
Abstract
Introduction:
Fulminant myocarditis is uncommon. Making the diagnosis in the emergency department is difficult due to the nonspecific clinical presentation and electrocardiogram results.
Case presentation:
A 58-year-old Chinese woman presented to an emergency department with dizziness and malaise for 2 days. She was hypotensive and afebrile. Initial electrocardiogram showed isolated nonspecific intraventricular conduction delay. Despite resuscitation, she rapidly deteriorated in the emergency department and eventually succumbed. Autopsy and histological examination of heart muscle found acute inflammatory cell infiltration and multifocal necrosis, suggestive of acute fulminant myocarditis.
Discussion:
There is a wide range of differential diagnosis of nonspecific intraventricular conduction delay. Clinical presentation of mycoarditis is also often non-specific. Rapid and accurate recognition of the condition is essential to save life.
Conclusion:
Fulminant myocarditis presenting with cardiogenic shock and isolated intraventricular conduction delay on electrocardiogram poses a diagnostic challenge as illustrated in this case report.
Introduction
Acute myocarditis is an inflammatory disease of myocardium with notoriously variable clinical presentations. 1 Patients often present with nonspecific symptoms. There are usually no telltale signs on physical examinations. Electrocardiogram (ECG) findings may mimic other diseases such as myocardial infarction. These factors pose serious diagnostic and therapeutic challenge to emergency physicians when the patient’s clinical condition rapidly deteriorates.
Here we present a case of fulminant myocarditis in which the diagnosis is missed with a challenging ECG. The patient eventually died during her short stay in the emergency department.
Case presentation
A 58-year-old Chinese woman with good past health attended the emergency department with malaise, dizziness, and chills for 2 days. She denied any chest pain or shortness of breath. She has been self-medicating with an unidentified proprietary medicine.
