
Abstract
Introduction:
Headache is one of the most common complaints of patients after head trauma. The aim of this study was the comparison of the analgesic effects of intravenous ketorolac, morphine, and paracetamol in patients with headache following head trauma.
Methods:
This clinical trial was performed on 105 referred patients to emergency unit with headache after head trauma. Patients were randomly divided into three groups of intravenous paracetamol (15 mg/kg in 100 mL normal saline), intravenous ketorolac (30 mg/kg in 100 mL normal saline), and intravenous morphine (0.1 mg/kg in 100 mL normal saline). Headache severity and side effects of drugs were assessed at baseline and 15, 30, and 60 min after intervention.
Results:
Headache severity score at baseline was similar among groups. After 15 min, headache severity score in paracetamol group was significantly lower than that in morphine and ketorolac groups (3.7 vs. 4.6 and 4.5, respectively). After 30 min, the score in paracetamol and ketorolac groups was significantly lower than that in morphine group (1.9 and 2.4 vs. 3.2, respectively). After 60 min, headache severity score in three groups was similar (1.6 in morphine and ketorolac groups and 1.5 in paracetamol group). The incidence of side effects in morphine group was significantly more than that in paracetamol and ketorolac groups.
Conclusion:
In emergency department, intravenous paracetamol and ketorolac obtain a faster and more effective onset compared with morphine for headache after head trauma.
Introduction
Traumatic brain injury is one of the most important causes of traumatic mortality and disability. 1 Headache, as one of the most common complaints in medicine, is the most common complaint of patients after head trauma. The prevalence of headache after trauma was different in studies, depending on the time and duration of follow-up, between 30% and 90% of the patients suffer from headache following head trauma. 2
There are a variety of opinions about headaches etiology after head trauma. 3 Pain is one of the main barriers to examination, diagnosis, and treatment. So, the management of pain in these patients is an important challenge in emergency units. 4 Inadequate or wrong headache treatment can lead to chronic daily headache and/or chronic headaches associated with medication overuse. 5 Treating a headache following a head trauma may be complex and difficult because many factors—such as musculoskeletal, vascular, visceral, neurological, and iatrogenic factors—are involved. 6 Studies on treating this headache are limited and group therapy is recommended. 7 Currently, headache treatment after trauma is only based on symptoms and solely aimed at reducing headaches. 8 The ideal analgesic for pain control should be fast acting, effective and has minimal side effects and minimal interactions with other medications. 9
In acute treatment, some medications such as ibuprofen or other non-steroidal anti-inflammatory drugs (NSAIDs), dexamethasone, and morphine are used to treat migraine headaches.10,11 Opioids, including morphine sulfate, are the most used and effective analgesic drugs in the emergency department which their most important complication is the reduction of patients’ consciousness that can disrupt the clinical evaluation of traumatic patients.12,13
Ketorolac is also one of the most commonly used potent analgesic drugs in the NSAID category, but its use is limited, especially in patients with trauma, due to its many side effects.14 –16 Ketorolac is a nonselective cyclooxygenase (COX) inhibitor, and its mechanism of action refers to the specific biochemical interaction through inhibition of prostaglandin synthesis by competitive blocking of the enzyme. 17 The analgesic effect occurs within 30 min, with the maximum effect between 1 and 2 h and duration of 4–6 h. 18 Gastrointestinal bleeding, renal impairment, liver dysfunction, and possible allergic reactions which reported as adverse events of NSAIDs are possible after the use of ketorolac, significantly in higher doses, increased duration of use, and in the elderly. 17
Paracetamol is a non-opioid, non-inflammatory analgesic drug with central effect that elevates the pain threshold in the central nervous system. 19 The exact mechanism of action of paracetamol is still unclear and seems that it has a multifactorial mechanism of action. Several theories such as the inhibition of the COX pathways, linked with both direct and indirect stimulation of the cannabinoid, nitric oxide synthase, and serotonergic pathways have been proposed. 20 Intravenous paracetamol is administered over 15 min with an onset of action in 10 min. 21 The adverse events of paracetamol are limited, and it has been safe and effective in pain control as successful as opioids, with no significant side effects.8,9,22
In most of emergency setting, especially in developing countries, despite the existence of known side effects, morphine has classically been the agent of choice for pain management in patients with trauma. Whereas it seems that paracetamol and ketorolac can be more suitable analgesic in patients with trauma. However, the studies regarding the comparison between analgesic effect and complications of paracetamol and ketorolac with morphine in patients with head trauma are limited. So, this study is aimed to compare the analgesic effects of intravenous ketorolac, morphine, and paracetamol in patients with headache following head trauma.
