
Abstract
Background:
Rapid access clinics are an increasingly common model of care in tertiary hospitals. Early streaming of suitable patients to appropriate clinic services could reduce Emergency Department overcrowding. This study set out to investigate the current utilisation of rapid access clinic dispositions in a tertiary centre. The findings have led to useful mapping of local services and early nurse led identification of patients suitable for streaming to clinic locations.
Methods:
A cross-sectional observational study in a tertiary centre. Complete lists of consecutive discharged Emergency Department patients were generated by a trained data manger. Individual electronic medical records were reviewed for evidence of clinic disposition, patient demographics and compared with concurrent Emergency Department patients who were not referred.
Results:
1367 patients included from 144 h of consecutive weekday presentations. Referral to clinic locations occurred in 179/1357 (13.2%) with rapid access clinics utilised in 129/179 (70.4%). No difference in median length of stay was observed for patients referred to clinics (3.9 h) versus patients not referred (3.8 h) (p = 0.29).
Conclusion:
In a tertiary Emergency Department setting, discharged patients were frequently referred to rapid access clinics. Early streaming to suitable outpatient locations may be an additional strategy to consider for mitigating Emergency Department overcrowding.
Background
Reducing overcrowding in the Emergency Department (ED) requires well-defined models of care and a whole of hospital approach. 1 Early streaming to alternate locations has been cited as an effective strategy, and there is evidence that patients with low acuity presentations (LAPs) are a significant contributor to overcrowding.2,3 Furthermore, early senior review has been shown to improve the appropriate use of outpatient facilities.4,5
Geographical location and size of the ED may contribute to the characteristics of LAPs. In rural settings, general practice (GP) presentations often predominate, whereas in urban settings, where access block is also frequently severe, LAPs may be appropriately referred by their GP to access tertiary services.3,6 Recently, in our Australian setting, we have observed an increase in LAPs referred to our EDs that are not suitable for GP review. Many of these patients present to access specialist tertiary services such as ophthalmology and cardiology. Over the same period, we have also observed an increasing number of rapid access clinics (RACs) available for ED referral. An RAC is an outpatient review location generally accessible only by the ED or inpatient teams and routinely booked within 2 weeks of discharge. Given the expanding array of clinic locations, an understanding the processes involved in disposition to these models of care and optimising referral was seen as an important priority in our department.
Studies of LAPs in the ED generally focus on the effectiveness of GP co-location with such interventions having a variable effect on overcrowding. 7 A recent systematic review examining various strategies to reduce ED overcrowding did not cite any articles on streaming to clinics. 7
To assess LAPs in our ED, we conducted a small observational study to examine the incidence of referral to RACs following discharge. The objectives were to assess the length of stay of patients discharged to clinics and to understand where patients were commonly referred in a hospital with over 150 listed clinics. Following the collection of data, as a wider quality improvement initiative, the findings were collated with a view to applying them our clinical practice. Specifically, we targeted improvements in ED patient flow via early streaming to clinics by triage nurses and senior doctors. Abbreviated instructions on how to stream LAPs to clinics were mapped and new infographics allowed ED staff to flag suitable patients early in their visit.
Materials and methods
Study setting
Westmead Hospital is a university affiliated tertiary centre. Study protocols were approved by the local Human Research Ethics Committee (HREC Code 1901-08).
Inclusion criteria
The inclusion criteria were: (1) discharged from ED < 24 h; and (2) electronic discharge plan available for review.
The exclusion criteria were: (1) deceased; (2) ward admission; (3) discharge against advice; (4) inter-hospital transfer; (5) no discharge time; and (6) uncertain disposition.
Outcome measures and analysis
Data were collected in December 2018 by a single investigator. Electronic medical record (EMR) presentation lists were generated by a trained data manager. Two distinct 72 h samples of weekday presentations were used.
Discharge summaries were individually reviewed for formal discharge disposition and to identify if ED discharge included referral to outpatient clinic(s) (primary outcome). Additional data recorded included age, gender and total length of stay. Assessments by the primary investigator (T.S.) were cross-checked by a second investigator (A.C.). Following data collection, stakeholders responsible for clinic-based models of care across the institution were consulted in semi-structured phone interviews and their responses were recorded and assessed via latent analysis. In order to measure the impact of the quality improvement intervention described 6 months following implementation, a staff survey was completed (n = 106) and ED overall performance was audited.
Medians and interquartile ranges (IQR) are reported for the data presented. For comparative analysis, valid differences are reported using the Mann–Whitney U test with significance level was set to p < 0.05.
Results
1367 patients presented over two distinct 72 h periods of weekday sampling (Table 1). 810/1367 (59.3%) ED patients had a discharge plan documented in the EMR, with 169 referred to tertiary clinics.
