
Abstract
A 77-year-old woman on metoprolol and lisinopril presented to an emergency department with giddiness after vomiting for few hours. She was found to have low blood pressure and bradycardia 38 beats per minute due to atrioventricular nodal blockade. Her bradycardia was refractory to atropine and dopamine infusion; but improved with calcium gluconate. She was found to have acute kidney injury and hyperkalemia at 6.4 mEq/L. This is a case of Bradycardia, Renal Failure, Atrioventricular-Nodal Blockers, Shock, and Hyperkalemia (BRASH) syndrome, precipitated by dehydration and perpetuated by atrioventricular blockade, illustrating the degree of bradycardia and electrocardiographic changes being out of proportion to the potassium level. BRASH syndrome should be recognized and intervened early in the course to avoid the patient entering a vicious cycle that could be rapidly fatal.
Case presentation
A 77-year-old woman presented to a local emergency department with giddiness. Her past medical history included atrial fibrillation on metoprolol for rate control, hypertension on lisinopril, and impaired fasting glucose not on medication. She had poor oral intake for several days and subsequently developed vomiting plus retrosternal chest discomfort for several hours, thus called the ambulance. She reported good compliance to her prescribed medications.
Her first blood pressure at triage was 76/30 mmHg and heart rate 38 beats per minute (bpm). She appeared tired but remained conscious and orientated. Fluid resuscitation was started immediately, and an electrocardiogram (ECG) was done (Figure 1).
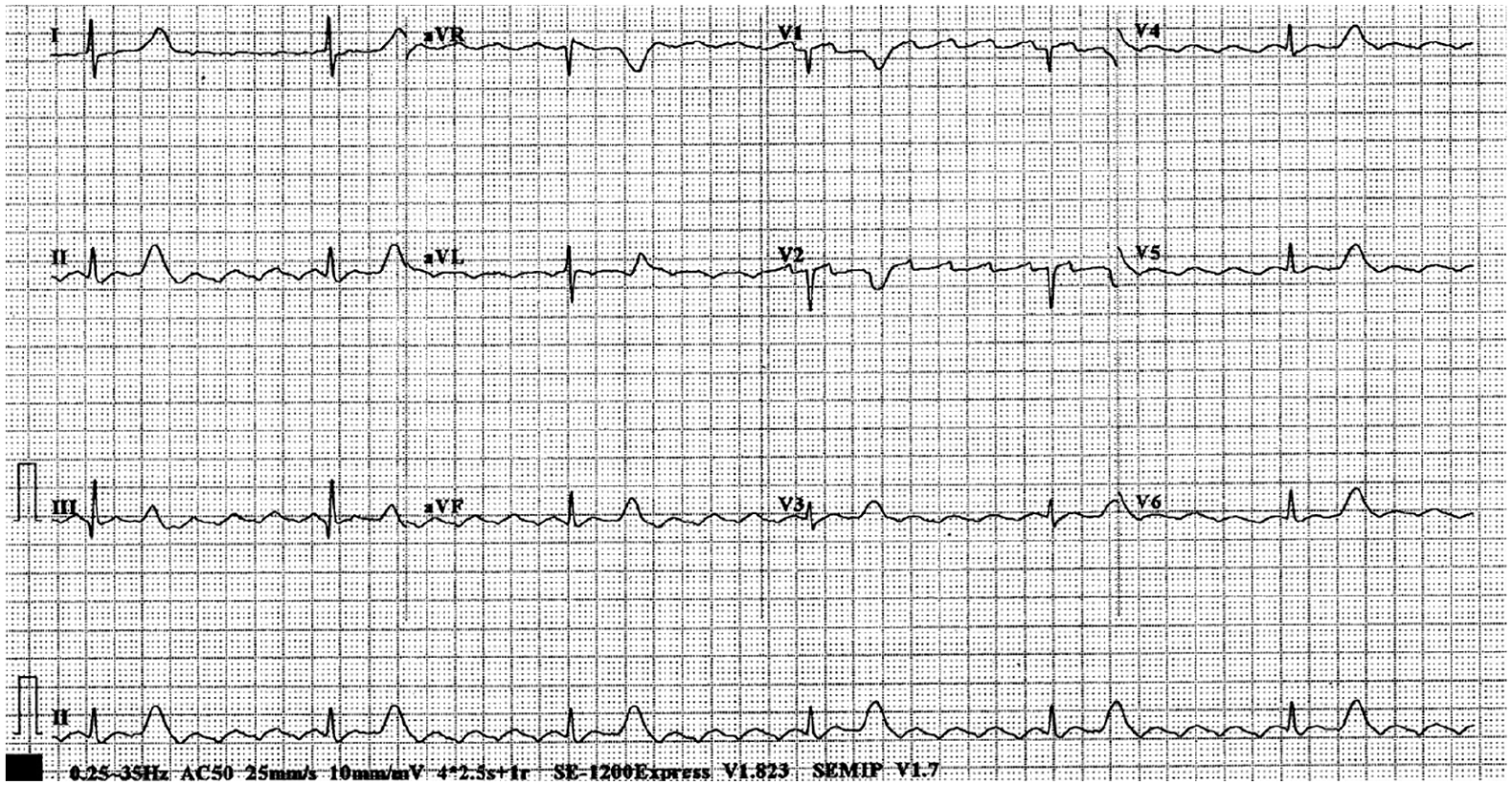
The patient’s first ECG.
Question 1
How do you interpret this ECG?