Methods
This clinical trial was performed on patients with headache after head trauma who referred to emergency department of Hamadan Besat hospital. This is a general hospital with 540 beds that known as referral center of traumatic patients. The hospital emergency department provides 50 beds, which has the average daily attendance about 800 patients. The protocol of this study approved at the Ethics Committee, and the informed consent was obtained from all participants before the beginning of the study. The inclusion criteria were as follows: age 18 years or older, head trauma within 24 h before referring to the hospital, having a headache severity score of more than 4 (from 10 score) based on a visual analog scale (VAS). Trauma was confirmed based on history, clinical examination (observation of trauma signs such as ecchymosis and scratching in the head and face), and trauma mechanism, and if necessary, brain computed tomography (CT) scan findings. Patients with concurrent traumas, abnormal level of consciousness (Glasgow Coma Scale (GCS) < 14), abnormal neurological findings, bleeding and pathological lesions in brain CT scan, thrombotic disorders or taking an anticoagulant, previous history of chronic headache, history of drug allergy and asthma, kidney, liver, heart and lung diseases, history of drug addiction, and patients who had consumed analgesic 6 h before the visit, as well as pregnant women were excluded from the study.
Patients were randomly divided into three intervention groups using a randomized block design in block size of six. Group 1 included 35 patients who received intravenous paracetamol (1000 mg/10 cc per vial) 15 mg/kg per 100 cc normal saline serum in an infusion of 15 min. Group 2 included 35 patients who received intravenous ketorolac (30 mg/cc per ampoule) 30 mg per 100 cc normal saline serum in an infusion of 15 min. Finally, group 3 included 35 patients who received intravenous morphine (5 mg/cc per ampoule) 0.1 mg/kg per 100 cc normal saline serum in an infusion of 15 min. In order to blind the study, all drugs were administered in the same manner (intravenous infusion), and the patients were not aware of the type of administered drug. The studied drugs were prepared in the emergency room in coded infusion bags by a collaborator physician, who did not interfere in collecting data. Patients’ data were collected using a checklist by a nurse who was not aware of the type of used drug by patients.
The primary outcome in this study was headache severity which was assessed at baseline, and 15, 30, and 60 min after intervention by the VAS using a vertical line with 10 cm length on paper (0 means no headache to 10 means worst headache imaginable). The secondary outcome was side effects included the occurrence of nausea, vertigo, allergy, alteration of consciousness, and hypotension during study period. During the study, in each time point, patients were asked about the presence of nausea and vertigo. Also, allergy was defined as any adverse drug reactions reported during study period. Hypotension was defined as any systolic blood pressure of 90 mm Hg or lower, and alteration of consciousness was defined as the presence of feeling dazed or confused, having difficulty thinking, or revealed decreased mental status by the neurologic exam.
The sample size calculation was based on headache severity score (as primary outcome) using the comparison of mean formula with two-sided log-rank test, α = 0.05, and 99% power. Using the mean values of headache score and their respective standard deviations (SDs) in paracetamol and morphine groups from a previous study, 8 allowing for a sample size of 35 patients per group. Collected data were analyzed by SPSS software for Windows (version 23; SPSS Inc., Chicago, IL, USA). Descriptive data are reported as mean ± SD and number (%) for continuous and categorical data, respectively. Independent sample t-test, chi-squared test, one-way analysis of variance (ANOVA), and repeated measurements of ANOVA were used to comparing studied variables among three groups as appropriate. The level of significance is considered to be less than 0.05.
Results
Figure 1 shows the flowchart of the study. 122 patients with headache after head trauma were reviewed for eligibility, 11 patients were not eligible, and six patients refused the informed consent. 105 patients randomly assigned into three groups. Follow-up period in all patients was 60 min, and all the patients in three groups were included in final analyses.