She was fully conscious at triage. Her blood pressure was 93/43 mmHg and pulse rate was 115 beats per minute. Her body temperature was 36.5°C. Chest and abdominal examinations were unremarkable. Heart sounds were normal without murmur. Urine rapid immunoassay toxicology kit detected morphine and opioid only. ECG was ordered at triage (Image 1).
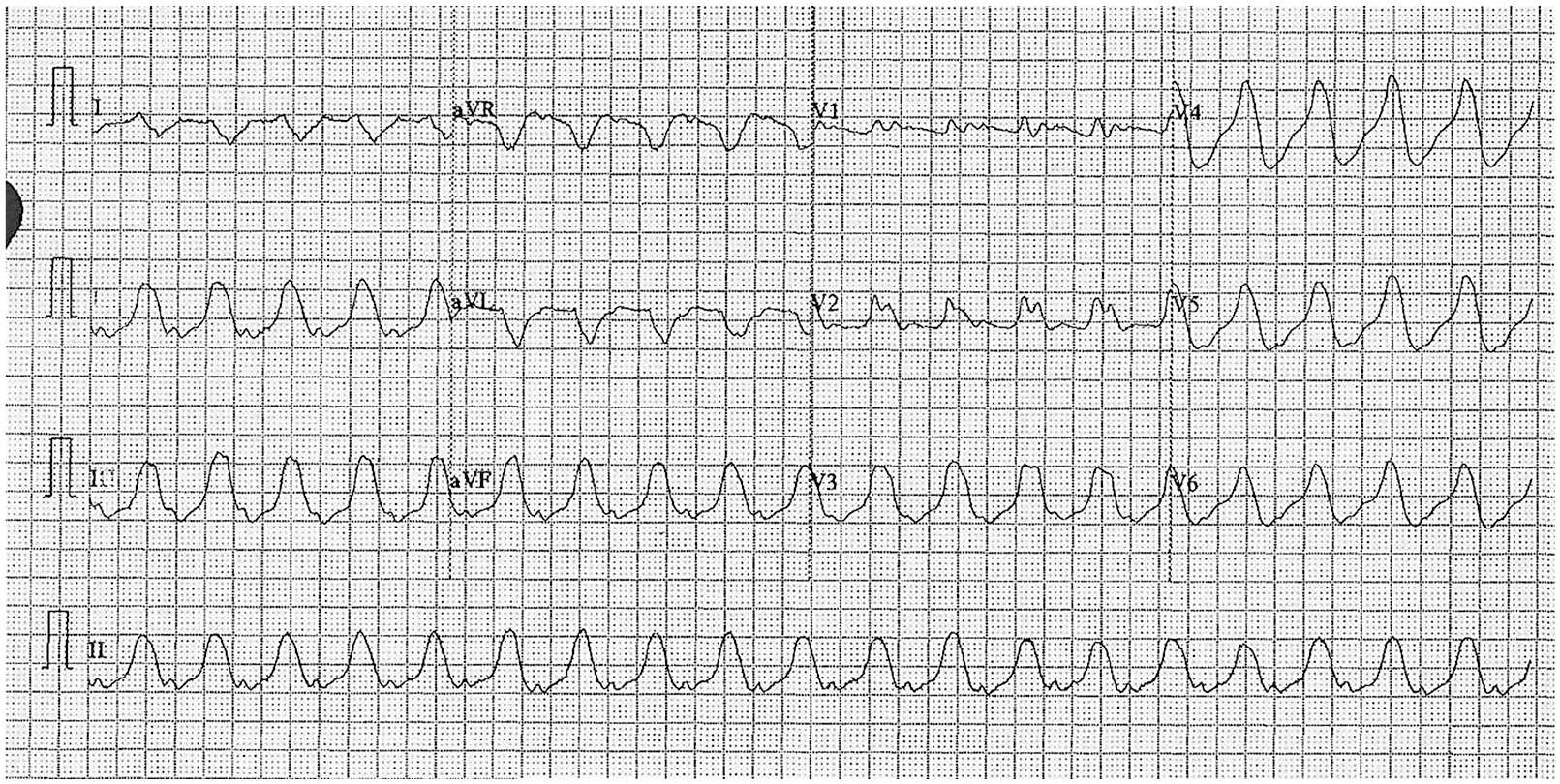
Triage ECG.
Her 12-lead ECG showed a sinus, wide QRS complex rhythm, with ventricular rate at 125 beats per minute. It has an inferior axis at +90°. P waves have a normal duration and form. They are followed by prolonged PR intervals (240 ms) and markedly widened QRS complexes (240 ms). The morphology of widened QRS complexes does not match with any bundle branch block or fascicular block pattern, suggestive of nonspecific intraventricular conduction delay (IVCD). There was no right axis deviation of the terminal QRS in aVR which if present, it would be suggestive of sodium-channel blocker toxicity.
The patient was under close cardiac monitoring in resuscitation room immediately after the ECG. She remained in hypotension despite fluid resuscitation with normal saline. Hyperkalemia and sodium-channel blocker toxicity were initially considered by the case physician as differential diagnosis based on the widened QRS complexes on her ECG and history of self medication. Treatment trials with intravenous calcium gluconate and sodium bicarbonate were given, but she remained in shock. Intensive care physician was urgently consulted. At this juncture, long lead II ECG strip showed wide complex tachycardia without obvious P wave (Image 2); in view of patient’s unstable condition, ventricular tachycardia was considered and synchro-nised cardioversion was performed. Right afterwards, she went into ventricular fibrillation. Defibrillation was performed immediately and sinus rhythm was restored. Chest X-ray showed clear lung fields with normal cardiac silhouette (Image 3). Another electrical cardioversion was performed for unstable wide complex tachycardia, and the patient was in cardiac arrest again. Laboratory results coming back during resuscitation showed that she had a normal serum potassium level (4 mmol/L) and a markedly raised hypersensitive troponin-I level (291,405 ng/L). Resuscitation was terminated 74 min after the second cardiac arrest, only 150 min after attending the hospital.
