
Abstract
Background:
Emergency department has been shown to be suitable for conducting screening and interventions for at-risk drinking groups. Simple screening test is needed for crowded environments such as the emergency department.
Objective:
This study explores the validity of screening test for at-risk drinking, which was a newly developed abbreviated version of the alcohol use disorder identification test, among patients in the emergency department.
Method:
A survey was conducted at the emergency department of an academic tertiary hospital in South Korea during 4 months. All patients, who visited the emergency department and were between 19 and 65 years of age, answered the alcohol use disorder identification test questionnaire. In this study, at-risk drinking was identified using alcohol use disorder identification test.
Results:
The screening test was completed by 178 patients in this study. At-risk drinking group comprises 78 patients (43.8%). The cut-off values of screening test for at-risk drinking were 3 for males and 2 for females. As a result, the sensitivity/specificity was 98.0/93.5 and 96.4/79.6 for men and women, respectively. Area under the receiver operating characteristics of screening test for at-risk drinking was 0.9 and 0.9 in men and women, respectively.
Conclusion:
screening test for at-risk drinking is a useful test that easily identifies at-risk drinking. It is expected that this test can facilitate screening for at-risk drinking in emergency department setting.
Keywords
Introduction
Consumption of alcohol is an important concern in the field of public health, since it is a contributing factor in increasing incidences of disease and injury. 1 Efforts have been made to reduce the incidence of harmful alcohol consumption. Studies show that identifying at-risk drinking behaviors and conducting brief interventions are effective ways to reduce harmful alcohol consumption.2,3 There are several spectrums of drinking behaviors, among which, at-risk drinking is milder than alcohol abuse or dependence. At-risk drinking means a pattern of alcohol consumption that increases the risk of harmful consequences for the user or others, and is defined by the amount of alcohol consumed. 2 The amount of alcohol consumed in at-risk drinking has been diversely defined as (1) a score of eight for men and seven for women using the whole alcohol use disorder identification test screening tool;4,5 (2) four standard drinks per day or 14 standard drinks per week for men, and three standard drinks per day or seven standard drinks per week for women and elders;6–8 (3) alcohol intake per week being over 280 g for men and over 168 g for women; 9 and (4) alcohol intake per day being 40 g for men and 20 g for women. 10 In the case of at-risk drinking, brief interventions at an early stage are known to be effective in reducing alcohol intake. 11 Emergency departments have been shown to be suitable for conducting screening and interventions for this problem drinking (including at-risk drinking) groups. 12 In the United States, alcohol abuse is one of the main public health problems among young adults.13,14 According to data from the Korea National Health and Nutrition Examination (KNHANES) conducted from 2007 to 2015, the proportion classified in the at-risk drinking group was 41.2% among those in their 20s, 35.5% among those in their 30s, 33.4% among those in their 40s, and 29.0% among those in their 50s. However, the proportion of at-risk drinking group decreases among those in their 60s (21.5%), 13.7% among those in their 70s, and 5.9% among those in their 80s and above. 15 Given these large proportions, screening and brief intervention for at-risk drinking among young and middle-aged adult is important.
The alcohol use disorder identification test (AUDIT) developed by the World Health Organization (WHO) is used worldwide to screen at-risk drinking. 16 The development of AUDIT was based on multinational studies, starting in 1987. The developers collected data using 150 questions and sorted them into conceptual groups. Four groups were selected through correlation analysis and factor analysis of intra-scale reliability and daily mean alcohol consumption. Subsequently, the developers selected two or three questions per group, considering the weighted mean item-to-total correlation coefficient in each of the four groups; from these questions, they assembled the AUDIT, consisting of ten questions. The AUDIT consists of three parts, questions 1–3 (Q1–Q3) relate to the amount and frequency of drinking, questions 4–6 (Q4–Q6) relate to alcohol dependence symptoms, and questions 7–10 (Q7–Q10) relate to alcohol-related problems. However, a simpler screening test is needed for crowded environments such as an ED. Screening test for at-risk drinking (STAD) is a new abbreviated version of the AUDIT, developed in 2018. It consisted of the third (How often do you have five or more drinks on one occasion?) and seventh questions (How often during the last year have you had a feeling of guilt or remorse after drinking?) based on confirmatory factor analysis of AUDIT. 17 This study explored the validity STAD among patients in the ED
Methods
Setting and data collection
A cross-sectional survey was conducted among patients in the ED of an academic tertiary hospital in South Korea from 1 October 2018 to 31 January 2019. Inclusion criteria were all patients who visited the ED and were from 19 to 65 years of age, and who agreed to answer the AUDIT questionnaire (Supplemental Appendix 1). Exclusion criteria were patients who were under the age of 18 or over 66, were mentally unstable, had an unstable hemodynamic status, or refused to participate in the study.
