mortality.
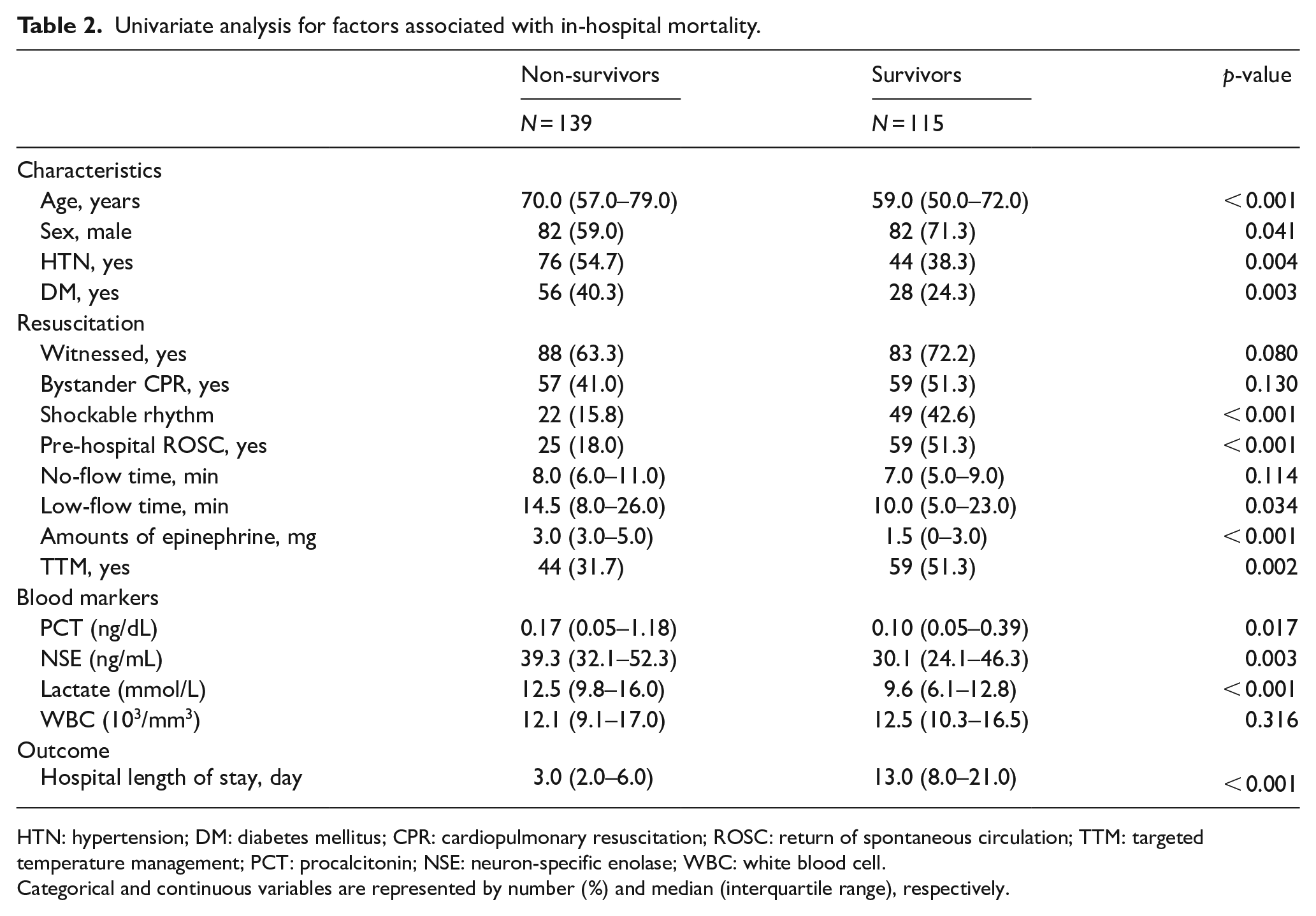
HTN: hypertension; DM: diabetes mellitus; CPR: cardiopulmonary resuscitation; ROSC: return of spontaneous circulation; TTM: targeted temperature management; PCT: procalcitonin; NSE: neuron-specific enolase; WBC: white blood cell.
Categorical and continuous variables are represented by number (%) and median (interquartile range), respectively.
