
Abstract
Background:
In a busy local emergency department, patients with certain non-life-threatening conditions which only require relatively quick and straightforward management may encounter long waiting times. A new service model called the “Fast Track” Nursing Service attempts to lessen the service load of the regular service queues and to improve patient outcomes.
Objectives:
This article reports the service outcomes of the Fast Track Nursing Service.
Methods:
Nurses at our department are selected and trained under clinical protocols specially developed for this service. Assessments and quality assurance audits ensure the quality of service.
Results:
This service resulted in comparatively shorter waiting times for patients included in predetermined clinical protocols. There was also a high level of patient satisfaction with this service.
Conclusion:
Our Fast Track Enhanced Nursing service is a model of tailored service diversification to shorten waiting times, thus improving patient satisfaction and outcome.
Introduction
Situated in a dense urban area with a population as diverse as ranging from active young families to elderly patients in old aged homes, our emergency department faces a wide variety of cases every day. Among the more complex and urgent cases, including myocardial infarction, respiratory failure, stroke, and trauma, some other cases, such as fish bone ingestion, acute retention of urine, Ryle’s tube dislodgement, simple ankle sprains, and minor wounds, are fairly straightforward. Logically, the more serious and life-threatening cases take precedence before these comparatively non-life-threatening conditions, resulting often in long waits for patients in the latter group.
It is well known that conditions such as retention of urine can be very painful, even though they are usually non-life-threatening, while delayed treatment of wounds can lead to worse outcome. These cases actually often require simple treatment and can be discharged quickly. In addition, previous studies 1 have found that long waiting times negatively affect patients’ perception of information, instruction, and perceived quality of care. Therefore, we find the need for a special team to treat these patients, not only to alleviate suffering by reducing their waiting time, but also to improve compliance to treatment by improving their perception of the quality of care and instruction, and to reduce congestion at the emergency department so as to allow clinicians to focus on the more serious cases with less pressure and distraction.
In 2013, our department designed a “Fast Track Protocol Driven Service” concept, where experienced nurses at our department were trained to assess and treat patients with selected conditions with close support from clinicians, following preset clinical protocols co-produced by doctors and nurses of the team.
Methods
Team building and training
A dedicated “Fast Track” team was built from scratch, and all team members were selected from experienced registered nurses of our department. They were trained in a structured manner specifically for this new service, making the transition from a nursing role into a semi-independent clinical role, with adequate skills and confidence to provide quality service to patients.
In 2013, the first batch of four nurses was recruited as trainees. Lectures and practical workshops were organized for all the clinical topics that were planned to be made into Fast Track Protocols. The first batch of protocols included the following topics: needlestick injury, nasogastric tube management, acute retention of urine, minor wounds management, incision and drainage for uncomplicated abscesses, foreign body ingestion, and minor scald injury. The focus of these lectures and workshops was on the clinical aspects of diagnosis and treatment. Emphasis was also put on clinical documentation, communication, and pitfalls. During the workshops, trainees had ample opportunities to gain hands-on experience in clinical procedures and equipment, for example, direct laryngoscopy.
To encourage in-depth learning and understanding, after the introductory lectures and workshops, each nurse was entrusted with the task of fashioning the drafts of one of the protocols that would be used for the Fast Track Service. Recommendations of reference books, local and overseas clinical guidelines as well as guidance on protocol writing were provided by doctors of the team, who subsequently edited the drafts, added appendices containing important clinical knowledge and illustrations, and finalized the protocols using a uniform structured template. These completed protocols were then sent to the Chief of Service of the department for his endorsement to activate these protocols in actual clinical service.
After the protocols were activated, an “internship” period was initiated. During this training period, selected patients would be interviewed and examined by Fast Track nurses under the supervision and guidance of the team doctors. The nurses’ documentations were also carefully checked for the quality of documentation. Constructive comments would be given, and any difficulties faced by the team nurses could be discussed and explored.
After the training period, team nurses could now operate independently, and the service was introduced to doctors of the department. The quality of service and documentation were closely monitored at any point of time. Quality assurance measures will be discussed in other sections.
In 2014, two nurses were further recruited into the Fast Track team as trainees for a 1-year period, and a logbook was designed to monitor training of team members. Each trainee was required to study a set number of previous cases and to see a number of cases under supervision. Existing team members were also given logbooks and were encouraged to study cases as revision themselves, while they coach new trainees with real patient cases.