Emergency medicine trainees explained the screening test for at-risk drinking to the patients while they waited for tests or procedures at the ED. If the patients refused to participate in the study, the process was discontinued at this stage. For patients who agreed to participate in the study, the AUDIT questionnaire (10 questions which included STAD questions) was distributed for completion after obtaining consent. Other patient information was collected, including details of age, gender, the mode of arrival, Korean triage and acuity scale (KTAS) results, diagnosis, and disposition. KTAS was developed by the Korean Ministry of Health and Welfare’s research project based on the Canadian emergency department Triage and Acuity Scale. It consists of five acuity levels; from level 1 (resuscitation) to level 5 (non-urgent). 18 Study data were collected over 24 h, 7 days a week.
Outcome measure
In this study, at-risk drinking was diagnosed using AUDIT, which was developed by WHO in 1989 and used to screen at-risk drinking. The cut-off point for at-risk drinking was determined as 8 or more for men and 7 for women. 19
For validation of STAD, the optimal cut-off values, sensitivity, specificity, and area under the receiver operating characteristics (AUROC) of STAD were analyzed. Furthermore, we compared AUROC of STAD with other abbreviated version of AUDIT, AUDIT-C (consumption, Q1–3) and AUDIT-QF (quantity frequency, Q1–2), which were widely used existing abbreviated tests.
Statistical analysis
The differences in variables between at-risk drinking and non-at-risk drinking were analyzed using Student’s t-test and chi-square test. Student’s t-test was used to compare continuous variables between two groups, and the chi-square test was used to compare categorical variables. Data were analyzed using PASW 18 (SPSS, Chicago, IL, USA). MedCalc Statistical Software version 19.1.3 (MedCalc Software bv, Ostend, Belgium; https://www.medcalc.org; 2019) was used to determine the adequate cut-off points of STAD based on the results of AUDIT. When these data are known, MedCalc program calculates the optimal criterion and associated sensitivity and specificity. MedCalc calculated bias-corrected and accelerated (BCa) bootstrapped 95% confidence intervals 20 for these parameters. When a test is used for screening or to exclude a diagnostic possibility, a cut-off value with a higher sensitivity may be selected. When a test is used to confirm a disease, a higher specificity may be required. We drew a receiver operation characteristic (ROC) curve and estimated an AUROC using sensitivity and specificity of each interval in males and females. The method of DeLong et al. 21 for the calculation of the standard error of the area under the curve (AUC) and of the difference between two AUCs were used.
Ethics statement
This study was approved by the institutional review board (IRB) of Ewha Womans University Mokdong hospital (IRB No. 2018-07-080-001), and informed consent was obtained from each patient.
Results
During the study, 19,119 patients were admitted to the ED. There were 9617 patients aged 19–65 years. The number of patients invited to participate in the study, excluding those who died in the ED, had unstable vital signs, or decreased mentality (lack of capacity to consent), was 6611. Except for patients who declined to participate in the study, the screening test was completed by 178 patients, giving a response rate of 2.7%. Among them, 96 patients (53.9%) were men and 82 patients (46.1%) were women. The mean age of patients was 39.4 years. The most common mode of arrival to the ED was walk-in (76.9%). Diagnosis showed that 78.7% of the participants were disease patients and 21.3% were injury patients. Acute abdomen was the most common diagnosis among those with diseases (23.0%). Sprain was the most common diagnosis among those with injury (21.3%). After treatment at the ED, 148 patients (83.1%) were discharged. The at-risk drinking group comprises 78 patients (43.8%). There is no significant difference in demographic characteristics between the at-risk drinking and the non-at-risk drinking groups (Table 1).