The following variables showed a significant correlation with the in-hospital mortality of patients hospitalized after OHCA in the univariate analysis: age, sex, presence of hypertension and diabetes, shockable rhythm on initial EKG, pre-hospital ROSC, low-flow time, total amounts of epinephrine, application of TTM, and serum PCT level. Table 3 shows the results of the test of significance of variables that were thought to influence the in-hospital mortality of patients hospitalized after OHCA independently. The factors that independently influenced the in-hospital mortality of patients were age, shockable rhythm on initial EKG, total amounts of epinephrine, and application of TTM. Although age, sex, presence of hypertension, pre-hospital ROSC, low-flow time, and serum PCT level were significant in the univariate analysis, they were not significant in the multivariate analysis (p = 0.750).
Adjusted odds ratios for the factors associated with in-hospital mortality.
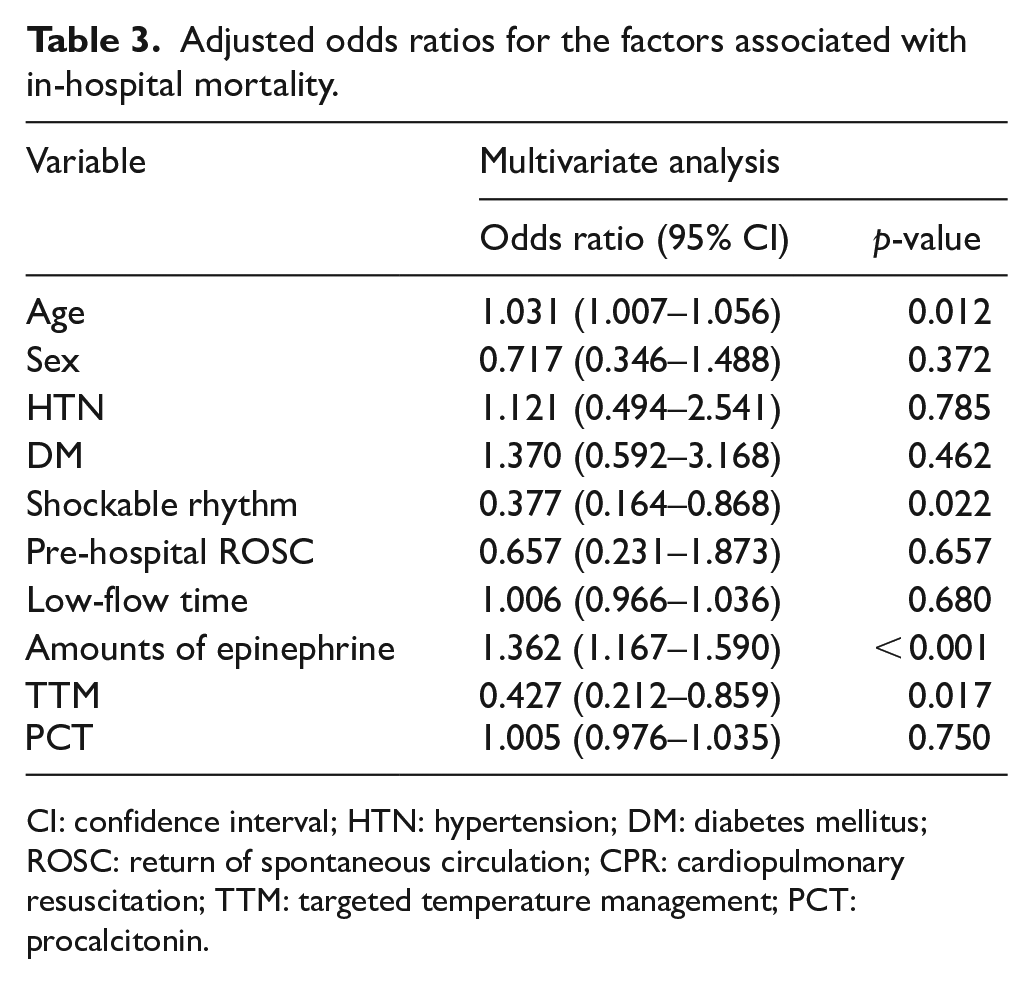
CI: confidence interval; HTN: hypertension; DM: diabetes mellitus; ROSC: return of spontaneous circulation; CPR: cardiopulmonary resuscitation; TTM: targeted temperature management; PCT: procalcitonin.