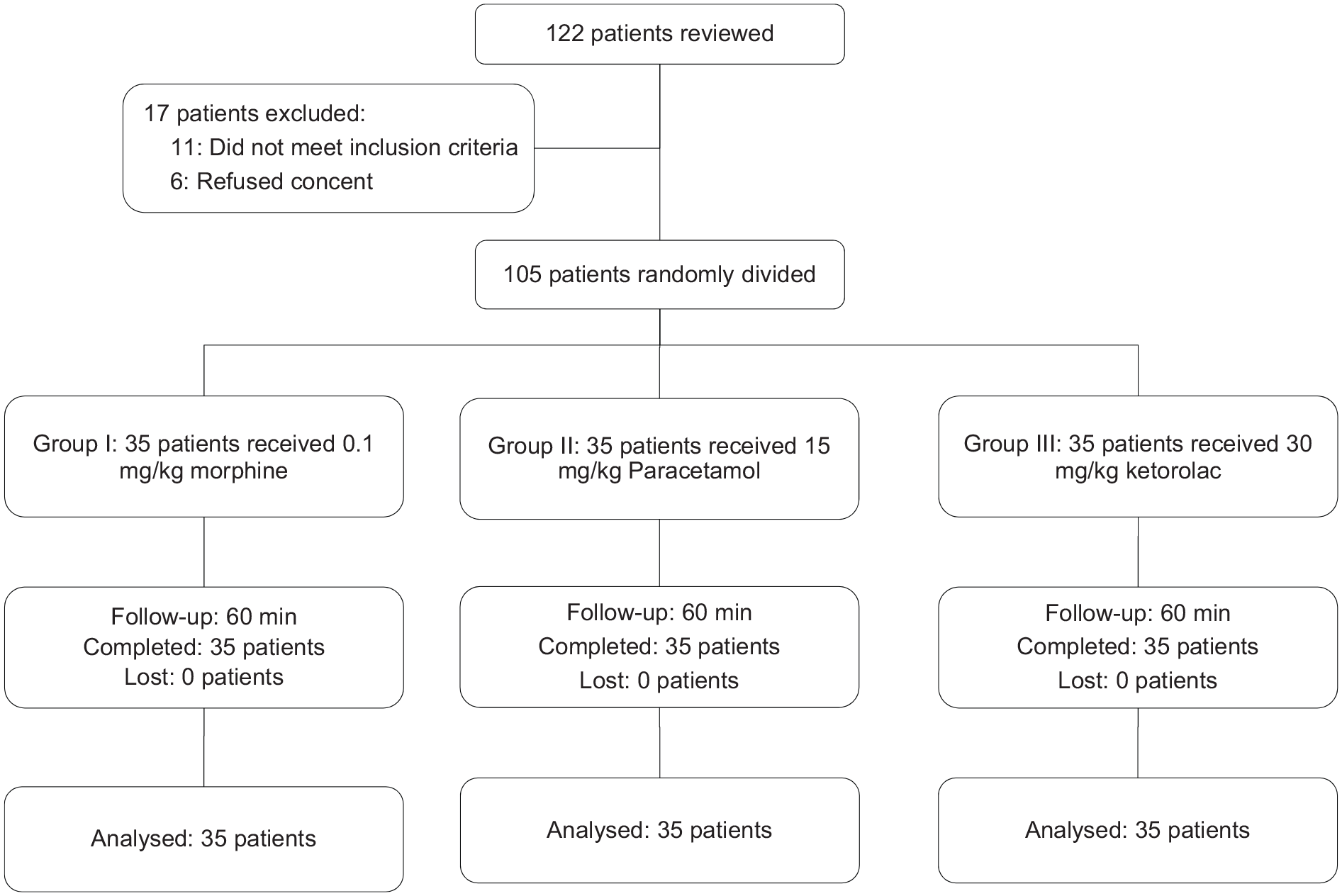
Flowchart of the study.