Demographic characteristics of study population.
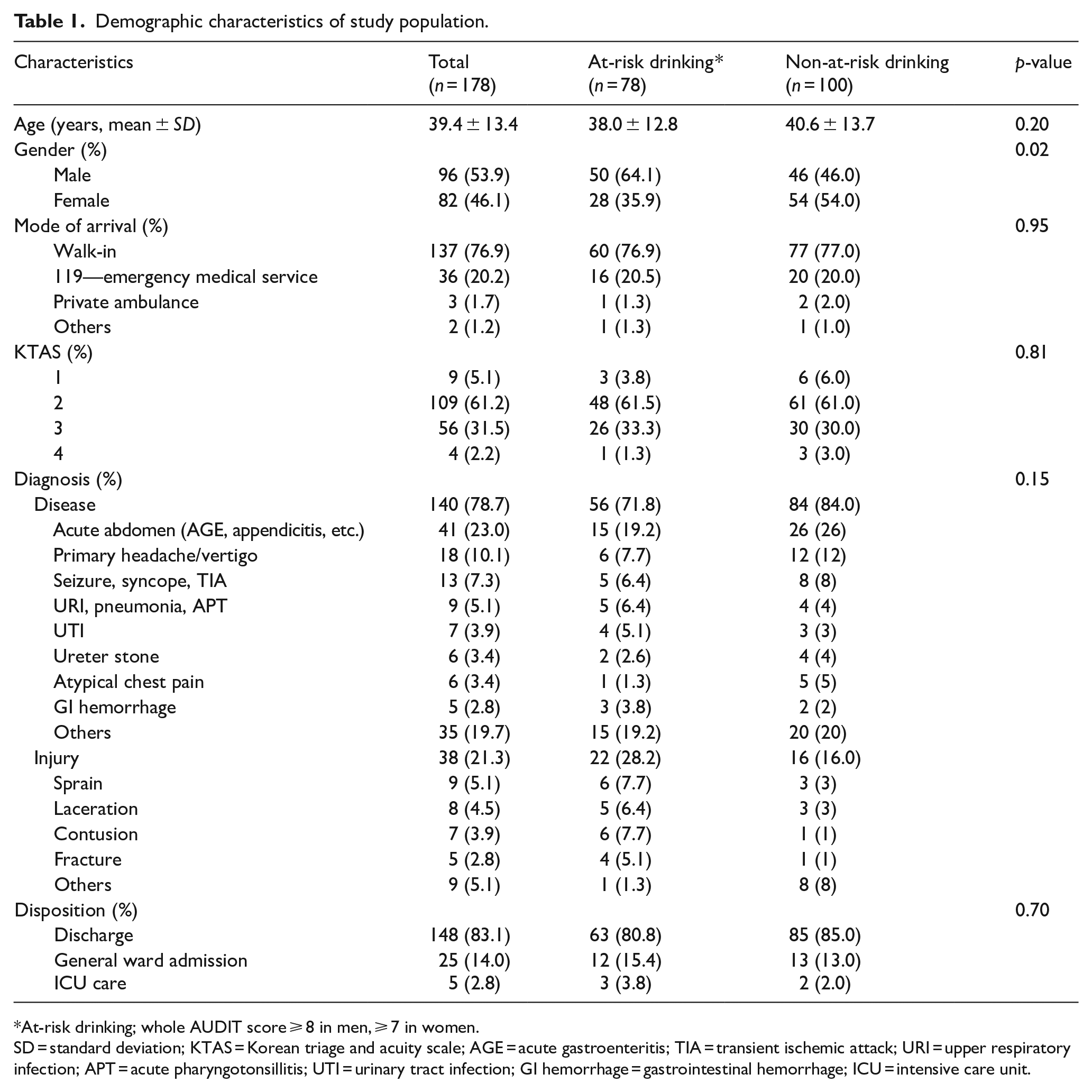
At-risk drinking; whole AUDIT score ⩾ 8 in men, ⩾ 7 in women.