Relationship between serum PCT level and neurologic outcomes at hospital discharge of patients hospitalized after OHCA
The relationship between serum PCT level and neurologic outcomes at hospital discharge of patients hospitalized after OHCA was also analyzed (Table 4). Serum PCT level was significantly elevated in patients with unfavorable outcomes at hospital discharge compared to those with favorable outcomes (0.16 ng/dL (IQR: 0.06–1.10) vs. 0.07 ng/dL (IQR: 0.04–0.22), p < 0.001, respectively). Moreover, the unfavorable outcome group at hospital discharge had higher lactate levels than the favorable outcome group. NSE and WBC did not show significant difference between the groups.
Univariate analysis of factors associated with neurologic outcome at hospital discharge.

HTN: hypertension; DM: diabetes mellitus; CPR: cardiopulmonary resuscitation; ROSC: return of spontaneous circulation; TTM: targeted temperature management; PCT: procalcitonin; NSE: neuron-specific enolase; WBC: white blood cell.
Categorical and continuous variables are represented by number (%) and median (interquartile range), respectively.
The following variables showed significant correlation with neurologic outcomes at hospital discharge of patients hospitalized after OHCA in the univariate analysis: age, sex, presence of hypertension and diabetes, shockable rhythm on initial EKG, pre-hospital ROSC, total amounts of epinephrine, application of TTM, and serum PCT level. Table 5 shows the results of the test of significance of variables that were thought to independently influence the neurologic outcomes of patients hospitalized after OHCA. The factors that independently influenced the neurologic outcomes at hospital discharge of patients were age, shockable rhythm on initial EKG, pre-hospital ROSC, and the total amounts of epinephrine. Although sex, presence of hypertension and diabetes, application of TTM, and serum PCT level were significant in the univariate analysis, they were not significant in the multivariate analysis.
Adjusted odds ratios for the factors associated with unfavorable outcome at hospital discharge.
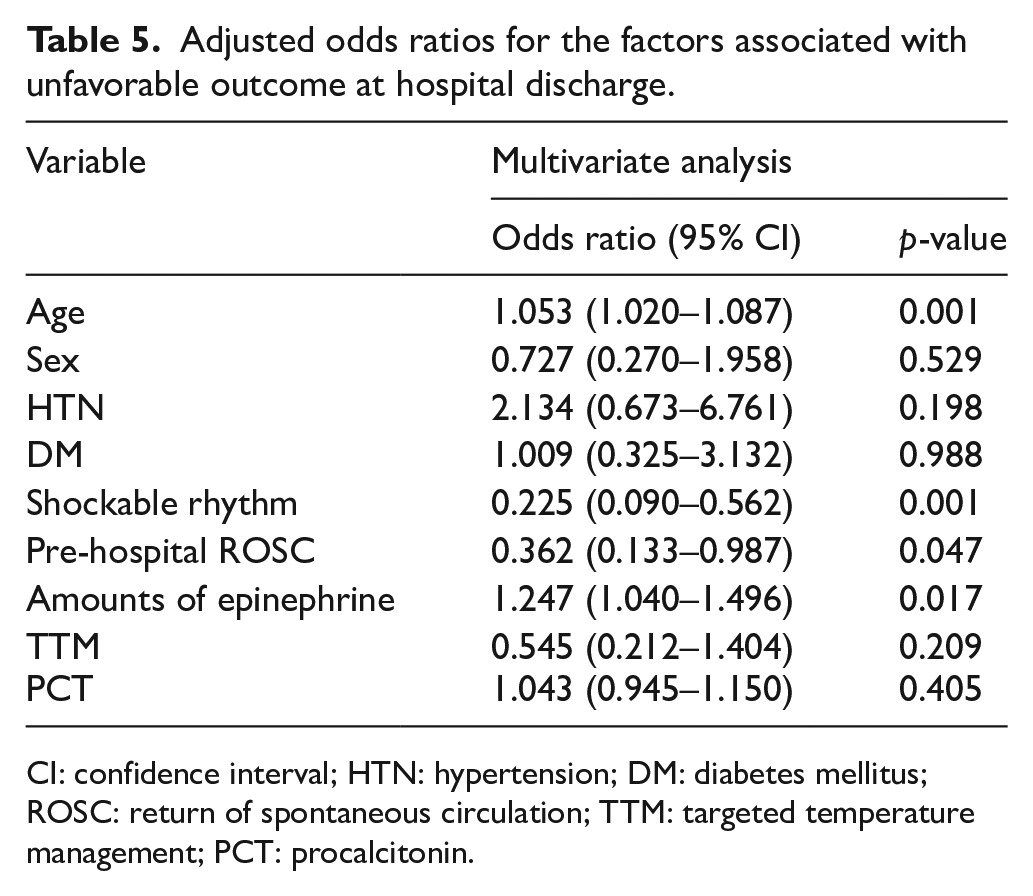
CI: confidence interval; HTN: hypertension; DM: diabetes mellitus; ROSC: return of spontaneous circulation; TTM: targeted temperature management; PCT: procalcitonin.