Characteristics of clinic referrals from the Emergency Department (two cohorts).
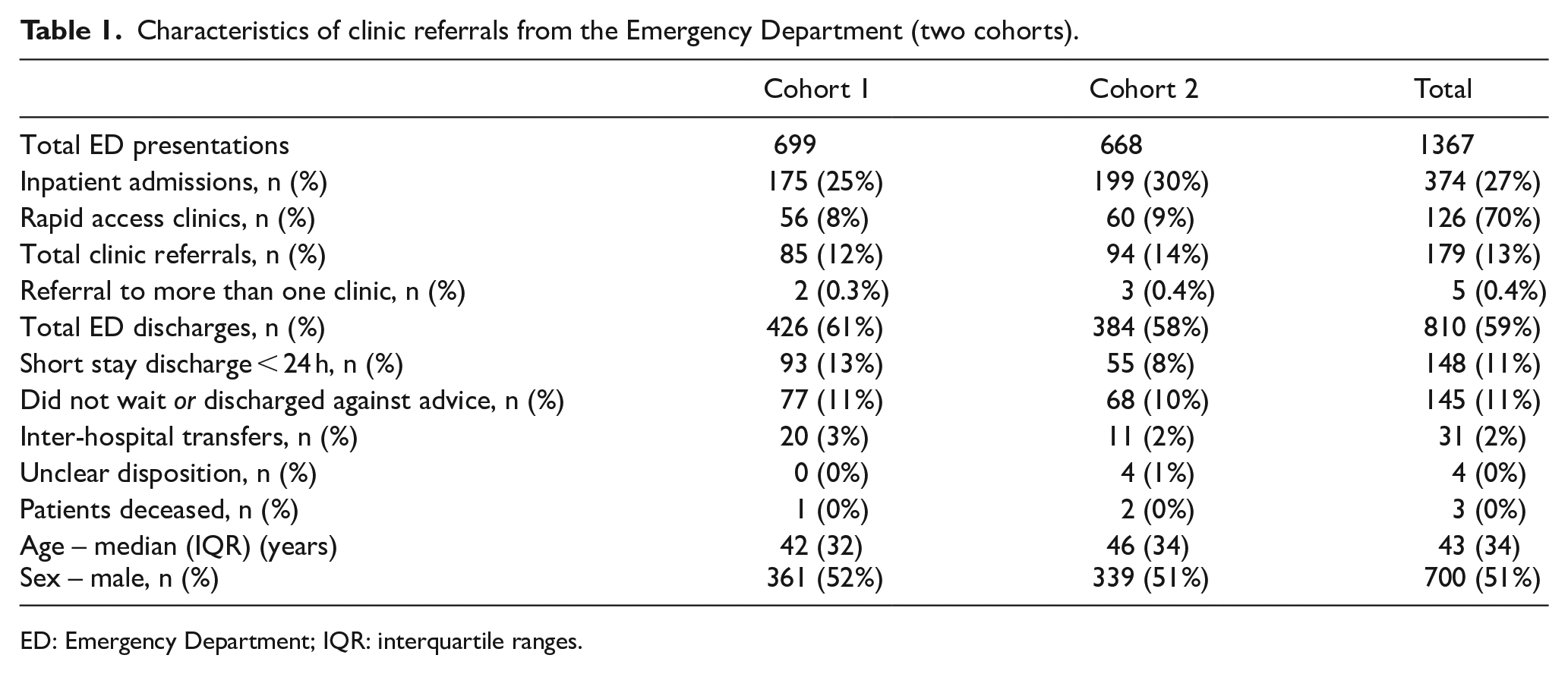
ED: Emergency Department; IQR: interquartile ranges.
There was no significant difference in median length of stay between patients discharged with clinic follow-up (3.9 h, IQR 2.93) versus without clinic follow-up (3.8 h, IQR 3.13) (p = 0.289). Table 2 outlines the various disposition locations. The most frequent disposition clinics were ophthalmology, pregnancy, cardiology, neurology and plastics. All of these locations are RACs with access within ⩽2 weeks.
Characteristics of clinic referrals by specialty (n = 179).