SD = standard deviation; KTAS = Korean triage and acuity scale; AGE = acute gastroenteritis; TIA = transient ischemic attack; URI = upper respiratory infection; APT = acute pharyngotonsillitis; UTI = urinary tract infection; GI hemorrhage = gastrointestinal hemorrhage; ICU = intensive care unit.
The cut-off values of STAD in this study were 3 for males and 2 for females. As a result, the sensitivity/specificity was 98.0/93.5 and 96.4/79.6 for men and women, respectively (Table 2). AUROC of STAD was 0.98 and 0.96 in men and women, respectively. We compared the utility of the existing abbreviated tests AUDIT-QF and AUDIT-C with that of the new abbreviated test, STAD. In AUROC, there was no significant difference between AUDIT-QF, consisting of two questions, and STAD. In addition, there was no significant difference between AUDIT-C, consisting of three questions, and STAD (Figure 1, Table 3).
Cut-off values, sensitivities, and specificities of STAD.
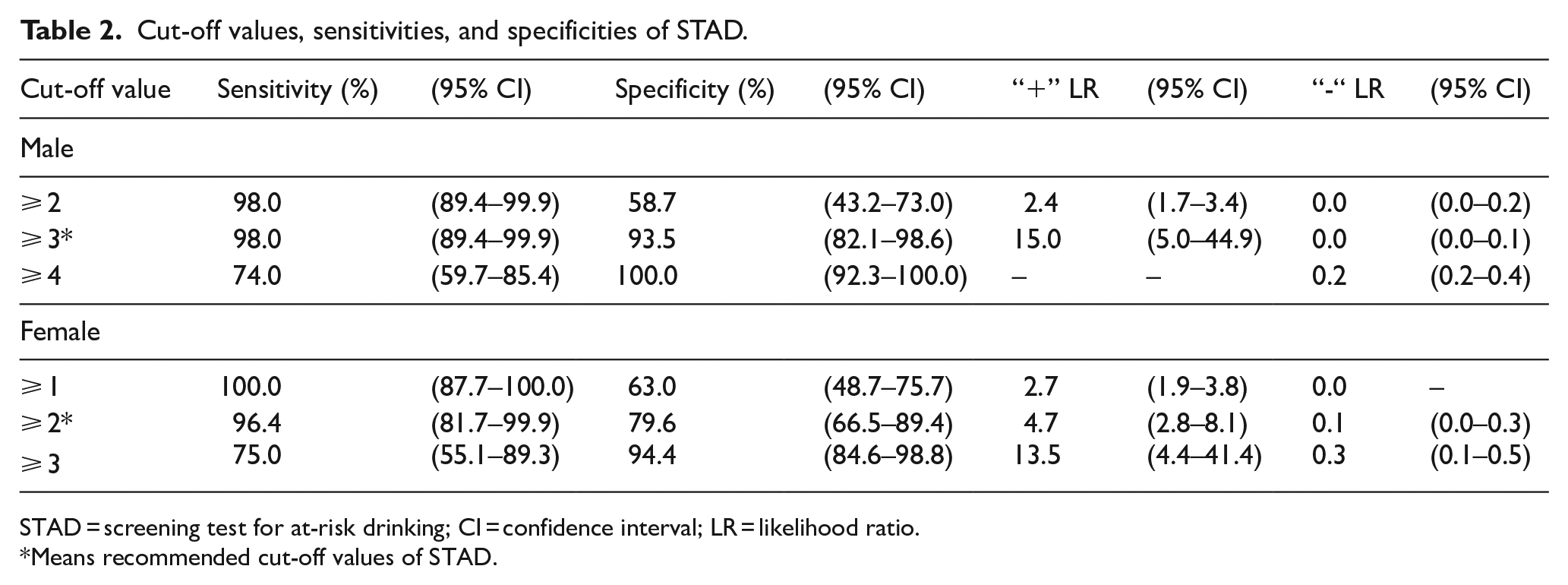
STAD = screening test for at-risk drinking; CI = confidence interval; LR = likelihood ratio.
