
Abstract
Objectives:
In some trauma centres, anaesthesiologists have the primary responsibility of managing airway in trauma resuscitation. However, as emergency physicians establish a separate specialty with airway management and endotracheal intubation being one of the core skills, role delineation within trauma members may vary. In this cohort study, we aim to determine the difference in mortality of trauma patients requiring intubation in the emergency department between emergency physicians and anaesthesiologists.
Methods:
We screened all 1588 patients in the hospital trauma registry from 2015 to 2018. We included all patients requiring endotracheal intubation and aged 18 or above but excluded those with pregnancy, presented with cardiac arrest and secondarily transferred from other hospitals. A total of 349 eligible patients were sorted into two cohorts according to the physicians who performed intubations (anaesthesiologists = 205 patients, emergency physicians = 144 patients). Patients’ baseline demographics, 30-day all-cause mortality and other predefined secondary outcomes were compared by statistical tests. Stepwise logistic regression of 30-day all-cause mortality was performed.
Results:
Our study has shown that intubation by emergency physicians was not associated with higher 30-day all-cause mortality after potential confounders were controlled by logistic regression (adjusted odds ratio = 1.253, p = 0.607). Both groups also did not differ in other clinical important secondary outcomes, including proportion of successful intubations, use of surgical airway or rescue manoeuvres, respiratory and airway complications, mortality in intensive care or high-dependency unit, post-intubation cardiac arrest, post-intubation hypotension and post-intubation hypoxia.
Conclusion:
Endotracheal intubation by emergency physicians is not associated with increased 30-day all-cause mortality when compared to anaesthesiologists after accounting for confounders.
Introduction
Background
Polytrauma is a life-threatening condition requiring multidisciplinary care. Many trauma centres adopt a ‘Trauma Resuscitation Team’ (TRT) approach. The exact composition of the TRT varies from centre to centre. There are differences in practice with respect to whom should manage the airway in trauma patients.
Traditionally, anaesthesiologists (ANs) have the primary responsibility for airway management in most centres. 1 However, with emergency medicine being established as a distinct specialty and airway management being one of the core skills,2 –5 emergency physicians (EPs) routinely perform advanced airway management in the emergency department (ED).5 –8
Previous observational studies have not demonstrated any differences in the outcome of trauma patients with airway managed by EPs versus ANs.9 –11 Locally, we do not have any study comparing outcome of intubation by EPs versus ANs in trauma resuscitation.
Airway management in trauma resuscitation is always challenging. The risk of rapid airway compromise is a common and important reason for early intubation in patients with direct airway trauma. EPs have the privilege of being the first to attend the patient and opportunity to timely manage the airway at risk.
Objectives
Our primary objective is to determine the difference in mortality of trauma patients requiring intubation between EPs and ANs. We also aim to identify the difference in other important outcome differences and also potential contributory factors of mortality. Secondary outcome and complications that may explain the mortality difference are identified. Potential contributory factors to mortality are also studied.
Methods
Study design
This is a registry-based unmatched cohort study. We identified trauma patients requiring intubation during resuscitation in the ED, and then extracted relevant trauma-related parameters and outcome data from the trauma registry of the hospital and patients’ health records. The reporting of this study is in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement. 12
Setting
This study was conducted in a trauma centre in Hong Kong. The centre is one of the five trauma centres in the region and it is also a regional tertiary and quaternary referral centre with full complements of clinical services. Daily ED attendance of the centre is around 500 patients. As a designated trauma centre, our unit receives primary trauma diversions from ambulance service and also secondary trauma diversion from other regional hospitals. Yearly major trauma (injury severity score (ISS) >15) attendance is around 300.
In this hospital, TRT comprises specialist EPs and trauma surgeons. ANs and other subspecialties will be consulted according to the injury pattern. The decision to solicit help from ANs for airway management is at the discretion of the attending EP specialist.
Participants
The hospital trauma registry captures any patients who met TRT activation criteria (see Appendix 1), who were triaged as critical or emergency in the ED, who died (excluding death prior to arrival to ED) and were admitted to intensive care units (ICUs)/high dependency units (HDUs). 13 Injury and outcome data were prospectively collected and entered into the registry.
We screened all patients requiring endotracheal intubation in the ED from the trauma registry of the centre during the period of 1 January 2015 to 31 December 2018. Patients were included if age 18 or above. Pregnant patients, those presented with cardiac arrest and those transferred from other hospitals were excluded.