After the training period of the second batch of trainees, a written test and an Objective Structured Clinical Examination (OSCE)-style assessment were organized with the expert assistance of an Associate Consultant experienced in simulation training, who kindly prepared clinical scenarios and advised on simulation-based assessment setup. Both existing team members and fresh trainees took part in the assessment. Both trainees passed the assessment while existing members also performed well in the assessment, which was regarded as a refresher exercise for them. A high level of adherence to protocols and good diagnostic accuracy were noted in our nursing team. Similar results were demonstrated in a study 2 involving the enhanced nursing service teams in several hospitals in Australia.
With a larger team of Fast Track nurses, new protocols could be developed to expand the scope of service, including the topics of ankle sprain, minor head injury, and back sprain. Again, lecture-workshops were arranged to familiarize members with clinical knowledge and physical examination skills. To enhance the accuracy of documentation and communication, reliable clinical decision tools and checklists such as the Ottawa Ankle Rules were incorporated into the Nursing Documentation Sheet, so that the whole doctor–nurse team would have an objective and identical idea of the patient’s condition.
Due to the shortage of nursing staff after 2016, the frequency of Fast Track service sessions was reduced to address manpower needs. However, Fast Track nurses remained active whenever there are suitable cases according to the protocol.
Operation of the fast track service
Potentially suitable patients for Fast Track Service according to the protocol are identified with a mark on their case files by the triage nurse which can be identified by Fast Track Nurses; however, these “marked” patients remain in the same queue as other patients of the same triage category before they are invited to be treated by our Fast Track service. A preset and uniform introduction of the Fast Track Service is given to the patient, and verbal consent is sought from the patient and recorded in the case notes. The patient is guaranteed that a doctor is ultimately responsible for all investigations, diagnosis, and treatment; therefore, this service is not a “lesser service for lesser patients” compared to the regular queue.
Results: Performance and quality assurance
Figure 1 demonstrated a steady growth of cases seen since the inauguration of the service. The number of cases seen in 2016 and 2017 showed a slight decline due to the lower number of duty shifts with Fast Track Service due to manpower shortage at our department.
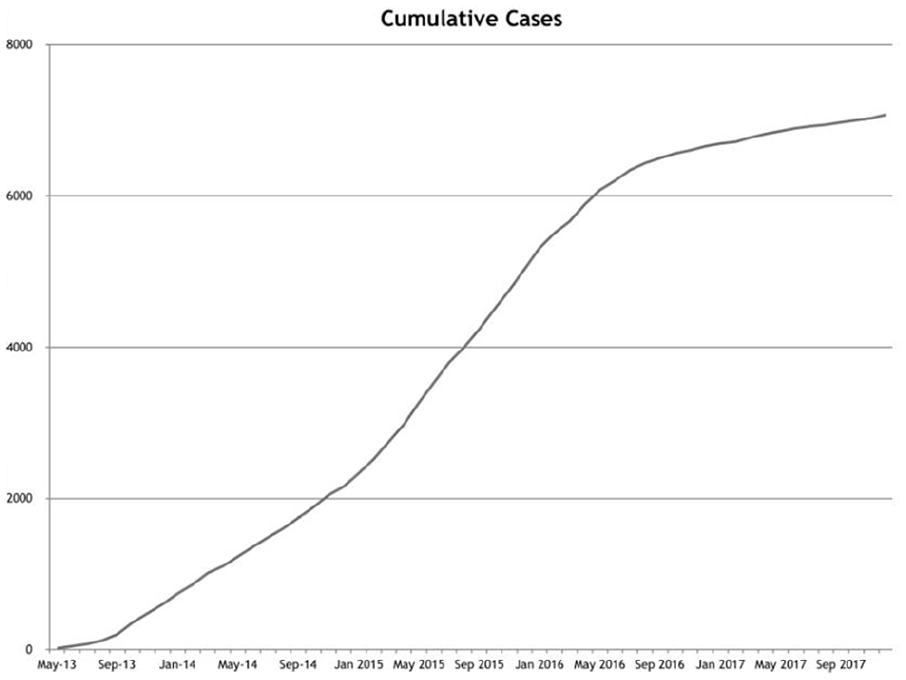
Cumulative number of cases treated by Fast Track Service.