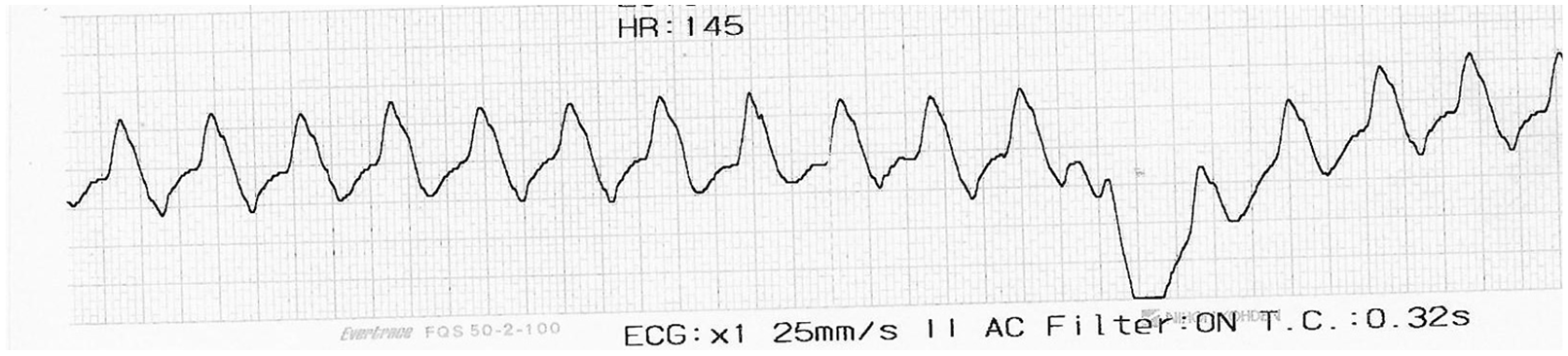
Long lead II ECG strip.
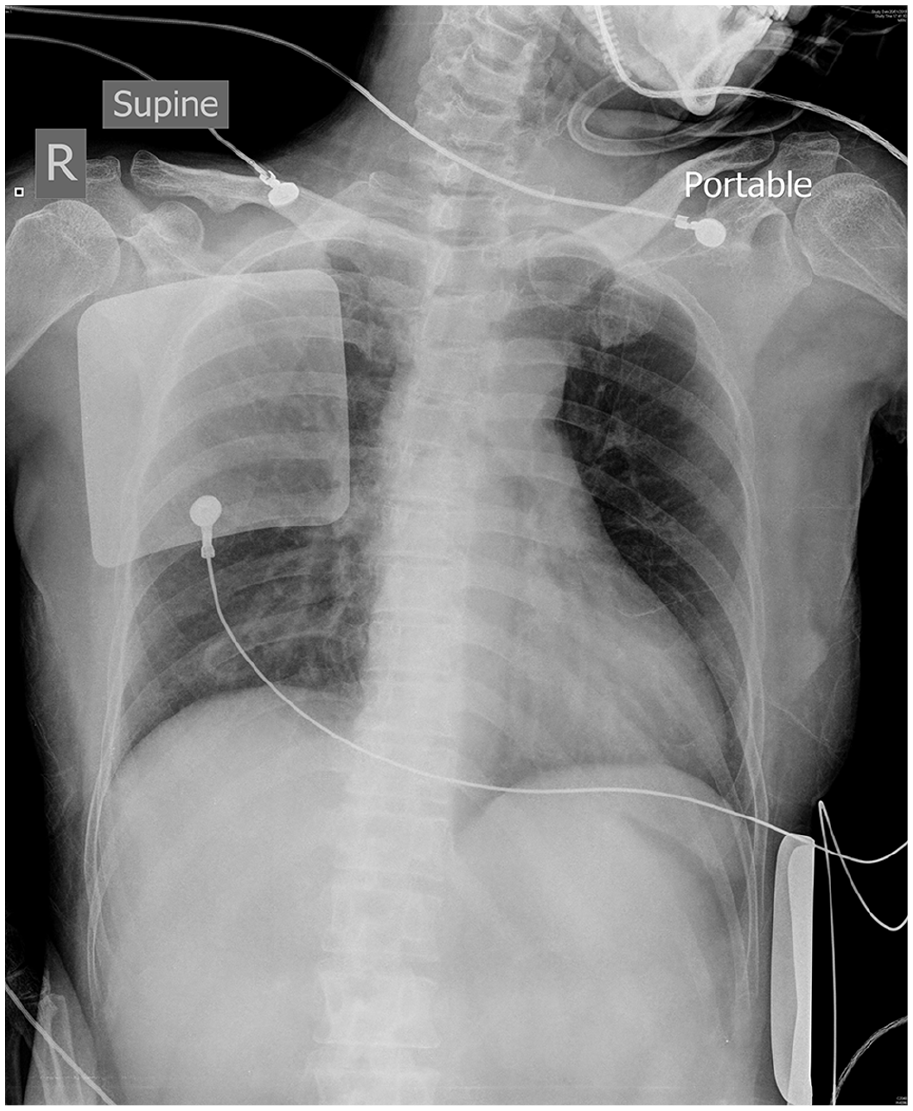
Chest X-ray.