Patients recruited were sorted into two cohorts according to the specialty (EPs or ANs) providing trauma airway management.
Variables
Our primary outcome is 30-day all-cause mortality.
Secondary outcomes include (1) proportion of successful intubations, (2) need of surgical airway or rescue manoeuvres, (3) respiratory or airway complications, (4) ICU and HDU mortality, (5) post-intubation cardiac arrest, (6) post-intubation hypotension and (7) post-intubation hypoxia.
Rescue manoeuvres were defined as any use of laryngeal mask airway or bronchoscopic intubation instead of direct laryngoscopy or video laryngoscopy. Airway and respiratory complications are composite outcomes defined as any ventilator-associated pneumonia (VAP)/hospital-acquired pneumonia (HAP) or tracheotomy for prolonged intubation. HDU/ICU mortality is defined as mortality during ICU/HDU care. Post-intubation cardiac arrest was defined as any cardiac arrest during resuscitation in the ED after the injection of induction and/or paralytic agents whichever was earlier. Post-intubation hypotension was defined as the first systolic blood pressure (SBP) after the placement of endotracheal tube less than 90 mmHg before leaving ED. Post-intubation hypoxia was defined as the lowest pulse oxygen saturation (SpO2) after the placement of endotracheal tube less than 93% before leaving ED.
Patients’ demographic data, including age, gender and comorbidities, were also collected. Comorbidites included AIDS, cirrhosis, diabetic mellitus, hepatic failure, immunosuppression, leukaemia/myeloma, non-Hodgkin’s lymphoma, solid tumour with metastasis, chronic respiratory condition. The definition of these conditions follows the definition used in APACHE IV score 14 . Renal failure was defined as patient requiring renal replacement therapy (peritoneal dialysis or hemodialysis). Data on patients requiring long-term residential care (elderly home, etc) were also collected. Clinical variables collected included vital signs (blood pressure, oxygen saturation and Glasgow Coma Scale), duration of ED resuscitation, time to intubation, base excess, emergency operations (including three-in-one procedure for pelvic fracture, laparotomy, neurosurgery, closed or open reduction with fixation, or others), activation of massive transfusion protocol, presence of neck collar, trauma diversion status and TRT activation status. Duration of ED resuscitation is the duration between patient transferred in and out of the resuscitation room. Time to intubation is the time from ED registration to injection of paralytic agent. If no paralytic agent was used, the time of recording first vital signs documented after intubation was used.
Mechanism of trauma was grouped into three categories, namely, burns, low-energy trauma (such as fell from height less than 2 m, or penetrating injuries), and high-energy trauma (such as fell from height more than 2 m or motor vehicle accidents). Trauma-related scores (probability of survival (1998), ISS, Revised Trauma Score (RTS)) were also extracted for analysis.
We were particularly interested in chest, head, neck and facial trauma which may predict intubation difficulty. As such, we have extracted the Maximum Abbreviated Injury Scale (MAIS) from the registry, by analysing the body region code of 1, 2, 3, 4 and 6 (head, face, neck, chest and spine) of the Abbreviated Injury Scale (AIS) separately. Spinal injuries other than cervical spine were excluded.
Data sources and measurements
Clinical and laboratory data were retrieved from the trauma registry and the Clinical Management System (CMS) via the Clinical Data Analysis and Reporting System (CDARS) of the Hospital Authority. Patient’s case notes were also accessed to retrieve data and ascertain diagnosis. The trauma registry was also the source of trauma-related data, such as clinical parameters during ED resuscitation, mechanism of injuries and ISSs, namely, AIS, ISS and RTS. The outcomes (mortality/survival) and interventions given during pre-hospital, ED resuscitation and inpatient period were also retrieved.
The diagnosis of VAP and HAP was based on the diagnosis made by the treating physicians.
The coding of the ISS and AIS was performed by an experienced trauma nurse specialist trained in the AIS coding.
Bias
In addition to the inherent bias in a retrospective study, we noted that EPs were found to intubate more patients with isolated head injury. It is well known that the probability of survival of severely head injured patients is poorer when compared with that of patients with other system injuries having the same ISS. There are also many parameters showing baseline imbalance. Hence, a planned logistic regression was performed to control for confounding factors resulted from differences in trauma severity and pattern.
Study size
Based on a cursory review of trauma registry data of the year 2017, there were a total of 107 intubated patients. Mortality among these patients was 53.5% and 29.7% when the airway was managed by EPs versus ANs, respectively.