Studied patients were included 67 male (63.8%) and 38 female (36.2%) with the mean age of 32.2 ± 1.8 years. The baseline characteristics of studied patients are reported in Table 1. Patients’ age among studied groups was similar, and no significant differences were noted between groups (p = 0.269). Also, frequency of sex was not significantly different among groups (p = 0.585).
Baseline characteristics of studied groups.
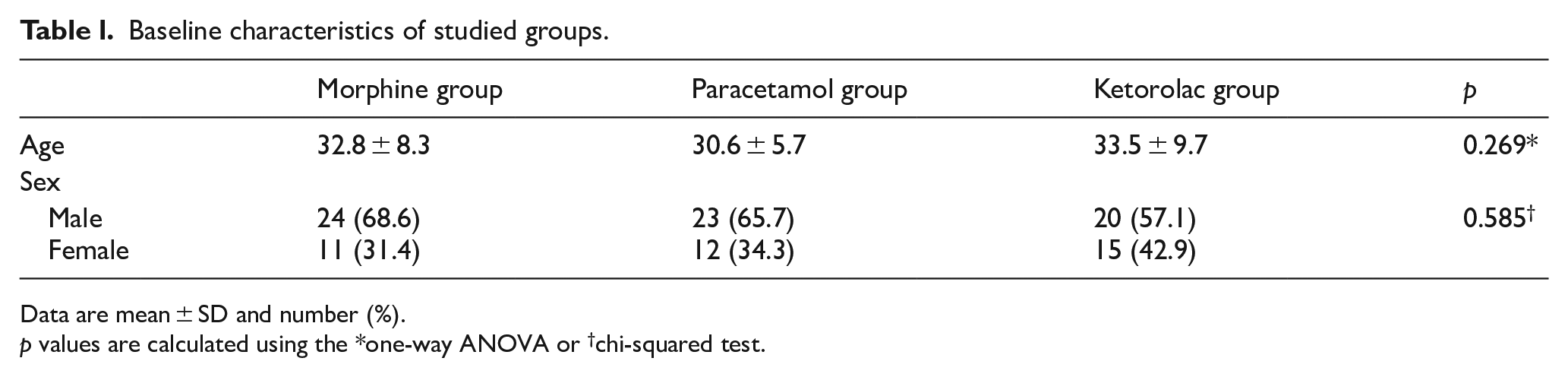
Data are mean ± SD and number (%).
p values are calculated using the *one-way ANOVA or †chi-squared test.
Table 2 shows comparison of headache severity score among studied groups. At baseline, headache severity score among groups was similar (p = 0.708). In three groups, headache severity score was significantly decreased during 60 min of follow-up period (p = 0.0001). After 15 min, the score in paracetamol group was significantly lower than that in morphine and ketorolac groups (p = 0.010). 30 min after intervention, the score in paracetamol and ketorolac groups was significantly lower than that in morphine group (p = 0.001). But, headache severity score 60 min after intervention among groups was not significantly different (p = 0.832). Trend of changes in headache severity score during study period among groups was not significantly different (p = 056; Figure 2).
Comparison of headache severity score during study period in 105 patients with head trauma.