Diagnostic accuracy of serum PCT level for predicting in-hospital mortality and unfavorable outcome at hospital discharge
The diagnostic accuracy of blood marker tests for predicting in-hospital mortality and unfavorable outcome at hospital discharge of patients hospitalized after OHCA was analyzed (Figure 2). ROC with AUC analysis was conducted for serum PCT level, lactate level, and NSE (Table 6).
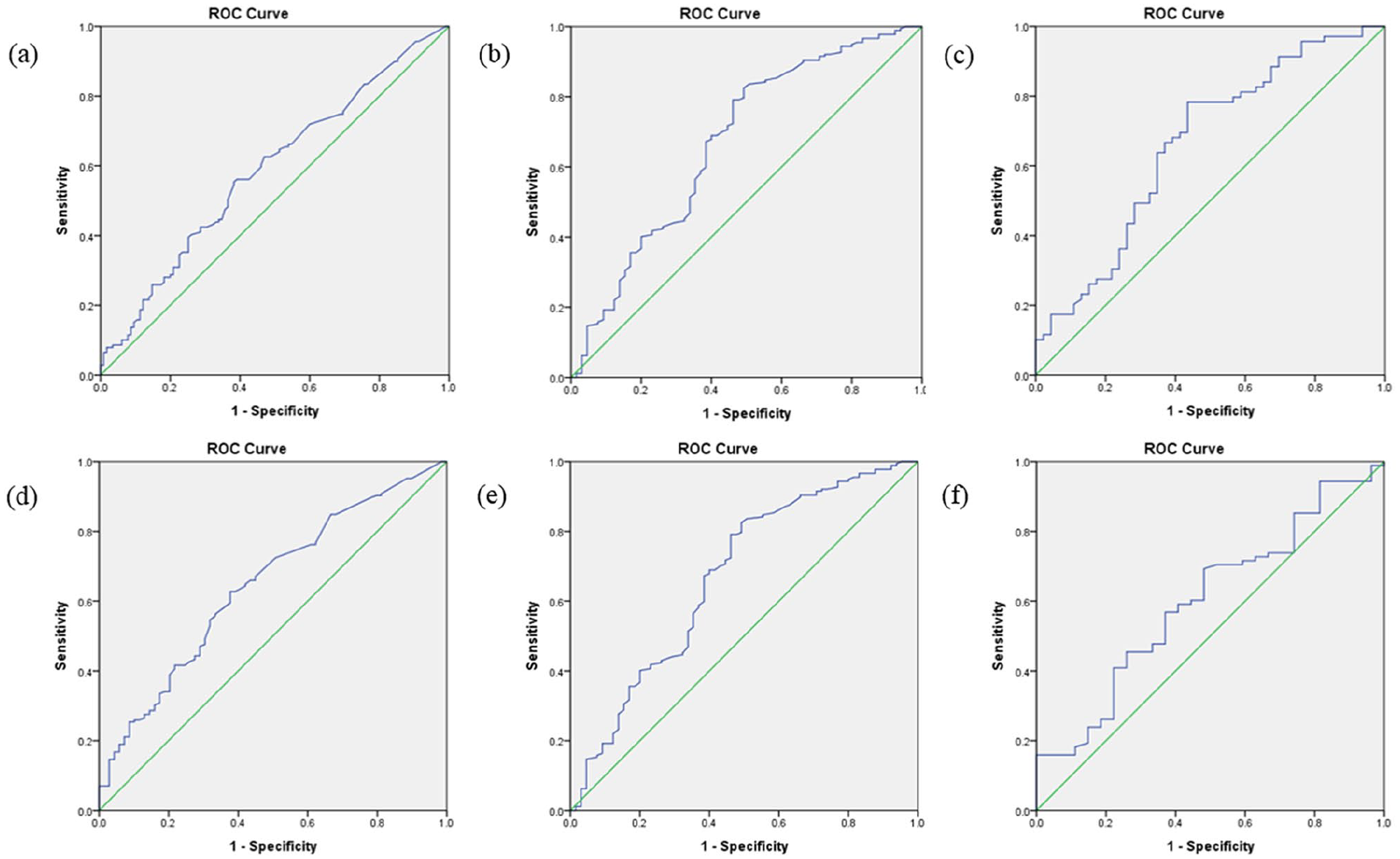
ROC curve analysis of (a) procalcitonin, (b) lactate, and (c) neuron specific enolase for predicting in-hospital mortality and ROC curve analysis of (d) procalcitonin, (e) lactate, and (f) neuron-specific enolase for predicting unfavorable outcome (cerebral performance categories 3–5) at hospital discharge in out-of-hospital cardiac arrest patients.