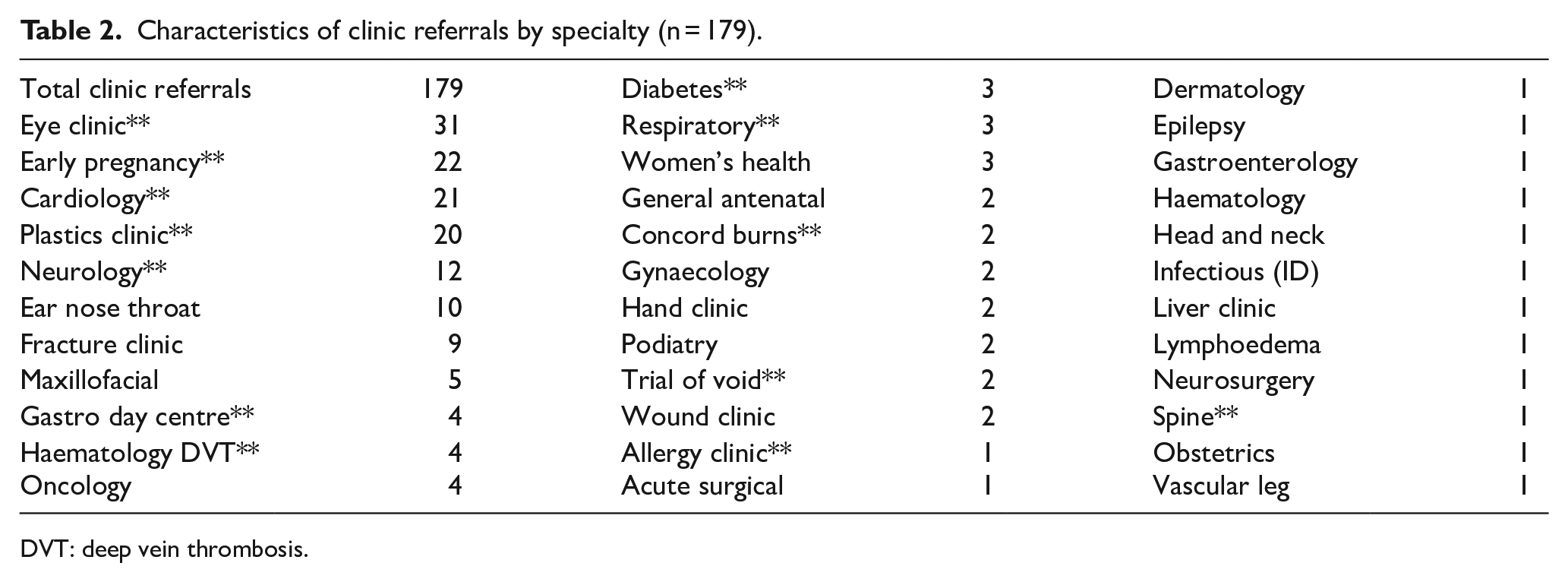
DVT: deep vein thrombosis.
Following the latent analysis of phone interview of clinical leads of the identified models of care, we constructed a map of the processes required to efficiently refer a patient to the various clinic models of care (Figure 1). Of the medical and nursing staff using the cards following implementation, 106 staff were surveyed, of which 81/106 stated that they regularly use the resource to aid in patient disposition to RACs. Furthermore, following implementation, overall time to leaving the ED for discharged was reduced to 3.2 h (IQR 2.95) despite an observed increase in ED access block in the intervening period.
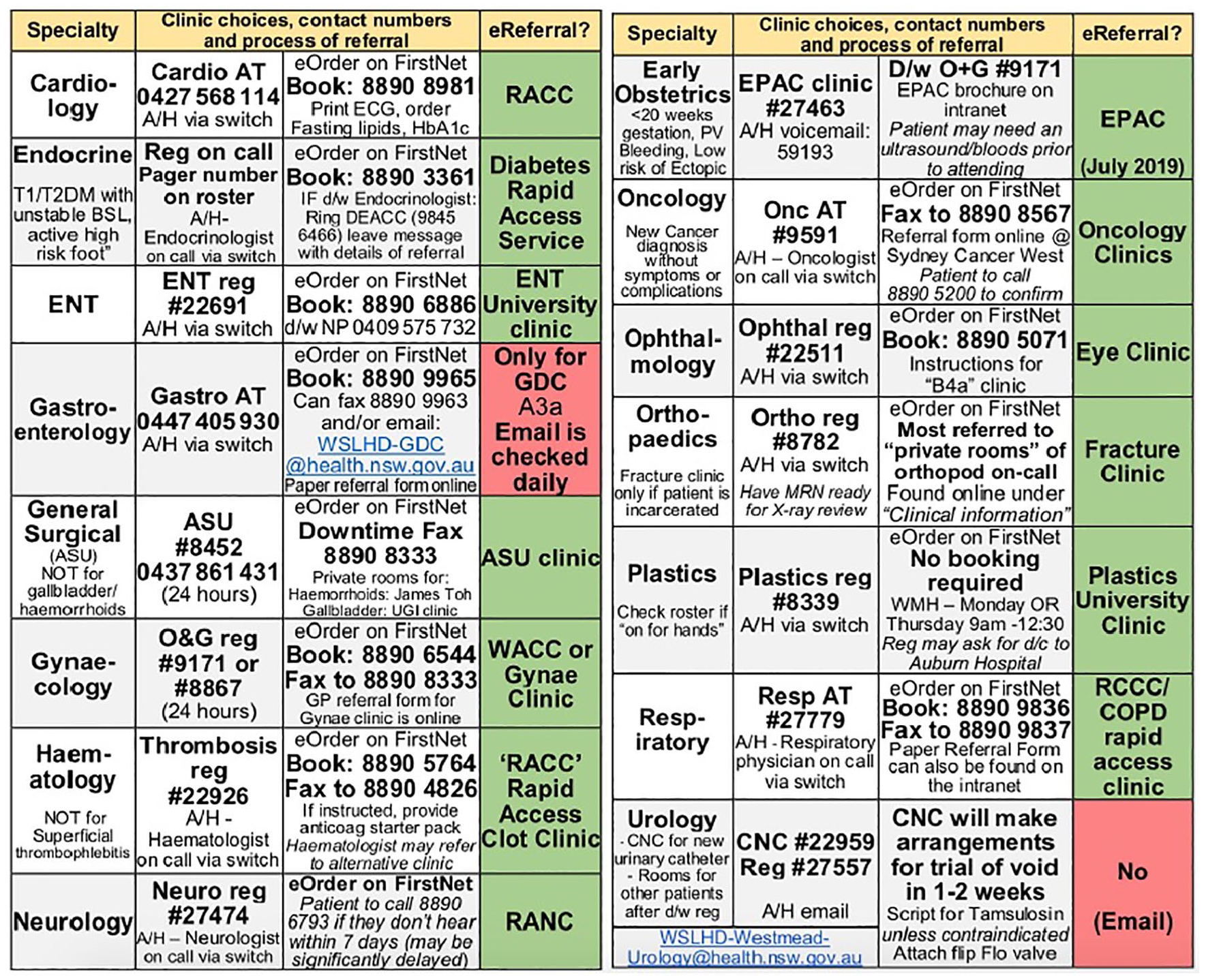
Identification card tag (two-sided).
Discussion
Prior studies of LAPs in the ED have predominantly focused on the effectiveness of co-located GP services. 7 The findings from studies focussing on the effectiveness of co-located primary care services may not be applicable to all types of ED patients because many urban centres have a low number of GP patients when compared with rural settings.3,6 Furthermore, results from the studies on early redirection to co-located services have been conflicting on whether these strategies reduce ED overcrowding. 2
In this study, we observed a surprisingly high utilisation of ED referral to both RACs and general clinic locations following ED discharge (Table 2). Furthermore, it appears that the streaming of patients to RACs was especially prevalent accounting for 70.4% of ED referrals despite accounting for only around a quarter of the hospital clinic capacity. It is therefore notable that at the same time we also unexpectedly observed that patients referred to clinics at discharge had a similar length of stay to other ED patients. In our view, this finding may suggest that improving identification and early streaming of suitable LAPs may be a pertinent strategy to reduce overcrowding as well as improve the overall patient experience. 4