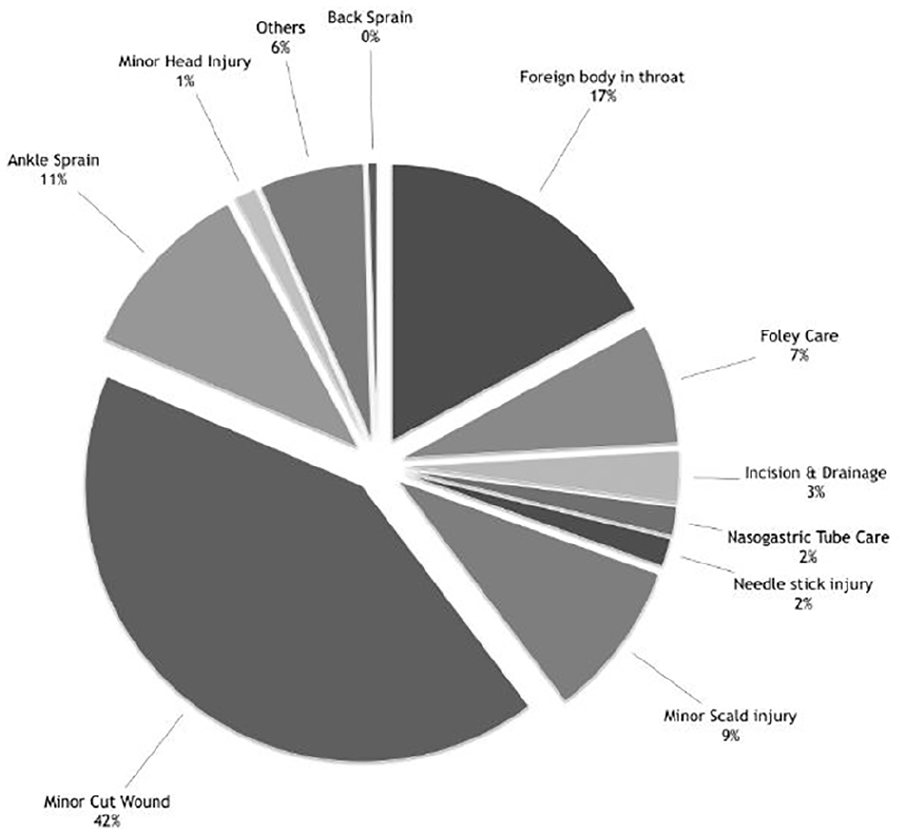
Figure 2 showed the spectrum and distribution of case types, displaying the versatility of the service.
A comparison of waiting time of patients being treated by Fast Track Service.
Figure 3 showed the resulting shortening of waiting time of patients who were treated by the Fast Track Service, thus allowing such patients to enjoy the benefit of better wound healing and less suffering.
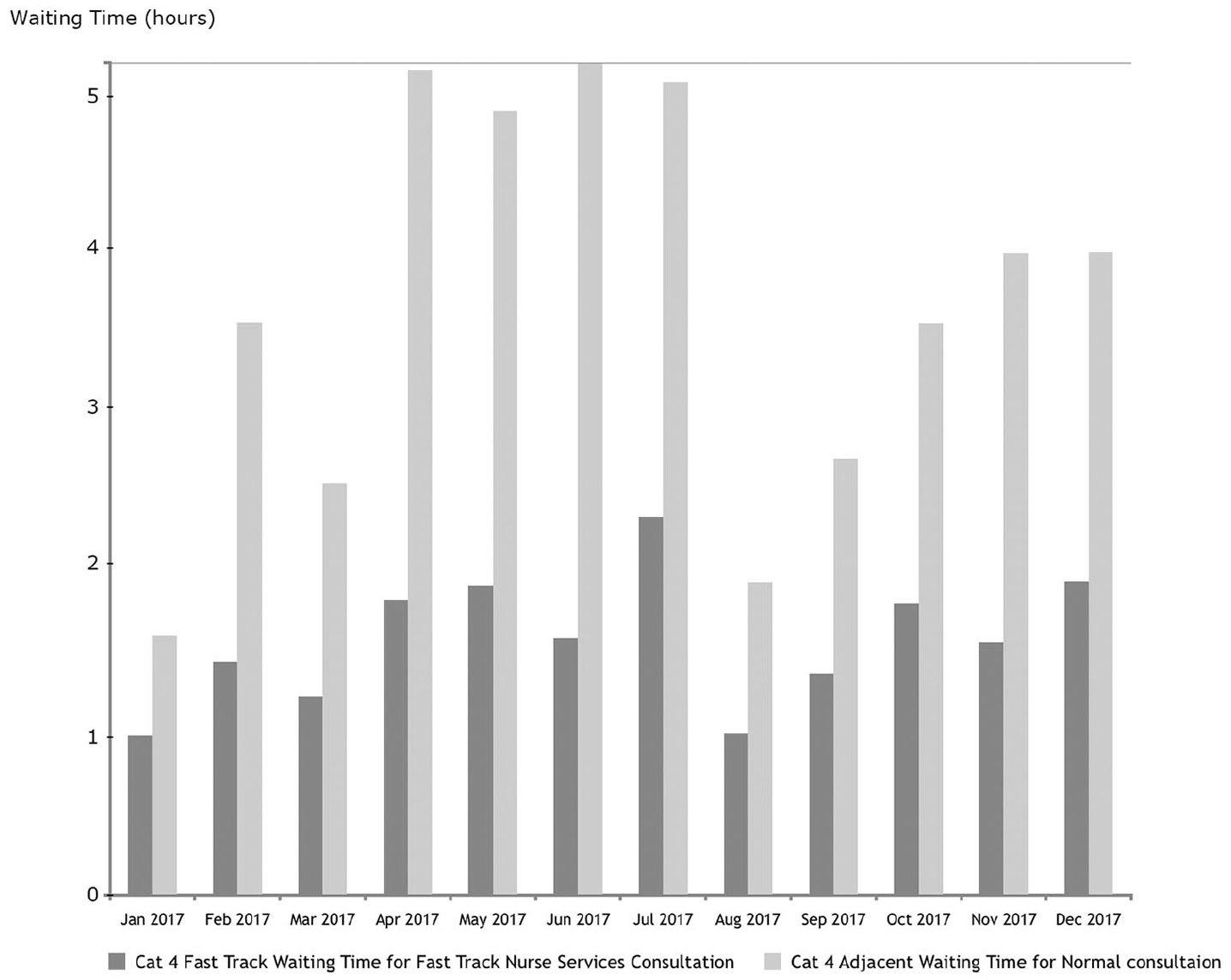
A comparison of waiting time of patients being treated by Fast Track Service against adjacent patients in the original queue.
To further ensure the quality of service, a few measures were implemented.
Each year, a selected number of cases were reviewed by doctors of the Fast Track Team in order to maintain the quality of documentation. Cases of re-attendance were screened for possible errors in the initial treatment or areas of improvement in patient communication. Our experience found that re-attendances caused by complications (e.g. wound infection) of cases treated in the Fast Track Service were rare, and no specific errors in the initial treatment were found. Since the responsible case doctors often personally inspect wounds, and the dressing or suturing treatments performed by the nurses were similar to the treatment in the regular queues, the re-attendances are not considered to stem from the Fast Track Service design.
In 2016, an independent assessor, who was a doctor of our department but who was not a part of the Fast Track Team, was invited to perform a clinical audit, to comment on the performance, and to give recommendations to improving service. No breach of protocol or documentation errors causing diagnostic and treatment errors were found.