Based on the above observation, the required sample size was found to be around 195, according to the Fleiss equation with continuity correction, taking power (1-beta) of 90% and alpha of p < 0.05. 15 To achieve the expected sample size, we have screened the trauma registry data from 2015 to 2018.
Quantitative variables
In this study, the following grouping of quantitative variables was performed prior to analysis.
MAIS more than 2 in each of the body regions was considered as serious. This is based on the definition of the abbreviated injury score.
Patient with ISS > 15 is considered as suffering from major trauma, as customary in trauma researches.
Statistical methods
Data were analysed by IBM SPSS Statistics Version 25, Microsoft Excel version 16.23 and Apple Inc. Numbers were used to handle calculation and data analysis.
Patient demographics were reported with descriptive statistics, using mean, median, standard deviation (SD) and interquartile range (IQR). Normality of continuous variables was tested with Shapiro-Wilk test. Difference between normal variables was analysed with Student’s t tests while non-normal variables were managed with Mann–Whitney’s sign rank tests. Categorical outcome variables such as 30-day all-cause mortality were analysed with the chi-square tests or Fisher–Freeman–Halton exact tests.
Missing data would be managed with multiple imputations, using missing at random assumption. The multiple imputation function of SPSS was used to impute10 sets of complete data set by the Markov Chain Monte Carlo method. The maximum number of parameters in imputation model was set to 10. Each data set was then inspected by two authors for consistence. Then, the pooled averaged values from the 10 sets will be used for analysis.
We carried out a multivariable logistic regression to control for any potential confounding and interaction. Baseline characteristics with potential difference (p < 0.25) were included in the univariate regression analysis (Table 3). Statistical outcomes are to be regarded as significant if p is < 0.05, and adjusted odds ratios (ORs) would be reported.
