
Abstract
Background:
Ischemic stroke is a leading cause of death and functional disability worldwide. Several clinical scores or stroke scales, biological test or markers, clinical signs, and radiological imaging have been performed to predict both worse neurologic outcome and mortality for ischemic stroke.
Objectives:
The aim of our study was to investigate the association between early Bispectral Index scores and in-hospital mortality in patients with ischemic stroke.
Methods:
This is a comparative prospective methodological study, in which we evaluated the predictive accuracies of Bispectral Index, Glasgow Coma Scale, and Charlson Comorbidity Index for in-hospital mortality of patients with ischemic stroke. Receiver operating characteristic analysis was used for comparing the accuracy of the scoring systems, areas under receiver operating characteristic curves were calculated, and Youden J index was used for estimating associated cut-off values.
Results:
Among the 80 ischemic stroke patients, in-hospital mortality rate was 38.8% (n = 31). The areas under receiver operating characteristic curves were 0.984, 0.960, and 0.863 for Bispectral Index, Glasgow Coma Scale, and Charlson Comorbidity Index, respectively. The difference between areas under receiver operating characteristic curves for Bispectral Index and Glasgow Coma Scale was statistically similar. Besides, the difference between areas under receiver operating characteristic curves for Bispectral Index and Charlson Comorbidity Index, and the difference between areas under receiver operating characteristic curves for Glasgow Coma Scale and Charlson Comorbidity Index were statistically significant. The associated cut-off values were ⩽74, ⩽12, and >4 for Bispectral Index, Glasgow Coma Scale, and Charlson Comorbidity Index, respectively. For these cut-off points, sensitivity and specificity of Bispectral Index were 93.6% and 95.9%, sensitivity and specificity of Glasgow Coma Scale were 100.0% and 83.7%, and sensitivity and specificity of Charlson Comorbidity Index were 83.9% and 69.4%, respectively. However, accuracy of Bispectral Index was 95.0%, accuracy of Glasgow Coma Scale was 90.0%, and accuracy of Charlson Comorbidity Index was 75.0.
Conclusion:
Knowledge of the risk factors for mortality in patients with ischemic stroke can help to identify which patients have a higher risk of fatal outcome. The Bispectral Index score improved discrimination and classified patients with higher mortality better than both Glasgow Coma Scale and Charlson Comorbidity Index.
Keywords
Introduction
Stroke is a leading cause of permanent disability and death worldwide, and presumably the incidence rates in the future are to be sustained or even rise due to the aging of the population. 1 Ischemic stroke (IS) is classically characterized as an episode of neurological dysfunction caused by focal cerebral infarction, and approximately 690,000 adults in the United States experience an IS each year.2,3 The mortality rate of the IS, ranging from 3.7% to 35%, depends on the characteristics of the studied population such as patient’s age and their comorbid condition. 4 In addition, up to 42% of the survivors show severe neurologic deficit for the rest of their life. 5
Stroke patients usually enter the hospital at the emergency department (ED) and their first examinations are performed at ED in collaboration with other departments as needed.6,7 It is critically important for predicting whether the patients develop worse neurological outcome and have higher risk of death after clinical diagnosis of IS. The early detection of patients with high risk may provide the implementation of early effective treatment and that can help decreasing morbidity and mortality rate. 8 It also improves the effective communication between health care workers and patients or their relatives concerning short- and long-term influences of IS. 4
Several clinical scores or stroke scales, biological test or markers, clinical signs, and radiological imaging have been performed to predict both worse neurologic outcome and death in ED, neurology, and intensive care units.4,8 However, some of them are requiring complex laboratory infrastructure such as new biologic markers,1,8,9 and some have moderate sensitivity. 8
The Bispectral Index (BIS) is a processed electroencephalogram (EEG) parameter with extensive validation and has been widely used in the operating room as a way to measure the hypnotic effects of drugs.10,11 However, the use of BIS has been broadened to measure the level of consciousness in neurosurgical patients who have experienced head trauma and other patients suspected of cortical damage due to metabolic or systemic disorders.11–13 A lot of clinical research exhibited that BIS monitoring could be a useful predictive indicator related to worse neurological outcome and death in patients with brain injury and in comatose patients after cardiac arrest or performed severe surgical intervention.7, 10–19 However, there were very few studies particularly investigating the predictive role of BIS scoring for mortality in patients with IS.20,21
The aim of the present study was to observe the relationship between early BIS monitoring and mortality in IS patients in the ED. The potential role of BIS in predicting the prognosis of patients was also investigated by comparing the other prognostic models such as Glasgow Coma Scale (GCS) and Charlson Comorbidity Index (CCI).