In autopsy, histological examination of cardiac muscles showed acute inflammatory cell infiltration involving most parts of heart muscles, with multi-focal muscle necrosis that was not bound by territorial distribution. Coronary vessels did not show significant stenosis or thrombosis. The overall picture was suggestive of acute fulminant myocarditis.
Discussion
This case highlights the wide range of differential diagnosis of IVCD, nonspecific ECG presentation of acute myocarditis and the importance of rapid recognition of the disease. IVCD is defined as the abnormalities in the intraventricular propagation of supraventricular impulses that give rise to widened QRS complexes. 2 In its broadest sense, IVCD includes right and left bundle branch block, left anterior and posterior fascicular block, Wolff–Parkinson–White pattern and nonspecific IVCD. Sometimes, the term may be referring only to QRS complexes that are wide but do not have a classical bundle branch block morphology. It is important for emergency physicians to recognise this pattern because in extreme case, IVCD with tachycardia can be misidentified as ventricular tachycardia.
Hyperkalemia and sodium-channel blocker can give rise to widened QRS complexes as well. Hyperkalemia inactivates sodium channels in the myocardial cell membrane by persistent depolarization of cell membrane, and sodium-channel blocker directly inhibits the channels. Both result in a decrement of inward sodium current and a decreased rate of rise of phase 0 of action potential. Impulse conduction through the myocardium is slowed down and membrane depolarization is prolonged; as a result, the QRS complexes are widened.3,4 The two conditions can be life-threatening and have to be ruled out when a patient is haemodynamically unstable and presented with an ECG with widened QRS complexes.5,6
Acute myocarditis is an inflammatory disease of myocarditis. Viral infection is the commonest cause, but it can also be due to bacteria, protozoa and systemic diseases such as systemic lupus erythematosus. Fulminant myocarditis is a specific form of acute myocarditis with distinctive clinical profiles. It composes only about 10% of the cases of myocarditis with heart failure. 1 Patients may present with life-threatening arrhythmia, cardiogenic shock or sudden death. Their early ECGs are often nonspecific, with ST segment and T-wave changes which may mimic acute myocardial infarction and pericarditis. 7
Isolated nonspecific IVCD on the presenting ECG in fulminant myocarditis is uncommonly reported in literature. In a descriptive case series of 41 patients with acute myocarditis diagnosed by magnetic resonance imaging, only one patient’s ECG was found to have IVCD but it also had ST segment change. 8 In another retrospective analysis of patients with fulminant myocarditis, ST elevation with wide QRS complex (50%) and complete atrioventricular block (11%) are the commonest findings on their ECG. The presence of a wide QRS complex has been associated with a poorer prognosis. 1
Diagnosis of fulminant myocarditis is difficult by emergency physicians during the patient’s short stay, but rapid and aggressive supportive treatment can potentially save the patient’s life. Once cardiogenic shock is recognised with a grossly abnormal ECG, cardiologist and intensivist should be urgently consulted as in our case. Emergency physicians should equip themselves with skill of point-of-care ultrasonography; adopting Rapid Ultrasound for Shock and Hypotension (RUSH) protocol aids in the confirmation of cardiogenic shock by looking for features including poor cardiac contractility, non-collapsing inferior vena cava and lung rockets. 1 Aggressive haemodynamic support with positive inotropes, intra-aortic balloon pump or veno-arterial extracorporeal cardiac membrane oxygenation provides first-line mechanical circulatory rescue to critically ill patients. 9 All patients should be admitted into an intensive or cardiovascular care unit for close monitoring and management.
Conclusion
In summary, this case report illustrates the diagnostic challenge of fulminant myocarditis in which the patient has a non-specific presentation and an alarming ECG. Emergency physicians should recognise the diagnosis as a life-threatening but potentially salvageable cause of arrhythmia and hypotension.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Informed consent
We were unable to obtain consent from the patient due to rapid deterioration of her condition and death. The article is anonymised and there is no unique identifying characteristic included.
Ethical approval
This case report does not require ethical approval as it is not a human or animal research.
Human rights
This case report does not require human right permissions.