Analysing the missing data by listwise deletion was planned as a sensitivity analysis.
Results
Participants
We screened all patients (1588 patients) in the trauma registry of the centre from 2015 to 2018. A total of 365 (23.0% of 1588 patients) patients age 18 or above were found to require intubation in the ED. Among them, sixteen patients were excluded, including fourteen patients presented with cardiac arrest and two patients transferred from other hospitals (see Figure 1).
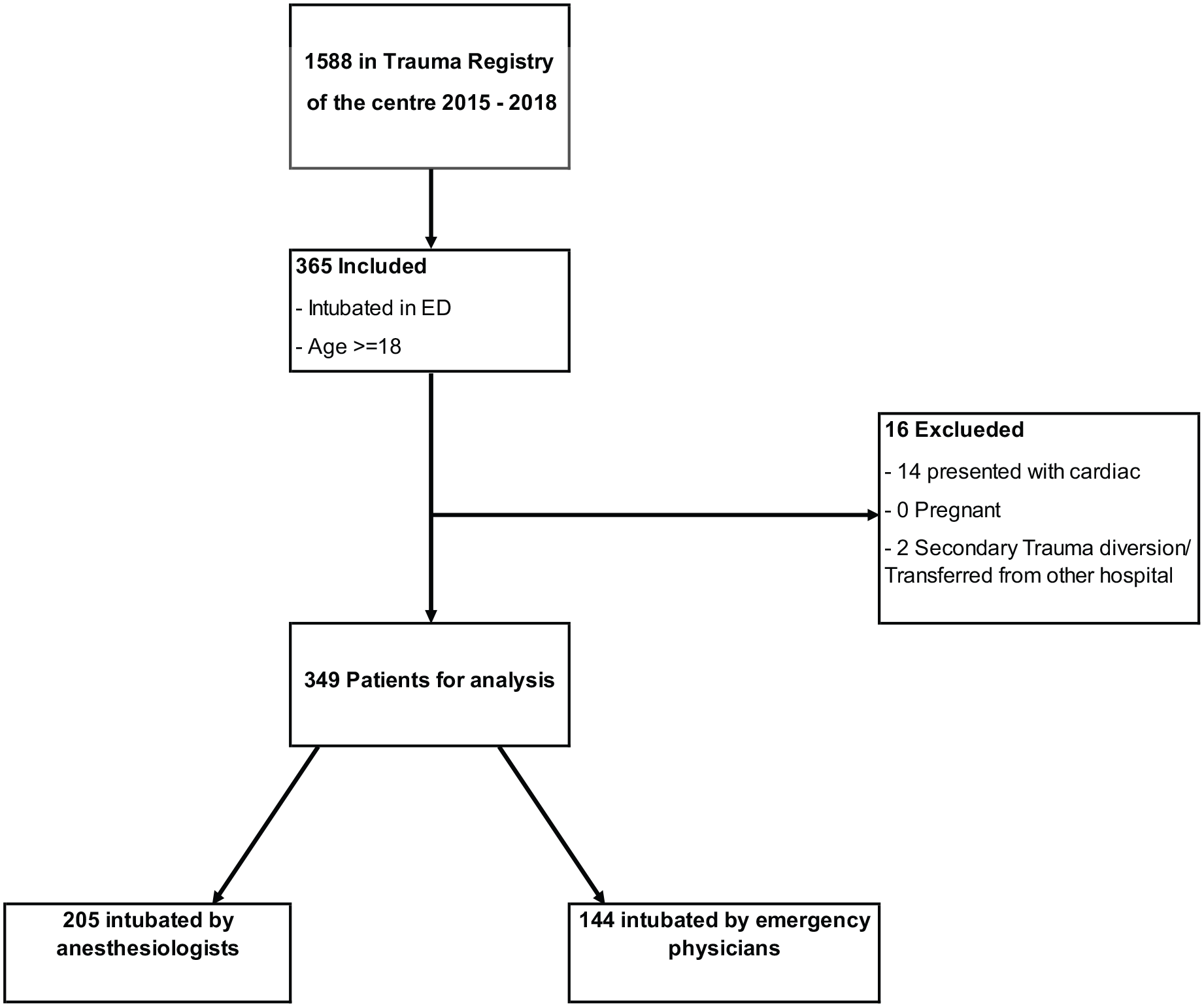
Flowchart: Case eligibility and selection.
A total of 349 patients were included in the final analysis; 205 patients (58.7%) were intubated by ANs while 144 patients (41.3%) were intubated by EPs.
Descriptive data
The two cohorts differ in many aspects in baseline characteristics (Table 1).
Patient characteristics and injury pattern.
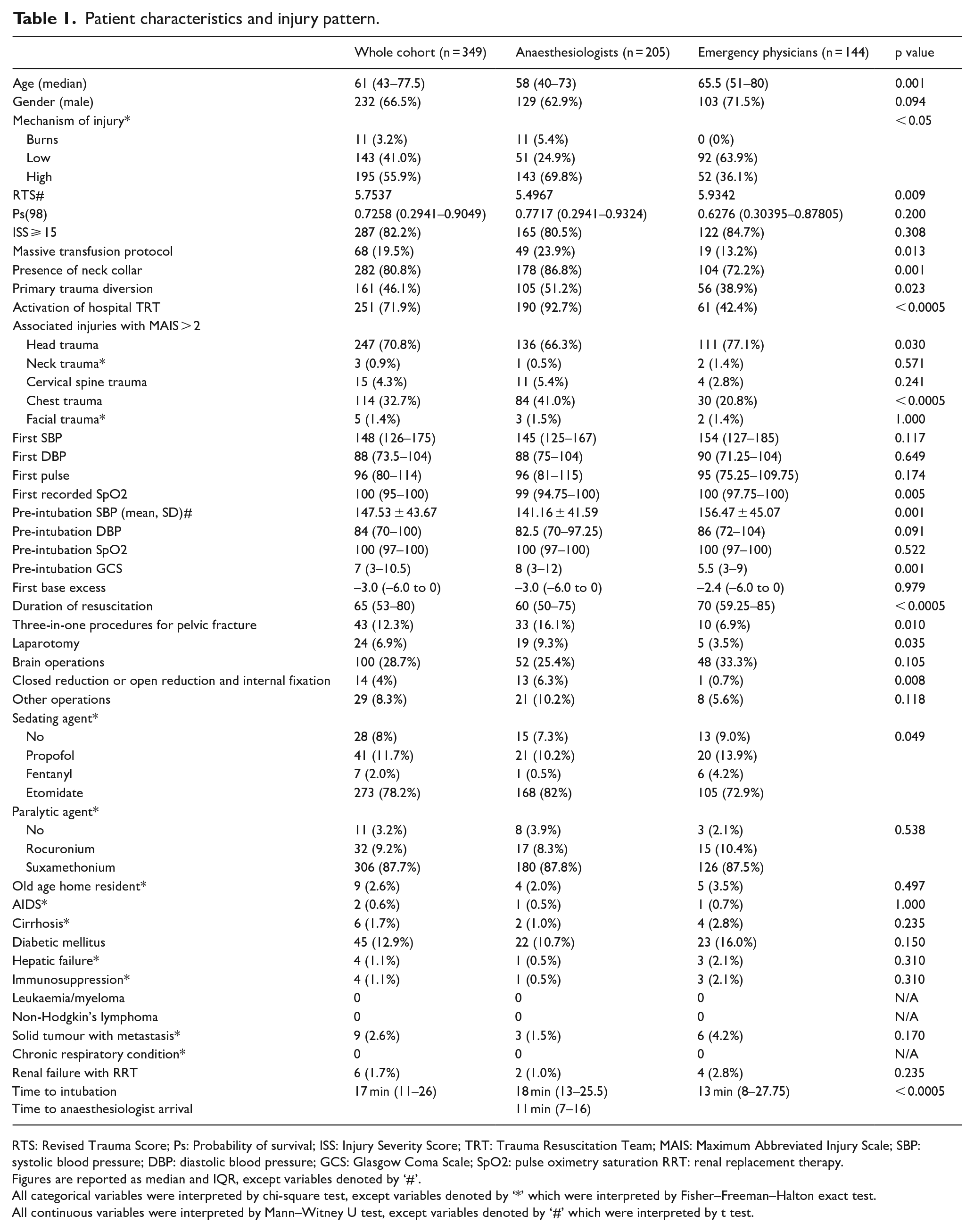
RTS: Revised Trauma Score; Ps: Probability of survival; ISS: Injury Severity Score; TRT: Trauma Resuscitation Team; MAIS: Maximum Abbreviated Injury Scale; SBP: systolic blood pressure; DBP: diastolic blood pressure; GCS: Glasgow Coma Scale; SpO2: pulse oximetry saturation RRT: renal replacement therapy.
Figures are reported as median and IQR, except variables denoted by ‘#’.
All categorical variables were interpreted by chi-square test, except variables denoted by ‘*’ which were interpreted by Fisher–Freeman–Halton exact test.
All continuous variables were interpreted by Mann–Witney U test, except variables denoted by ‘#’ which were interpreted by t test.
The EP group included older patients compared with AN group (median age = 65.5 vs 58, p = 0.001). ANs intubated all burn patients (n = 11) in the whole cohort.
ANs intubated more patients with serious chest trauma (41.0% vs 20.8%, p < 0.0005) and the presence of a neck collar (86.1% vs 72.2%, p = 0.001). Both groups did not differ in severity of neck trauma, cervical spine trauma and facial trauma.