Material and method
Study design and setting
This study was a prospective methodological study, in which we compared the predictive accuracies of the BIS, GCS, and CCI for in-hospital mortality in patients with IS. We informed all patients or patients’ relatives about the study procedures, and obtained informed consents on paper from them before their inclusion in the study. We performed this study in accordance with Good Clinical Practice standards, and also according to the Standards for the Reporting of Diagnostic accuracy studies (STARD). 22 After we obtained the ethical approval from the Ataturk University Faculty of Medicine Ethics Committee, we carried out the study between 1 and 31 May 2019 at Ataturk University Research Hospital which is a tertiary care regional hospital with a stroke center.
Patients
Patients who admitted to our ED were evaluated for eligibility. The single inclusion criterion of the study was admission to the ED with stroke. The exclusion criteria were (1) pregnancy, (2) hemorrhagic stroke, (3) having microvascular ischemic lesion, and (4) treated with thrombolytic agents before admission to our ED. Except these patients, others who were admitted with IS to our ED were included in the study. We defined the microvascular ischemic lesion as the lesion up to 2-cm diameter on computerized tomography or magnetic resonance imaging. We used the guidelines of American Stroke Association for the definitions, diagnosis, and treatment of the patients.2,3
We recorded age, sex, smoking status, comorbid diseases, vital signs, symptoms, clinical findings, and length of the stay of the patients included in the study.
Test methods
BIS is a neuromonitoring index that is ranging continuously from 0 to 100, 0 represents isoelectric EEG and 100 represents fully awake state. BIS was monitored with an electrode that was placed on the forehead of the patients according to the manufacturer guidelines (Medtronic, Minneapolis, MN, USA). The values were monitored for 10 min following admission to ED without effecting the medical treatment, and the 10th-min value was recorded for all patients.
We calculated the GCS score evaluating all components of the scale (eye, verbal, motor) for all patients at the admission to ED. We recorded the total GCS score ranging from values of 3 to 15. 23 We also collected the data about the components of the CCI, and calculated the CCI score for all patients in accordance with the original scoring system established by Charlson et al. 24
The reference standard of the study was the in-hospital mortality. We defined it as a death of the patient from any cause during the hospital stay.
Analysis
Statistical analyses were performed with SPSS version 23 (IBM Corp. in Armonk, NY) and MedCalc version 16 (MedCalc Software bvba, Ostend, Belgium). Descriptive statistics were presented as the median with interquartile range (IQR) for non-normally distributed data, and as frequency (n) and percentage (%) for categorical data. Receiver operating characteristic (ROC) analysis was used for comparing the predictive accuracies of BIS, GCS, and CCI scores for in-hospital mortality. Areas under ROC curves (AUCs) were calculated, and DeLong et al. 25 method was used. Youden J index was used for estimating best cut-off values. Sensitivity, specificity, positive likelihood ratio (+LR), negative LR (–LR) with 95% confidence intervals (CIs), and accuracy were calculated; p < 0.05 was set as statistically significance level.
Results
Patients
Between 01 and 31 May 2019, 9988 patients admitted to our ED, 9892 were excluded (9866 didn’t meet inclusion criteria, 21 received thrombolytic therapy, met exclusion criteria, 5 withdrew from the study), and 96 patients were pre-diagnosed with stroke. BIS, GCS, and CCI scores were calculated for all these patients (n = 96), and then, 16 were excluded (13 had hemorrhagic stroke, 3 had microvascular ischemic lesions) after they were evaluated with radiologic examination for differential diagnosis. There has been no loss to follow-up, and finally 80 patients were analyzed for in-hospital mortality (Figure 1).
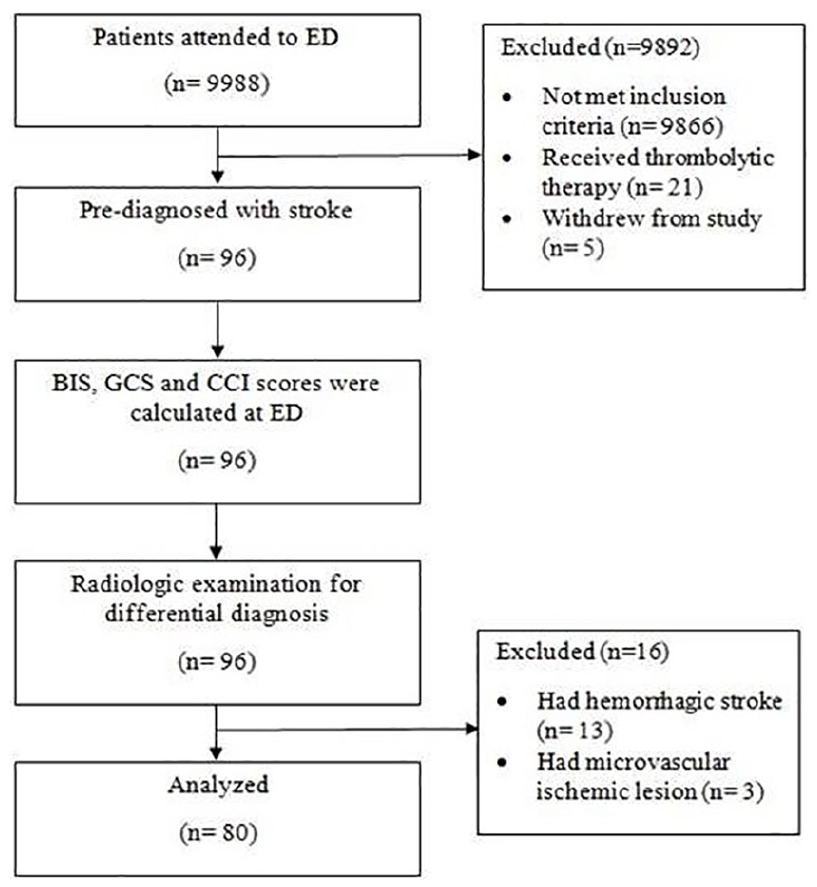
Flow diagram of the study.