A patient satisfaction survey modified with permission from a previously proven evaluation tool for nurse practitioner care in Canada 3 was also performed to understand how patients perceive the service. The results showed that the Fast Track Service was well received by patients, and there was good rapport between Fast Track Nurses and patients. The results and study of the validity of the statistics of the survey as a measurement of patient satisfaction 4 in our hospital were later published as a journal paper by our independent auditor.
Moreover, a paper introducing the present service was published in the Singapore Medical Journal in 2016. 5
Discussion
The Fast Track Protocol Driven nursing service of our department shares certain common objectives and methods as other “enhanced nursing service clinics” in other hospitals both local and overseas. However, there are a few special features of our service model that we will present in this section.
Designed to guarantee shortening of waiting time
In certain existing nurse-led service models, suitable patients are identified at triage and separated into a nurse-led queue to wait to be managed by nurse practitioners. However, there is no such division of queue in our Fast Track Nursing Service. Fast Track nurses only proceed to invite one potentially suitable patient still waiting to be seen by a doctor in the regular queue each time when he or she is ready to see a case. Once that patient agrees to go into Fast Track, he or she will be treated immediately. Hence, by design, the waiting times of each Fast Track treated patient is always reduced compared to the waiting time if they refuse Fast Track service and continue to wait for doctor consultation in the regular queue.