AN group had higher proportion of activation of massive transfusion protocol (23.9% vs 13.2%, p = 0.013), primary trauma diversion (51.2% vs 38.9%, p = 0.023) and activation of the hospital TRT (92.7% vs 42.4%, p < 0.0005). More patients in AN group received three-in-one procedures for pelvic fracture (16.1% vs 6.9%, p = 0.010), laparotomy (9.3% vs 3.5%, p = 0.035), closed reduction or open reduction and internal fixations (6.3% vs 0.7%, p = 0.008).
While EP intubated more patients with serious head injury (77.1%vs 66.3%, p = 0.030), the median Glasgow Coma Scale in the AN group is also significantly better than the EP group (8 vs 5.5, IQR = 3–12 vs 3–9, p = 0.001). However, both group did not differ significantly in receiving brain operations (25.4% vs 33.3% p = 0.105) and other operations (10.2% vs 5.6%, p = 0.118).
ANs intubated patients with lower pre-intubation SBP (mean = 141.16 vs 156.47, p = 0.001) and lower first recorded SpO2 (median = 99% vs 100%, IQR = 94.75–100 vs 97.75–100, p = 0.005) but received shorter duration of resuscitation in the ED (median = 60 vs 70 min, IQR = 50–75 vs 59.25–85, p < 0.0005). Other clinical parameters such as first SBP and diastolic blood pressure (DBP), first pulse, pre-intubation DBP and laboratory parameter such as base excess did not differ in both cohorts.
Overall, the EPs handled more severely head injured and older patients, while the ANs handled patients who are likely to be in shock and bleeding.
The following baseline variables have missing data: first recorded SpO2 1.43%, pre-intubation SBP and DBP 0.86%, pre-intubation SpO2 3.43%, first base excess 6.3%.
Outcome data
Among the 349 trauma patients requiring intubation in ED during the study period, 67 (32.7%) in AN group died within 30 days of hospitalisation while 69 patients (47.9%) died in EP group (Table 2).
Primary and secondary outcomes.