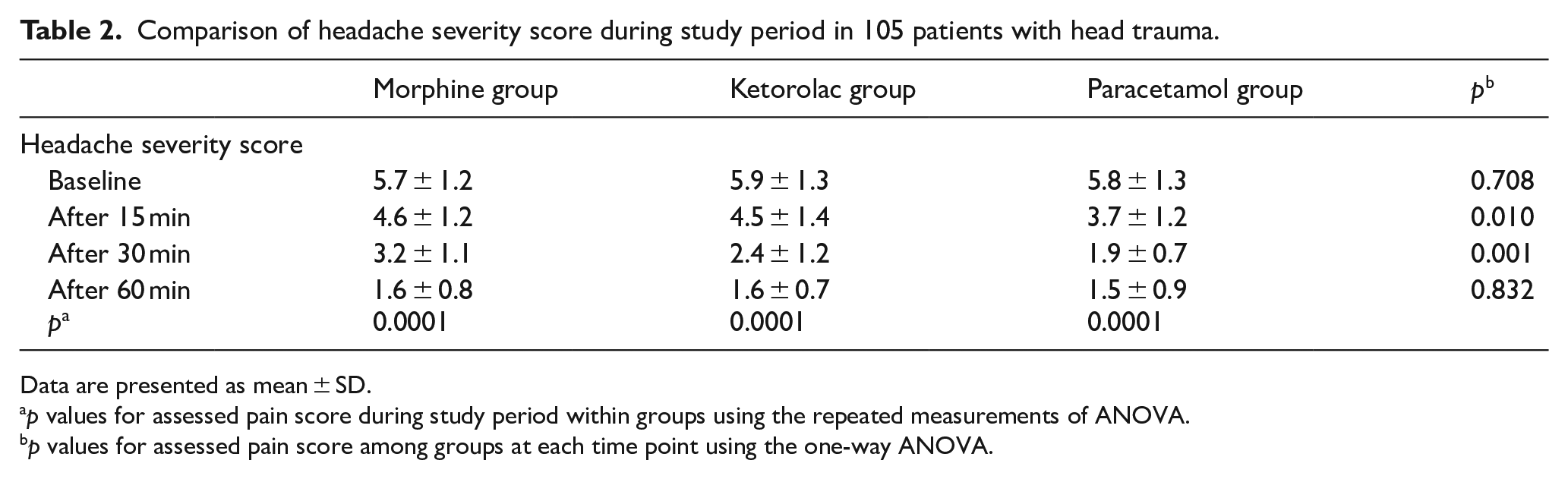
Data are presented as mean ± SD.
p values for assessed pain score during study period within groups using the repeated measurements of ANOVA.
p values for assessed pain score among groups at each time point using the one-way ANOVA.
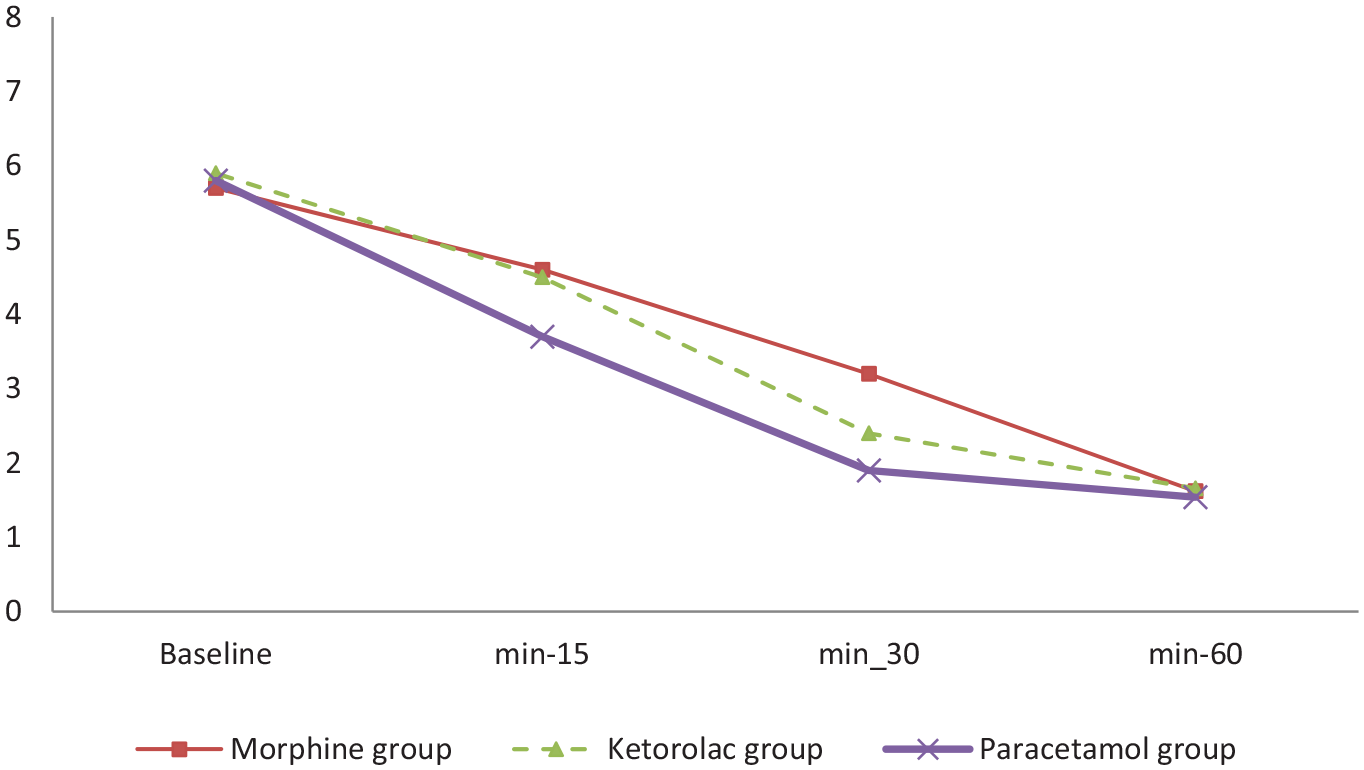
Trend of headache severity score during study period among groups by repeated measurements of ANOVA (p = 0.056).