Answer 1
Atrial flutter waves could be seen, with a regular 6:1 conduction leading to bradycardia of approximately 36 bpm. The T waves were prominent, with an amplitude comparable or larger than that of the QRS complex in some leads. This is highly suggestive of hyperkalemia. 1
The emergency physician (EP) first attempted to treat the bradycardia with atropine and followed by dopamine infusion in a moderately high dose, but both medications failed to increase the heart rate. Subsequently, in view of the high suspicion of hyperkalemia and the patient being in shock from high degree heart block, a dose of calcium gluconate was administered, which within minutes improved the patient’s hemodynamics with the prominent T waves resolved (Figure 2) and dopamine weaned off. The blood tests coming back later showed acute kidney injury (AKI) with creatinine level at around 300 µmol/L (baseline level was normal) and potassium level at 6.4 milliequivalents per liter (mEq/L). The patient was admitted to the cardiac care unit (CCU) for close monitoring, in which her vital signs remained stable. Her AKI resolved with rehydration, chest discomfort subsided, and her troponin levels did not ascend.
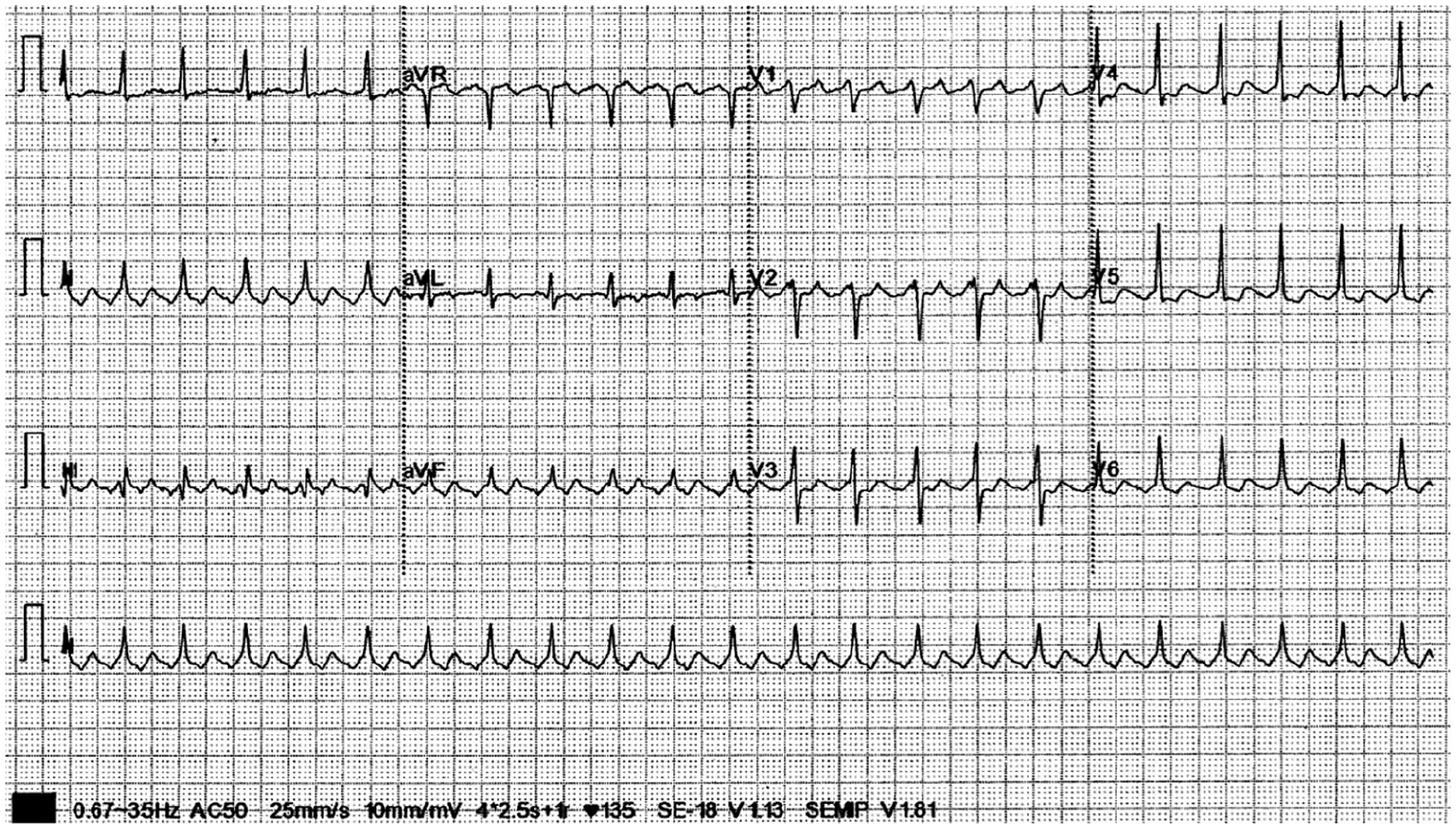
ECG after administration of calcium gluconate. Note that the prominent T waves in Figure 1 had resolved.
Question 2
What were the predisposing and precipitating factors for the patient to present with this arrhythmia?
Answer 2
The predisposing factors included being on beta blocker and angiotensin-converting enzyme inhibitor. The AKI was most likely precipitated by dehydration from vomiting.
Discussion
This is a typical presentation of Bradycardia, Renal Failure,
Footnotes
Author contribution
All authors contributed equally to this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable for this clinical quiz.
Informed consent
Written informed consent was obtained from the patient for his/her anonymized information to be published in this article.
Human rights
The data and images obtained were in accordance with the principles outlined in the Declaration of Helsinki.