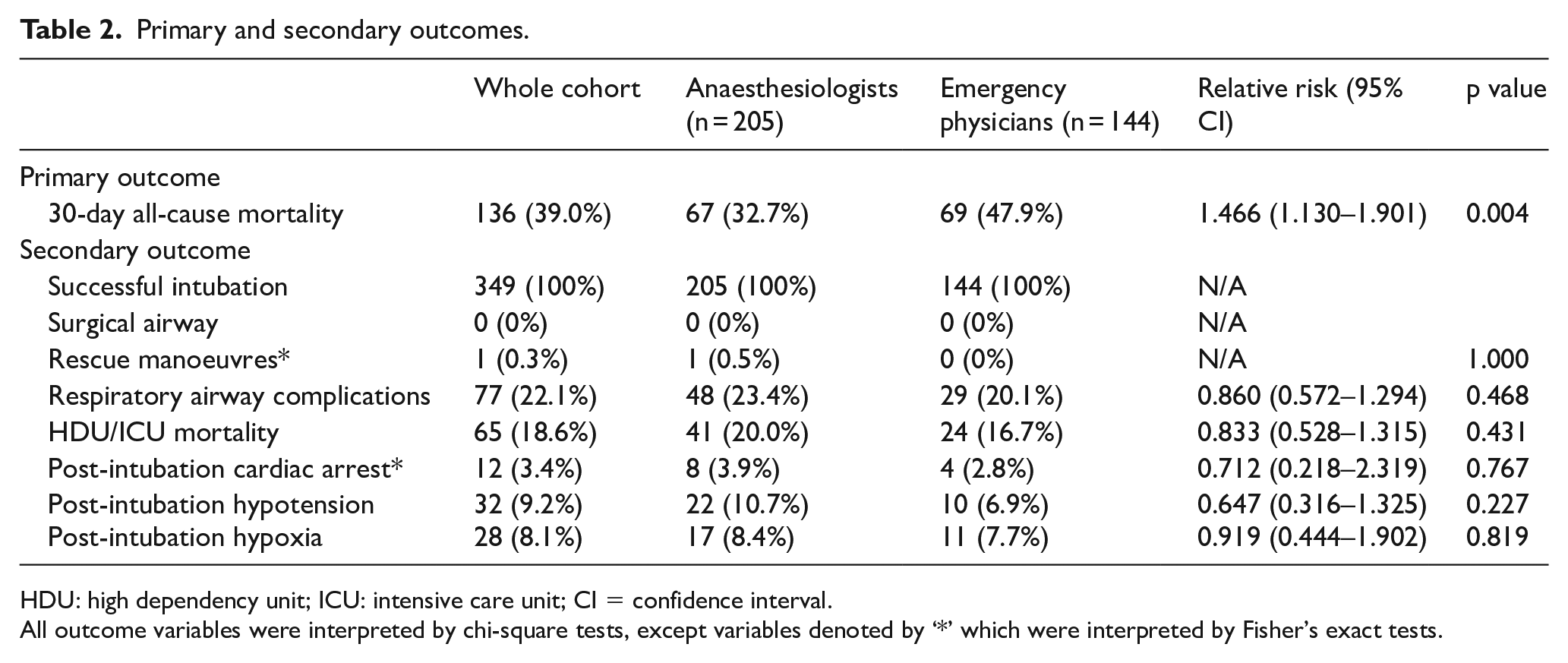
HDU: high dependency unit; ICU: intensive care unit; CI = confidence interval.
All outcome variables were interpreted by chi-square tests, except variables denoted by ‘*’ which were interpreted by Fisher’s exact tests.
As for the secondary outcomes, the number of successful intubations of AN and EP group was 100%, need of surgical airway was 0% and need of rescue manoeuvres was 0.5% vs 0%.
In all, 23.4% of AN group patients developed respiratory and airway complications while 20.1% of EP group patients did. Mortality in ICU or HDU was 20.0% in AN group and 16.7% in EP group. In all, 3.9%, 10.7% and 8.4% of AN group patients versus 2.8%, 6.9% and 7.7% of EP group patients developed post-intubation cardiac arrest, post-intubation hypotension and post-intubation hypoxia, respectively. Both groups did not differ significantly in secondary outcomes (Table 2).
The following outcome variable has some data missing: post-intubation hypoxia 0.86%.
Main results
Primary outcomes
Intubation by EPs was associated with higher unadjusted 30-day all-cause mortality (relative risk = 1.466, 95% confidence interval (CI) = 1.130–1.901, p = 0.004) (Table 2).