Means recommended cut-off values of STAD.
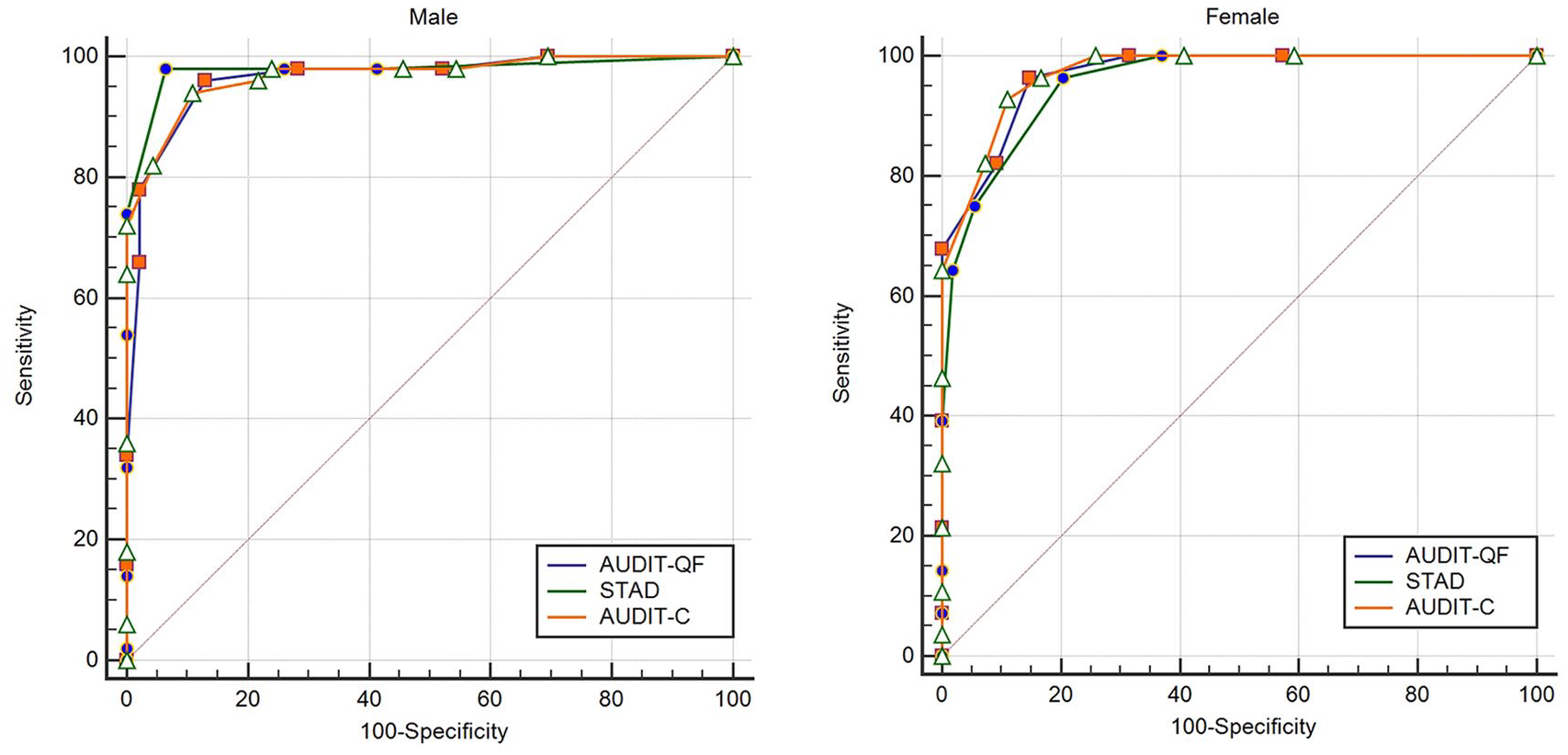
AUROC of AUDIT-QF, AUDIT-C, and STAD for at-risk drinking.
Comparison of AUROCs between STAD and abbreviated version of the AUDIT.