Table 3 shows the incidence of side effects in the three groups. The incidence of side effects in morphine group was significantly more than that in paracetamol and ketorolac groups (p = 0.0001). In total, 85.7% of patients in morphine group reported one or more side effects whereas in ketorolac group only 34.3% and in paracetamol group only 11.4% of patients reported side effects. The incidence of nausea, alteration of consciousness, and hypotension in patients in morphine group was significantly more than that in the other two studied groups (p < 0.05). Vertigo and allergy were more frequent in morphine and ketorolac groups than those in paracetamol group (p = 0.001).
Comparison of side effects during study period in 105 patients with head trauma.
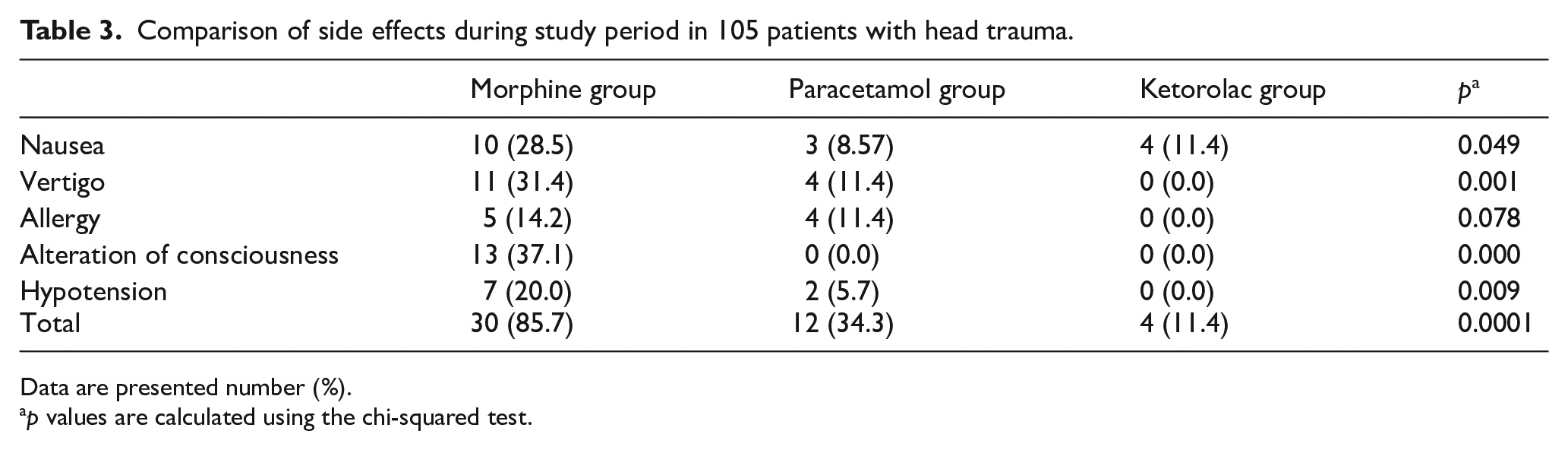
Data are presented number (%).
p values are calculated using the chi-squared test.