Following data collection, stakeholders responsible for clinic-based models of care across the institution were consulted leading to improved mapping of the available streaming options (Figure 1). These process maps were disseminated via spaced educational interventions and summarised in a laminated cognitive aid. Translation to ‘on the floor’ practice was observed in the short term because information on RACs was available in multiple formats. With the advent of RAC models of care becoming an increasingly common means of service provision, it would seem prudent to further study both the effects on patient care but also on ED patient flow. 8
Our local ED team are now able to readily access information about clinic referral using either a smartphone application, laminated ID card or local intranet and the content is utilised by both nurses and medical officers. 9 Further work in this area could focus on a number of areas, including the sustainability of the changes to workflows described, identification of suitable patients by triage nurses and the overall effectiveness of the quality improvement changes listed with the study results used as a comparative baseline. 10
Limitations
The main limitations regard the single tertiary centre location and underlying observational methodology. This could lead to various forms of bias. Any new approach to improving streaming of patients or reducing ED overcrowding requires a holistic approach and recognition that sustained change is challenging. We acknowledge that the improved streaming to clinics observed can only provide a small impact in this setting and we ideally would have presented further patient or staff survey data to support our conclusions. 1
Conclusion
In this study, we observed that ED patients were often referred to RACs at discharge. Improving the ED interdisciplinary team’s knowledge of relevant outpatient pathways and ensuring that staff are able to quickly flag suitable patients may have a small role in improving ED patient flow.
Footnotes
Acknowledgements
The authors acknowledge the contribution of our Emergency Department data manager Mrs Shannon Joyce, who assisted with the data extraction in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The study was approved by the local Human Research Ethics Committee (HREC) – November 2018.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by departmental resources only.
Human rights
No identifiable patient information is used or was evaluated in this study.
Informed consent
No identifiable patient information is used or was evaluated in this study.