AUC and cut-off value of procalcitonin, lactate, and neuron-specific enolase for predicting in-hospital mortality and unfavorable outcome at hospital discharge in patients hospitalized after out-of-hospital cardiac arrest.
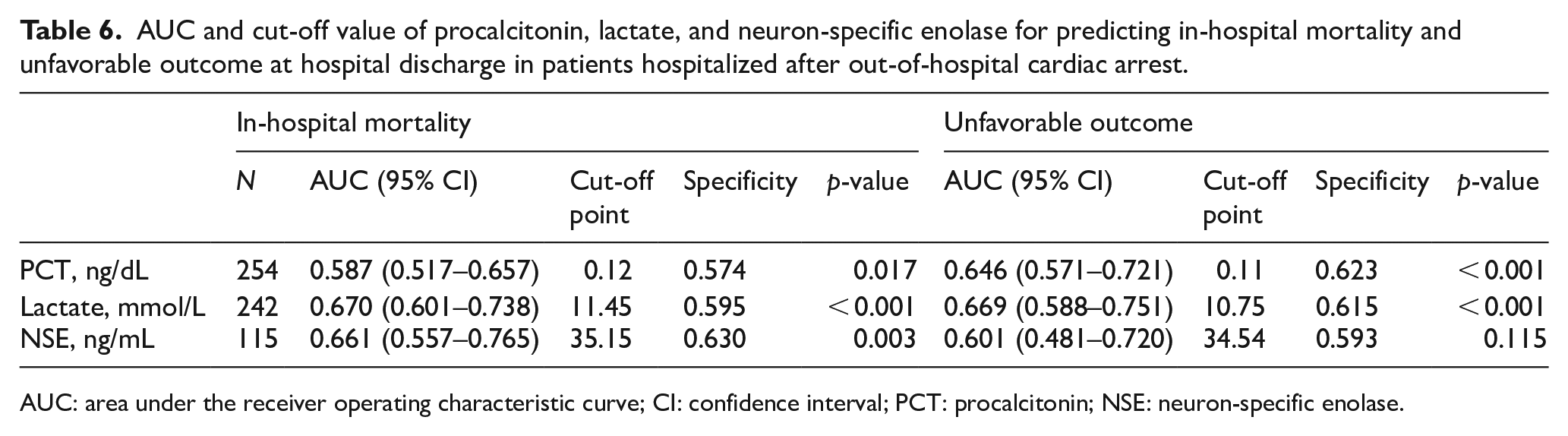
AUC: area under the receiver operating characteristic curve; CI: confidence interval; PCT: procalcitonin; NSE: neuron-specific enolase.
The diagnostic accuracy of serum PCT level for predicting in-hospital mortality was 0.587 (95% CI: 0.517–0.657, p = 0.017, cut-off = 0.12 ng/dL, specificity = 57.4%), while the diagnostic accuracy of lactate level for predicting in-hospital mortality was 0.670 (95% CI: 0.601–0.738, p < 0.001), and that of NSE was 0.661 (95% CI: 0.557–0.765, p = 0.003).
In addition, the diagnostic accuracy of serum PCT level for predicting unfavorable outcome at hospital discharge was 0.646 (95% CI: 0.571–0.721, p < 0.001, cut-off = 0.11 ng/dL, specificity = 62.3%) and that of lactate level for predicting unfavorable outcome was 0.669 (95% CI: 0.588–0.751, p < 0.001). NSE did not show a significant diagnostic accuracy for predicting unfavorable outcome at hospital discharge of patients hospitalized after OHCA.
Discussion
This study analyzed the association between serum PCT level measured in patients hospitalized after OHCA and their outcomes. Elevated serum PCT level in patients was associated with increased in-hospital mortality and unfavorable outcome. However, serum PCT level was not considered as an independent factor for predicting the outcomes of patients. Moreover, serum PCT level had a low diagnostic accuracy for predicting in-hospital mortality and unfavorable outcome at hospital discharge of patients.