Discussion
In this study, the analgesic effect and side effects of paracetamol, morphine, and ketorolac in 105 patients with headache after head trauma were assessed. Our results show that 15 min after intervention, headache severity was decreased in 35%, 25%, and 20% of patients, and after 30 min, reduction is reported in 68%, 59%, and 43% of patients in paracetamol, ketorolac, and morphine groups, respectively. In generally, statistical analysis showed that fast efficacy was related to paracetamol. Most cases of nausea, vertigo, allergy, alteration of consciousness, and hypotension in our study were related to morphine. Nausea and vomiting are the most complications of trauma, 23 but since this study has been performed comparatively and more nausea and vomiting in the morphine group are due to the side effects of the morphine drug.
The lowest incidence of vertigo, allergy, alteration of consciousness, and hypotension was related to paracetamol group and the lowest incidence of nausea was observed in the ketorolac group. This low number of nausea and vomiting may be result from trauma to head rather than drug side effects. The difference among the groups was significant in terms of drug side effects, except for impaired consciousness. In addition, other observed side effects in morphine group were included such as two cases of weakness and lethargy, two cases of status hypotension, and one case of abdominal cramp.
This study is the first research to compare the efficacy of morphine, paracetamol, and ketorolac in management of patients with headache after trauma. In Vahdati et al.’s 8 study, the morphine and paracetamol in 60 patients with headache following the trauma was compared, and showed that paracetamol was more effective and safer than morphine. This is similar to our findings. In a study by Steven Chan et al., treatment of migraine headache after head trauma in children with ketorolac, ondansetron, and metoclopramide was compared. They showed that ketorolac was effective in 80% of cases which is more than our results. 24 In Esmailian et al.’s study, the paracetamol and morphine drugs had similar analgesic effects on patients with rib fracture. The efficacy of these drugs was 80% for paracetamol and 58.6% for morphine after 30 min. In this study, the rapid effect of paracetamol compared to morphine confirms our findings. 25 In a study by Moller et al., 26 paracetamol had greater effect in controlling physical pains after pediatric herniotomy surgery compared to placebo. Sinatra et al. 9 reported that paracetamol in patients undergoing hip or knee surgery reduced the need for opiates during the first 24 h after surgery.
In Van Aken et al.’s study, the effects of paracetamol and morphine on pain control after dental surgeries have been compared and indicated that these two drugs have significant effects compared to placebo but there is no significant difference between the two drugs, while in our study the paracetamol had more efficacy than morphine. 27 In a study by Craig et al., 28 on the control of acute traumatic limb pain, no significant difference was found between the efficacy of morphine and paracetamol, but paracetamol side effects were lower than morphine in similar to those of our study. Bektas et al. investigated the effects of paracetamol on the pain control of patients with renal colic and compared to morphine. They showed that the efficacy and side effects of paracetamol were lower than morphine. 29 Holdgate and Pollock 30 indicated that NSAIDs are more effective and less complicated than morphine in controlling renal colic, which confirms the results of our study.
In conclusion, intravenous paracetamol is an appropriate pain reliever in the emergency unit to control headache after the head trauma, with fast effects and lower side effects compared to intravenous ketorolac and morphine, after that intravenous ketorolac has faster effects when compared to intravenous morphine and had lower incidence of side effects. So, intravenous paracetamol and ketorolac can be used as available and appropriate alternative of intravenous morphine to managements of headache after the head trauma.
Footnotes
Acknowledgements
The authors acknowledge that this article has been extracted from an emergency medicine specialist thesis at the Hamadan University of Medical Sciences.
Author contributions
A.A.F. and R.S. contributed to the design of the work, conducting the study, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work. A.A. and J.P. contributed to the conception of the work, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Hamadan University of Medical Sciences.
Availability of data and materials
Data are available from the corresponding author upon reasonable request and with permission.
Informed consent
Informed consent was obtained from all participants before the beginning of the study and is available from the corresponding author.
Ethical approval
The protocol of this study is reviewed and approved by the Ethics Committee of Hamadan University of Medical Sciences (no. 9504011608).
Human rights
Our study was done in accordance with the ethical standards of the responsible committee on human experimentation and with the Declaration of Helsinki.