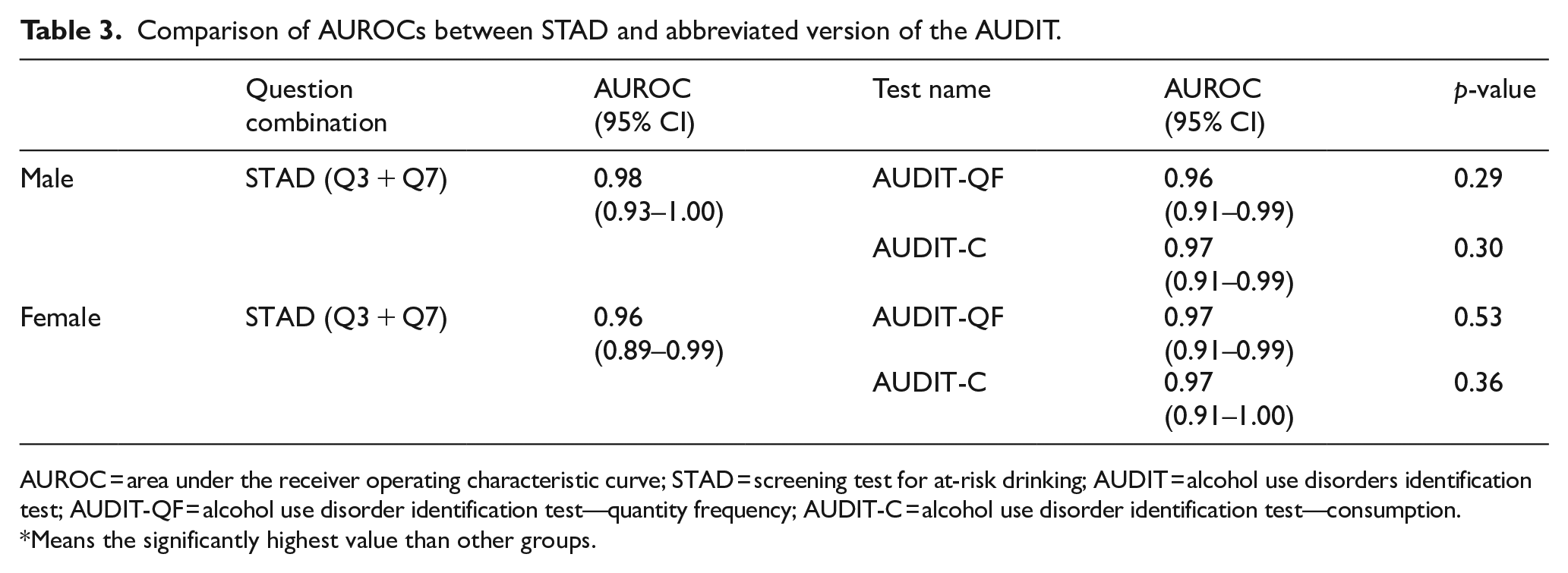
AUROC = area under the receiver operating characteristic curve; STAD = screening test for at-risk drinking; AUDIT = alcohol use disorders identification test; AUDIT-QF = alcohol use disorder identification test—quantity frequency; AUDIT-C = alcohol use disorder identification test—consumption.
Means the significantly highest value than other groups.
Discussion
Screening and brief intervention for at-risk drinking among young and middle-aged adults is important. The National Institute on Alcohol Abuse and Alcoholism (NIAAA) proposed several clinical situations—ED or urgent care centers—as key opportunities for screening at-risk drinking. 22 Many studies have shown that a brief intervention about alcohol drinking in the ED is effective.11,23–25 The ED is an important clinical place for screening at-risk drinking and conducting a brief intervention.