At the same time, the Fast Track nurse is always additional manpower not included in the general nursing duty roster; thus, the service to non-Fast-Track patients is never adversely affected. On the contrary, when a patient is taken up by the Fast Track Service, the queue behind that Fast Track patient is reduced immediately by one patient, creating a win–win situation.
Flexible staff
Contrasting with some other enhanced nursing service clinics, our Fast Track team nurses, apart from having undergone additional training, are no different in ranking or job position as any other registered nurse or advanced practice nurse in the department. Therefore, Fast Track nurses can perform both Fast Track service and general nursing service or resuscitation duties in the department at any time according to manpower needs. In fact, in our department, whenever one Fast Track team nurse is on Fast Track duty on a certain shift, the other Fast Track nurses who happen to be on duty on the same shift will be assigned as a member of the general and/or senior nursing staff. Nevertheless, the principle is that the Fast Track duty nurse of any shift is always an additional manpower.
On ordinary days with Fast Track nursing service, the assigned Fast Track nurse will dedicate her/his efforts in Fast Track cases and works independently from and is not counted as part of the general nursing staff.
In cases of overwhelming and extraordinary manpower needs, such as during disaster alerts, the Fast Track team nurse on duty could immediately take up roles in the general nursing team when resuscitation needs override those of non-life-threatening Fast Track cases. In these situations, nursing manpower is increased.
A doctor is responsible at all stages of consultation
The training of our Fast Track Team focuses on the initial assessment of the patient, that is, history taking and physical examination, as well as simple treatments such as wound, Foley, and Ryle’s tube management. However, Fast Track nurses are not officially empowered to document X-ray findings, order investigations such as X-rays or wound swabs, make diagnoses, or to prescribe medications. This approach allows the Fast Track nurse to facilitate the assessment of patients to shorten their waiting time, but also ensure a doctor actively takes responsibility and communicates with the nurse in every step of the case, instead of simply signing off the case. In this way, Fast Track patients actually enjoy “dual channel care,” that is, firsthand knowledge of the case from the beginning to the end by both the nurse and the doctor, compared to the usual case where nursing involvement only begins after a doctor has seen the case single-handedly and focuses mainly on following treatment orders.
Enhancement of clinical knowledge of nurses
Fast Track nurses are trained in more clinical aspects than other nurses and have a more global picture of the clinical logic of diagnosis and treatment, since a Fast Track nurse is required to manage each patient from the initial assessment phase to the investigation phase, and then to the diagnosis, management, and discharge phase. They are also vigorously trained to identify “red flags” during patient assessment. Many of our Fast Track nurses are advanced practice nurses (senior nurses), and their enhanced knowledge of clinical logic and sensitivity toward “red flags” would also help them make decisions with a more holistic view as a nurse-in-charge when they are not on Fast Track duty, thereby benefitting patients as a whole and not limited to Fast Track cases. Fast-track nurses also became more interested in reading X-rays and wound outcome etc., as they have a greater sense of involvement and achievement under this service. This led to better first-hand knowledge, for example in the patterns of ankle injuries and complications of foreign body ingestion, which could in turn be applied onto future patients they encounter.
Conclusion
Since an emergency department faces a wide diversity of patient conditions each day, a “diverse patients, diverse service” management approach is required to facilitate patient care. Our Fast Track Enhanced Nursing service is a model of tailored service diversification to shorten waiting times, improve patient satisfaction and outcome.
Footnotes
Acknowledgements
We would like to thank Ms. Leung Yuen Fan Fanny (Department Operations Manager) for her contribution toward nursing and resource management of the service, and Ms. Law Chi Wai Eliza (Advanced Practice Nurse (APN)), Ms. Mok Shuk Man Anson (APN), Mr. Siu Chun Bong Maverick (APN), Ms. Yang Siu Fan (APN), and Ms. Ng Wai Chun Oliver (Registered Nurse) for managing the statistics of the service and developing the charts and figures of this report.
Author contributions
NHY, FKP, and LCM wrote the draft of the manuscript, and all reviewed and revised the manuscript. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data are generated from our own clinical service statistics.
Informed consent
Informed consent is not applicable, as no patient data or study on patients was involved in this article.
Ethical approval
Ethical approval is not applicable, as no patient data or study on patients was involved in this article.
Human rights
Human rights are not applicable, as this article does not involve any clinical study on patients.