Controlling of potential confounding factors
Logistic regression was performed to adjust for baseline imbalance and potential confounding factors for our primary outcome, 30-day all-cause mortality. Univariate analysis had showed 27 potential confounding factors with p < 0.25 (Table 3).
Univariate and multivariate regression of primary outcome: 30-day all-cause mortality.
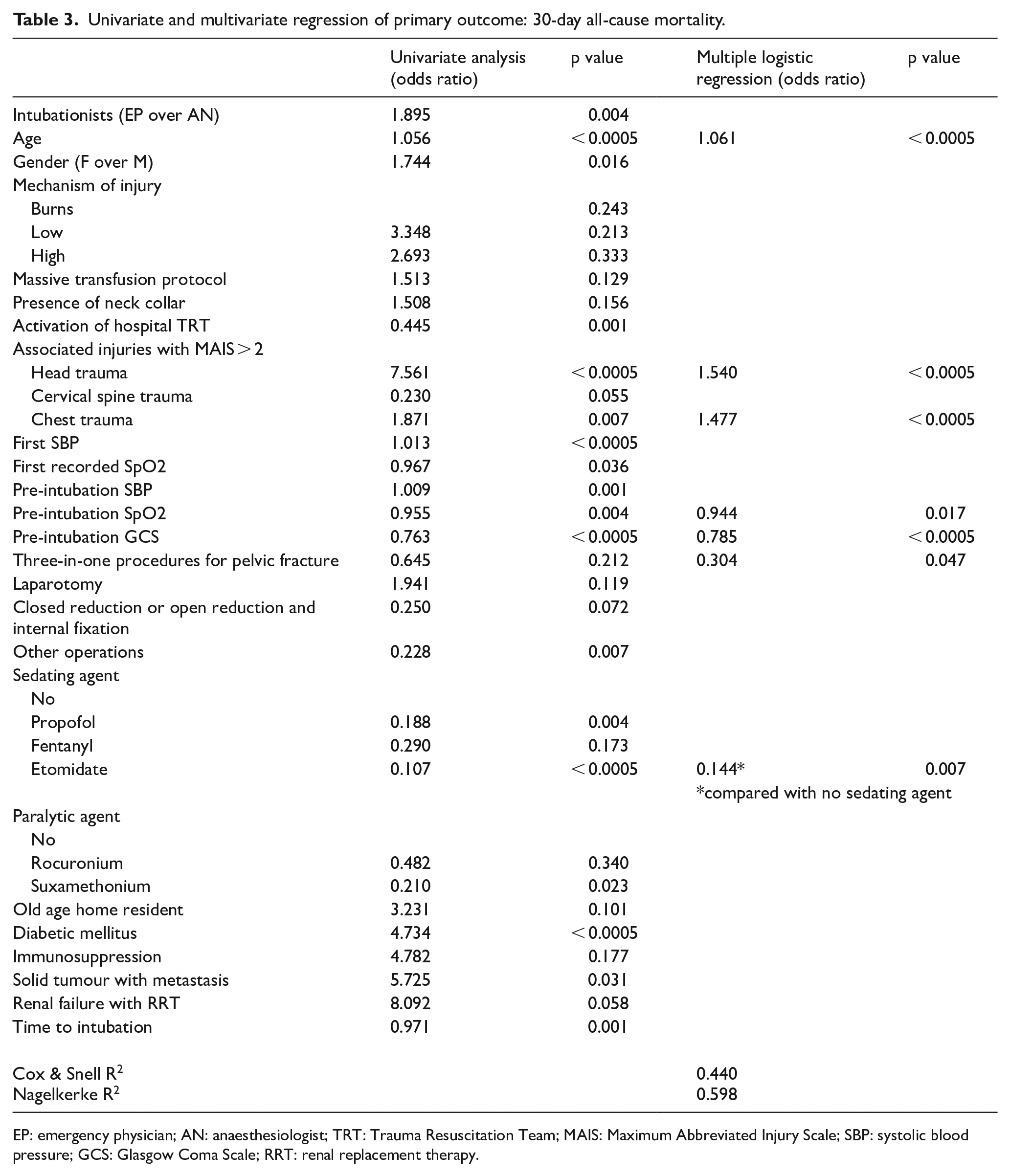
EP: emergency physician; AN: anaesthesiologist; TRT: Trauma Resuscitation Team; MAIS: Maximum Abbreviated Injury Scale; SBP: systolic blood pressure; GCS: Glasgow Coma Scale; RRT: renal replacement therapy.