PCT is a peptide precursor to calcitonin, a hormone secreted by the thyroid gland to regulate calcium levels, and is produced by enzymatic degradation of pre-PCT by endopeptidase. 10 PCT consists of 116 amino acids, and its synthesis is regulated by the calcitonin-1 gene (CALC-1) on chromosome 11. Serum PCT level starts to increase within 2–3 h due to inflammatory responses and peaks after 6–12 h; its half-life is 20–24 h. 14 Therefore, PCT is known to be helpful in the early diagnosis of sepsis, systemic inflammatory response, and in planning antibiotic treatment in patients with bacterial infection. 4
PCT is also known to increase in patients with PCAS. 7 The level of calcitonin gene–related peptide (CGRP) increases during ischemia/reperfusion of the brain, which promotes the production of CALC-1 and increases serum PCT level. 4 Patients with successful ROSC after cardiac arrest also have brain ischemia/reperfusion, similar to acute ischemic stroke patients; and the serum PCT levels may increase without bacterial infection through the same mechanism. 15 Annborn et al. reported that increased serum PCT level in patients with PCAS is not specific for bacterial infection but rather reflects nonspecific inflammatory responses. 10 Moreover, the authors explained that serum PCT level is a marker that shows the duration of systemic ischemia during cardiac arrest. Serum PCT level measured to diagnose bacterial infection in patients with PCAS has been reported to carry a low diagnostic accuracy.16,17 Tang et al., 18 who conducted a meta-analysis with 18 studies, also reported that serum PCT level has a low diagnostic accuracy in diagnosing sepsis from systemic inflammatory responses in critically ill patients who were admitted at the intensive care unit.
However, serious bacterial infection or sepsis may arise in patients with PCAS, which may influence the prognosis of patients with successful ROSC. 19 Bacterial infection, including pneumonia commonly observed in patients with PCAS, has been reported to significantly increase the serum PCT level. 20 Given that this may cause confusion in predicting the prognosis of patients, systemic inflammatory responses due to infection should be ruled out if serum PCT level increases in patients with PCAS. Moreover, elevated serum PCT level may guide the attending physician on antibiotics treatment for underlying bacterial infection, which may also affect the prognosis of patients if there is any significant infection. Thus, to identify the more precise association between serum PCT level and the prognosis in patients with PCAS, a further study of patients excluding those whose cardiac arrest was caused by bacterial infection or sepsis is needed. Moreover, early complications of bacterial infection from patients with PCAS should be evaluated and excluded.
The diagnostic accuracy of serum PCT level in this study was lower than that measured in previous studies to predict in-hospital mortality. 11 Serum PCT also had a low diagnostic accuracy for predicting unfavorable outcome at hospital discharge. Although NSE did not show significant results, the diagnostic accuracy of serum PCT level was lower than that of lactate level. The diagnostic accuracy of serum PCT level was also lower than that reported by previous studies to predict unfavorable outcomes of patients.10,12,13
South Korean OHCA patients were included in this study, and it was conducted in Northeast Asia, not in Europe or America. Early chest compressions and defibrillation are important factors that influence the survival rate of OHCA patients.21,22 The conditions of pre-hospital CPR in Korea may be different from that of other countries. Pre-hospital CPR in South Korea showed a relatively low frequency of shockable rhythms on initial EKG after cardiac arrest, low rate of pre-hospital defibrillation, low frequency of bystander CPR (worldwide = 32% vs. South Korea = 12.2%),23,24 and a relatively long median time required until defibrillation (Europe = 7–11 min, United States and Canada = 8.7 min, Japan = 9 min vs. South Korea = 17 min).25–27 According to Berdowski et al., 28 in a systematic review and meta-analysis conducted with 67 prospective studies (30 European, 24 North American, 7 Asian, and 6 Australian) showed that the worldwide frequency of shockable rhythm on EKG in OHCA patients was 26.9% (Europe = 35.2%, North America = 28.1%, Asia = 11.2%, Australia = 39.8%), which differs significantly from the frequency of 11.1% in South Korea.
Moreover, the survival rate of OHCA patients depended on the efficiency of EMSs in local communities and the supply of automated external defibrillators. 29 The number of acute cardiac arrest patients in South Korea increased approximately 1.5-fold in 12 years between 2006 (19,480) and 2016 (29,382). Assuming that approximately 30,000 cases of cardiac arrest are seen in South Korea every year, approximately 9.2% of all cases would have been entered into the KoCARC registry. The 36 participating hospitals for the KoCARC registry are large hospitals located in cities with populations of more than 200,000, and the characteristics of patients presenting to these hospitals may differ from those of the general OHCA patients.