Research was conducted to develop and test abbreviated versions of AUDIT as simple screening instruments that can be administered quickly.6–9,4,10,26,27 Among them, in the case of AUDIT-Q3 alone, AUDIT-QF (first and second questions), and AUDIT-C (first, second, and third questions), items were selected based on past research,27,28 whereas AUDIT-4 (first, second, third, and tenth questions) and AUDIT-PC (primary clinic, first, second, fourth, fifth, and tenth questions) extracted the items using logistic regression.9,29 Fast alcohol screening test (FAST, third question for first step, fifth, eighth, and tenth questions for second step) used a method to compare the sensitivity and specificity of the combinations of the questions after the questions were analyzed by principal component analysis. 30 However, previous abbreviated tests are limited in that they do not properly reflect the AUDIT survey structure. AUDIT-C, the most widely used abbreviated version of AUDIT, 2 is limited to three questions about the consumption of alcohol and does not reflect the structure of the AUDIT ten questions. For this reason, Choi et al. developed the two-question abbreviated version of AUDIT, STAD, which could replace AUDIT-C in 2018. STAD consisted of two questions by selecting one question from each of the two factors of AUDIT. For the first factor, Q3 was selected, which had the highest factor loading, based on the results of the factor analysis and previous research. For the second factor, Q7 and Q8, which had the highest factor loadings, were selected first. Subsequently, the combinations of Q3, Q7 and Q3, Q8 were compared in terms of AUROC, sensitivity, and specificity. Based on the results of the comparison, Q3 and Q7 were selected for the new abbreviated test, STAD. 17 This is an account of the development process of AUDIT.
When developing STAD, data from KNHANES, the representative health indicator of South Korea, were used. There is a limitation that STAD has not been validated in the clinical setting. In this study, we conducted STAD on patients visiting the ED. The cut-off values of STAD in this study were 3 for males and 2 for females. These cut-off values are the same as previous study. 17 The cut-off values in men and women differ because of the different patterns of drinking behavior and alcohol-related problems according to gender and age. In the case of AUDIT, the cut-off value for at-risk drinking applies differently in men, women, and the elderly (8 points for men and 7 points for women and the elderly). 2
In this study, sensitivity/specificity of STAD was 98.0/93.5 and 96.4/79.6 for men and women, respectively. AUROC of STAD was 0.98 and 0.96 in men and women, respectively. STAD has similar AUROC, despite having one less question, compared with AUDIT-C, which is the most widely used abbreviated version of the AUDIT. In the previous study, STAD was validated by data from KNHANES, the sensitivity/specificity were 86.7/96.3 and 97.1/88.5 for males and females, respectively. AUROC was significantly higher for STAD than for AUDIT-QF, which has the same number of questions. There was no significant difference between AUDIT-C, consisting of three questions, and STAD. 17 The results of this study confirmed that STAD is a useful screening test for clinical use.
One of the limitations of this study is that the population was not representative of the patients that attended the ED during the study period. This was due to the exclusion of severely unwell patients as they could not be surveyed. Small response rate (2.7%) is weak point of this study. In addition, one sample site from one ED means that the results may not be generalizable to other population in other areas. Due to the nature of the ED, where limited medical personnel are required to treat a large number of patients, it was difficult to conduct a survey without dedicated personnel. The difficulty of conducting screening and brief interventions in a busy ED with limited medical personnel may also be a limitation of screening for at-risk drinking in this environment. A more representative sample may be achieved if more personnel were available to conduct the study with a larger number of patients in a number of sites.
The purpose of the present study was to validate STAD, a new abbreviated test that reflects AUDIT’s structure, in clinical situations. The findings show that STAD is a useful test that reflects the structure of AUDIT and can detect at-risk drinking. It is expected that this test facilitate screening for at-risk drinking more easily. Further research will be needed to see if STAD reduces the time for screening at-risk drinking and increases the frequency of appropriate brief alcohol interventions.
Supplemental Material
revision_appendix_1 – Supplemental material for Clinical validation of screening test for at-risk drinking for young and middle-aged adults in an emergency department
Supplemental material, revision_appendix_1 for Clinical validation of screening test for at-risk drinking for young and middle-aged adults in an emergency department by Hosub Chung and Jae Hee Lee in Hong Kong Journal of Emergency Medicine
Footnotes
Acknowledgements
The authors would like to acknowledge their ED staff for their support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical approval
This study was approved by the Institutional Review Board of Ewha Womans University Mokdong Hospital. (IRB No. 2018-07-080-001)
Informed consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.