After accounting for these potential confounders, intubation by EPs is not found to be associated with increased 30 days mortality (adjusted OR = 1.253, p = 0.607).
Other analyses
Sensitivity analysis
We performed a sensitivity analysis of the missing data by assuming missing completely at random. Missing data were then deleted listwise. A total of 316 cases remained for re-analysis.
This does not differ from the main result significantly in both the primary and secondary outcomes.
Logistic regression analysis
A stepwise logistic regression analysis was done on the cohort to identify independent predictors of outcome (Table 3).
Discussion
Key results
This retrospective cohort study demonstrated that higher 30-day all-cause mortality occurred in the group of patients who were intubated by EPs. However, the mortality difference is not substantiated by those secondary outcomes and complications. Both groups had 100% rate of successful intubation. Respiratory and airway complications such as VAP and HAP did not have any statistical significant difference. The immediate post-intubation complications such as cardiac arrest, hypotension and hypoxia did not differ in both groups.
The more probable explanations for the primary outcome difference of the two groups are the baseline imbalance leading to those confounding factors. Twenty-seven potential confounding factors (p < 0.25) are detected (Table 3). As a matter of fact, those baseline parameters do lead to logical explanation for the observed primary outcome difference. EP group patients were older (65.5 vs 58 years old), suffered from more (77.1% vs 66.3%) and more severe (pre-intubation GCS = 5.5 vs 8) head injury and poorer initial physiological status (RTS = 5.9342 vs 5.4967). All of these parameters are statistically significant.
On the contrary, the lower pre-intubation SBP (141.16 vs 156.47 mmHg) and first recorded SpO2 (99% vs 100%) in the AN group are clinically not significant despite significant statistically. There were more bleeding patients in the AN group. Chest trauma (41% vs 20.8%), use of massive transfusion protocol (23.9% vs 13.2%), three-in-one procedures for pelvic fracture (16.1% vs 6.9%) and laparotomy rate (9.3% vs 3.5%) are significantly more than the EP group. Given a relatively high percentages of patients with ISS ⩾ 15 in both groups (80.5% vs 84.7%), the EP group with more and severe head injury patients explains the higher 30-day all-cause mortality. 16
Limitations
The current study is a single-centre retrospective cohort study. Clinical practice varies from different trauma centres, caseloads, service scale and staff expertise. The availability of onsite ANs is also variable among some EDs.
The decision of who perform intubation is one of the limitations of our study. The attending EP may have intubated patients on their own or consulted ANs to intubate, and the decision is on case-by-case basis.
Grade of laryngeal view and use of direct and video laryngoscopy are not well documented. Hence, difficulty of intubation could not be compared. First pass success data are missing in most of the ED records, and the experience of intubationists (and their supervisors if any) could not be tracked in our study. Therefore, we could not use first pass success as one of our outcomes.
When determining the independent predictors for mortality, the sample size may not be sufficient as we calculated our sample size based on crude primary outcome which is 30-day all-cause mortality.
As for the outcome measures, we did not measure the functional outcome, or examine the quality of life, both of which are important outcomes for survivors of severe trauma.
Interpretation
In this retrospective cohort study, it cannot demonstrate any difference in 30-day all-cause mortality for patients indicated for intubation as performed by EPs or ANs. All the secondary outcomes and immediate post-intubation complications are comparable. Suffice to say, in circumstances when emergency intubation for trauma patients is required and AN is not immediately available, EP can intubate the patients safely.
Generalisability
Our study result is applicable to all urban EDs with a well-established, EP-lead trauma service.
Footnotes
Appendix 1
Acknowledgements
We would like to acknowledge the Trauma Service of Queen Elizabeth Hospital for contributing in the preparation and data collection process.
Author contributions
Conceptualization: THT, MY and OYC. Methodology: THT, MY and LC. Investigation: THT, OYC and LC. Data Curation: THT, OYC, LC and MY. Visualisation: THT and MY. Formal analysis: THT and MY. Writing – original draft: THT and MY. Writing – review and editing: THT, MY, OYC and HFH. Supervision: MY and HFH.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Availability of data
Data will be made available on request. 17
Ethical approval
Ethical approval was sought from Research Ethics Committee, Kowloon Central Cluster, Hospital Authority of Hong Kong (KC/KE-18-0232/ER-3).
Informed consent
Informed consent was waived as this is a retrospective cohort study.
Human rights
Human rights are respected. The study is a retrospective study, and no information identifiable to individuals has been collected or stored.