Serum PCT level is a supplemental variable of the KoCARC registry and is not routinely measured from patients after OHCA. It is possible that serum PCT level was measured selectively as patients included in this study were thought to likely have ROSC, or measured additionally to identify the cause of cardiac arrest when its cause is unclear after successful ROSC. Moreover, it may also have been measured additionally to confirm complications when patients showed septic conditions after ROSC. To more accurately analyze the predictive values of serum PCT level as a prognostic marker in PCAS patients, prospective studies measuring serum PCT level in more patients with successful ROSC are required.
This study, which is a retrospective observational study conducted using a prospectively collected multi-center data registry, has the following limitations. First, although the KoCARC registry was used to better represent South Korea, the results are applicable only to South Koreans and the actual results may differ depending on race or country. Second, serum PCT level was measured in only a small proportion of adult patients hospitalized after OHCA. Given that the patients included in this study and all patients with successful ROSC had different basic characteristics, there could have been a selection bias. Serum PCT level, which is a supplemental variable of the KoCARC registry, was measured in a small proportion of patients (3.5%), and the time of measurement of serum PCT level could be a variable. Third, as limitations for a registry-based study, bias in data entry and extraction as well as statistical bias from missing values may have been present. Fourth, the patients included in this study were admitted for a median of 8 days, and their prognosis might have differed from this study’s results if long-term prognosis after 30 days was evaluated. Given that previous research suggests that patients’ neurologic outcomes at discharge may change up until 6 months later, 30 additional studies evaluating the long-term outcomes of patients with successful ROSC and their serum PCT level are required.
NSE and S-100B are the most commonly used blood markers for predicting and evaluating the outcomes of PCAS patients. 2 However, many studies have shown that NSE and S-100B measured 24 h after ROSC are significant.31–33 To predict and evaluate the prognosis of PCAS patients earlier, future studies would be needed to investigate appropriate combinations of serum PCT level and other blood markers, such as conventionally used NSE and S-100B.
Conclusion
Elevated serum PCT level measured at hospital presentation of patients hospitalized after OHCA was associated with increased in-hospital mortality and unfavorable outcome. However, serum PCT level could not be considered as an independent factor to predict the outcomes of patients, and serum PCT level had a low diagnostic accuracy for predicting in-hospital mortality and unfavorable outcome.
Footnotes
Acknowledgements
The authors would like to acknowledge and thank the investigators from all participating hospitals of KoCARC: Do Kyun Kim (Seoul National University Hospital), Sang Kuk Han, Phil Cho Choi (Kangbuk Samsung Medical Center), Sang O Park, Jong Won Kim (Konkuk University Medical Center), Han Sung Choi, Jong Seok Lee (Kyung Hee University Hospital), Sung Hyuk Choi, Young Hoon Yoon (Korea University Guro Hospital), Su Jin Kim (Korea University Anam Hospital), Min Seob Sim, Gun Tak Lee (Samsung Medical Center), Shin Ahn (Asan Medical Center), Jong Whan Shin (SMG-SNU Boramae Medical Center), Sang Hyun Park, Keun Hong Park (Seoul Medical Center), In Cheol Park, Yoo Seok Park (Yonsei University Severance Hospital), Tae Young Kong (Yonsei University Gangnam Severance Hospital), Kyoung Won Lee, Chu Hyun Kim (Inje University Seoul Paik Hospital), Youngsuk Cho (Hallym University Kangdong Sacred Heart Hospital), Gu Hyun Kang, Yong Soo Jang (Hallym University Kangnam Sacred Heart Hospital), Tai Ho Im, Jae Hoon Oh (Hanyang University Seoul Hospital), Seok Ran Yeom, Sang Kyoon Han (Pusan National University Hospital), Jae Hoon Lee (Dong-A University Hospital), Jeong Bae Park, Hyun Wook Ryoo (Kyungpook National University Hospital), Kyung Woo Lee, Tae Chang Jang (Daegu Catholic University Medical Center), Jae-hyug Woo (Gachon University Gil Medical Center), Woon Jeong Lee, Seon Hee Woo (The Catholic University of Korea Incheon St. Mary’s Hospital), Sung Hyun Yun, Tae Jin Cho (Catholic Kwandong University International St. Mary’s Hospital), Sun Pyo Kim, Yong Jin Park (Chosun University Hospital), Jin Woong Lee, Wonjoon Jeong (Chungnam National University Hospital), Sung Soo Park, Jae Kwang Lee (Konyang University Hospital), Ryeok Ahn, Wook Jin Choi (Ulsan University Hospital), Young Gi Min, Eun Jung Park (Ajou University Hospital), You Hwan Jo, Joong Hee Kim (Seoul National University Bundang Hospital), In Byung Kim, Ki Ok Ahn (Myongji Hospital), Han Jin Cho (Korea University Ansan Hospital), Seung Cheol Lee, Sang Hun Lee (Dongguk University Ilsan Hospital), Young Sik Kim, Young Rock Ha (Bundang Jesaeng Hospital), Jin Sik Park, Myoung Woo Lee (Sejong Hospital), Dai Han Wi (Wonkwang University Sanbon Hospital), Ok Jun Kim, Tae Nyoung Chung (Cha University Bundang Medical Center), Soon Joo Wang, Hang A Park (Hallym University Dongtan Sacred Heart Hospital), Jun Hwi Cho, Chan Woo Park (Kangwon National University Hospital), An Mu Eob, Tae Hun Lee (Hallym University Chuncheon Sacred Heart Hospital), Sang Chul Kim, Hoon Kim (Chungbuk National University Hospital), Han Joo Choi, Chan Young Koh (Dankook University Hospital), Jung Won Lee, Dong Wook Lee (Soonchunhyang University Cheonan Hospital), Tae Oh Jung, Jae Chol Yoon (Chonbuk National University Hospital), Dai Hai Choi, Jung Tae Choi (Dongguk University Gyeongju Hospital), Jin Hee Jeong, Soo Hoon Lee (Gyeongsang National University Hospital), Ji Ho Ryu, Maeng Real Park (Pusan National University Yangsan Hospital), Won Kim (Cheju Halla General Hospital), Sung Wook Song, Woo Jung Kim (Jeju National University Hospital), Joon-myoung Kwon, Eui Hyuk Kang (Mediplex Sejong Hospital), Sang Chan Jin, Tae-kwon Kim (Keimyung University Dongsan Medical Center), Seong Chun Kim (Gyeongsang National University Changwon Hospital).
They would also like to thank the steering committee comprising the following individuals: Sung Oh Hwang (Chair, Wonju Severance Christian Hospital), Sang Do Shin (Chair of Steering Committee, Seoul National University hospital), Hyuk Jun Yang (Advisory Committee, Gachon University Gil hospital), Sung Phil Chung (Data Safety and Management Board, Gangnam Severance Hospital), Sung Woo Lee (Security and Monitoring Board, Korea University Anam hospital), Kyung Jun Song (Secretariat, SMG-SNU Boramae Medical Center), Seung Sik Hwang (Epidemiology and Prevention Research Committee, Seoul National University), Gyu Chong Cho (Community Resuscitation Research Committee, Hallym University Kangdong Sacred Heart Hospital), Sung Woo Moon (Emergency Medical Service Resuscitation Research Committee, Korea University Ansan Hospital), Kyoung Chul Cha (Hospital Resuscitation Research Committee, Wonju Severance Christian Hospital), Won Young Kim (Hypothermia and Post-Resuscitation Care Research Committee, Asan Medical Center), Sang Hoon Na (Cardiac Care Resuscitation Research Committee, Seoul National University Hospital), Young Ho Kwack (Pediatric Resuscitation Research Committee, Seoul National University hospital). To member of Secretariat: Joo Yeong Kim (Korea University Ansan hospital), Jeong Ho Park (Seoul National University hospital), Sun Young Lee (Seoul National University hospital), and Jung Eun Kim (Seoul National University hospital); and they also thank the National Fire Agency for providing pre-hospital EMS data.
Author contributions
H.S., Y.L., and H.J.C. contributed to study concept and design, and analysis and interpretation of the data. H.S., C.K., and H.J.C. contributed to acquisition of the data and critical revision of the manuscript for important intellectual content. H.S. and Y.L. contributed to drafting of the manuscript. All authors contributed to statistical expertise.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data
The datasets generated and/or analyzed during the current study are available from corresponding author.
Ethical approval
The study protocol was reviewed and approved by the Institutional Review Board of Hanyang University Guri Hospital (IRB No. GURI 2015-12-001-001), which waived the requirement of informed consent. Approval for this study was obtained from the institutional review boards of each of the 64 participating hospitals.
Human rights
The principles of autonomy and confidentiality were followed.