Of the patients who were included, median age was 74.0 years, half of them were female, and none of them were smokers. Most prevalent comorbid diseases were hypertension, diabetes mellitus, cerebrovascular disease in medical history, and hyperlipidemia. Among the arrival examinations, median body temperature was 36.9°C, median heart rate was 78 beats per minute, median systolic blood pressure was 183.0 mm Hg, median diastolic blood pressure was 88.0 mm Hg, and median oxygen saturation was 96.0%. The most common presenting symptoms and findings were loss of strength in extremities, speech disorders, deviation of mouth and syncope, respectively. The median of the time elapsed between onset of the symptoms and admission to the ED was 3.5 h. The in-hospital mortality rate was 38.8% (n = 31) with a median length of stay of 11 days (Table 1). The median BIS score was 85.5 (IQR: 68.5–91.0), the median GCS score was 13.5 (IQR: 10.0–15.0), and the median CCI score was 5 (IQR: 4–6) (Table 1 and Figure 2).
Demographics and clinical features of the patients.
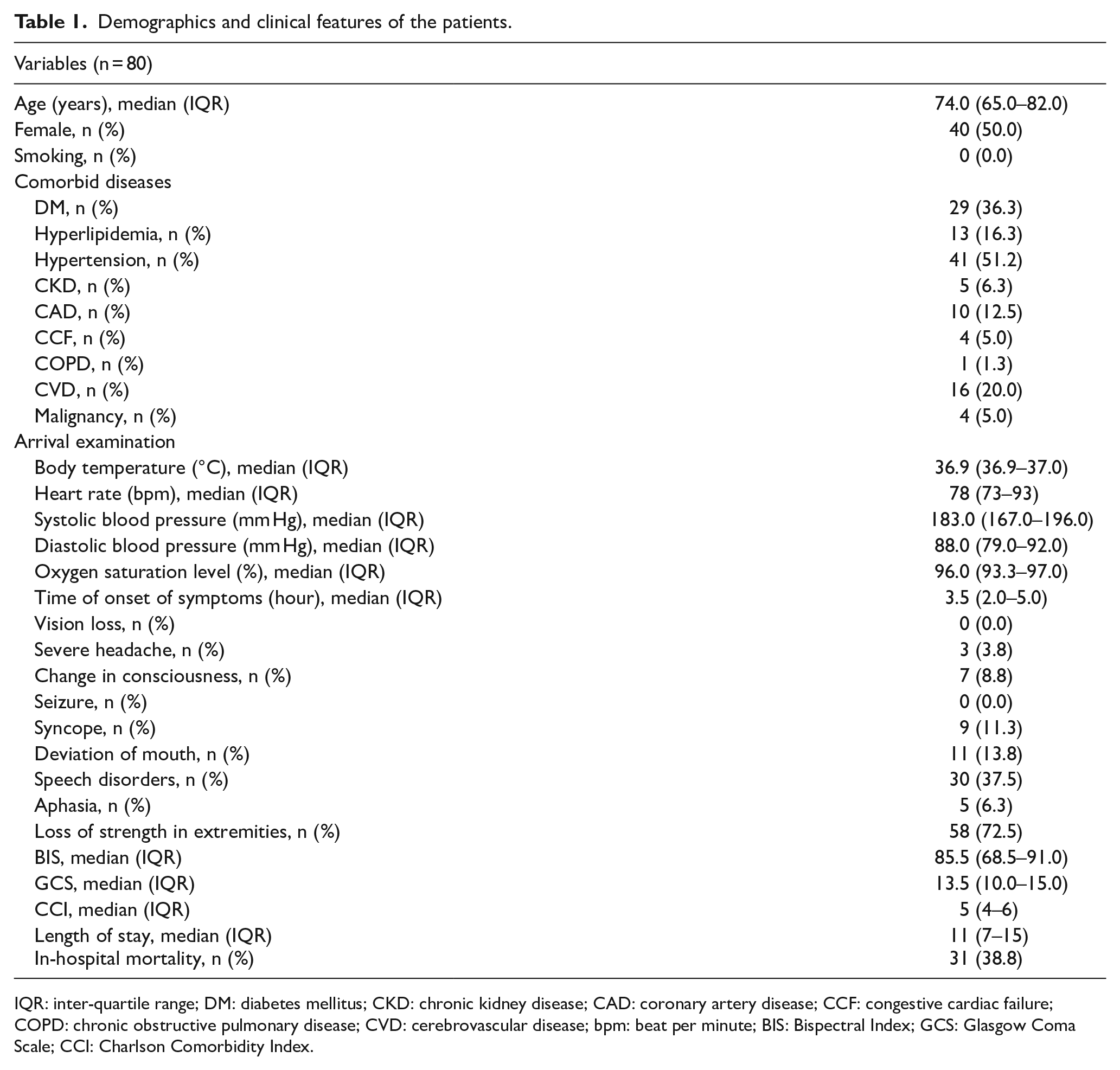
IQR: inter-quartile range; DM: diabetes mellitus; CKD: chronic kidney disease; CAD: coronary artery disease; CCF: congestive cardiac failure; COPD: chronic obstructive pulmonary disease; CVD: cerebrovascular disease; bpm: beat per minute; BIS: Bispectral Index; GCS: Glasgow Coma Scale; CCI: Charlson Comorbidity Index.
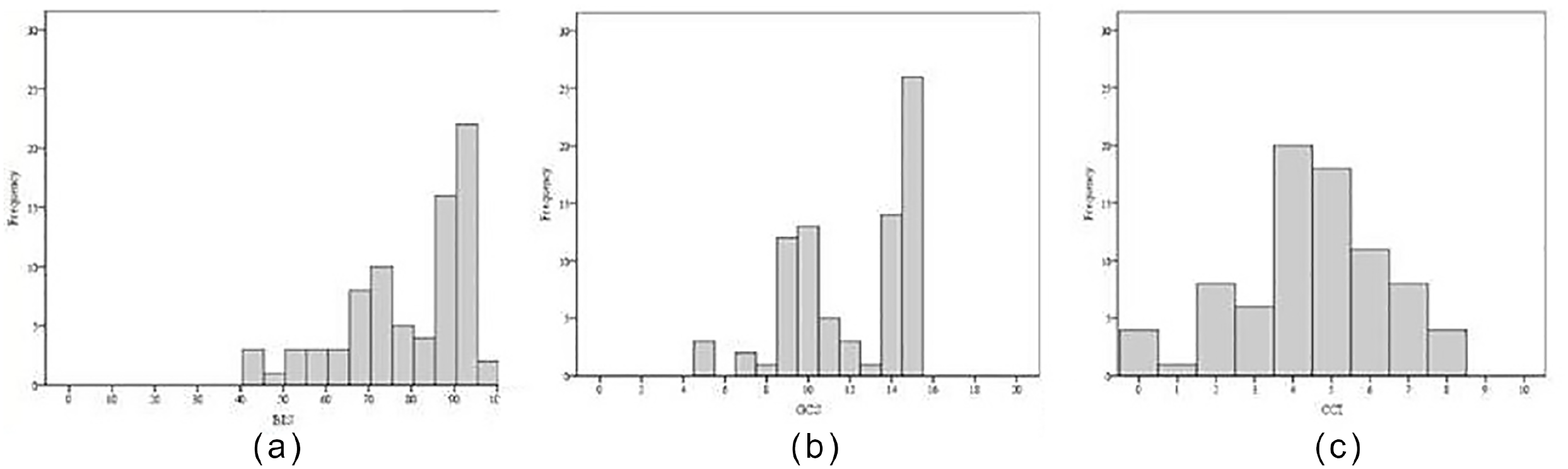
Distributions of (a) BIS, (b) GCS, and (c) CCI data.
Test results
The AUCs were 0.984, 0.960, and 0.863 for BIS, GCS, and CCI, respectively. The difference between AUCs for BIS and GCS was statistically similar. On the contrary, the difference between AUCs for BIS and CCI, and the difference between AUCs for GCS and CCI were statistically significant (p = 0.002 and p = 0.026, respectively). The best cut-off point for BIS, GCS, and CCI, estimated by Youden J indexes (0.985, 0.837, and 0.533, respectively) were ⩽74, ⩽12, and >4, respectively (Figure 3 and Table 2).
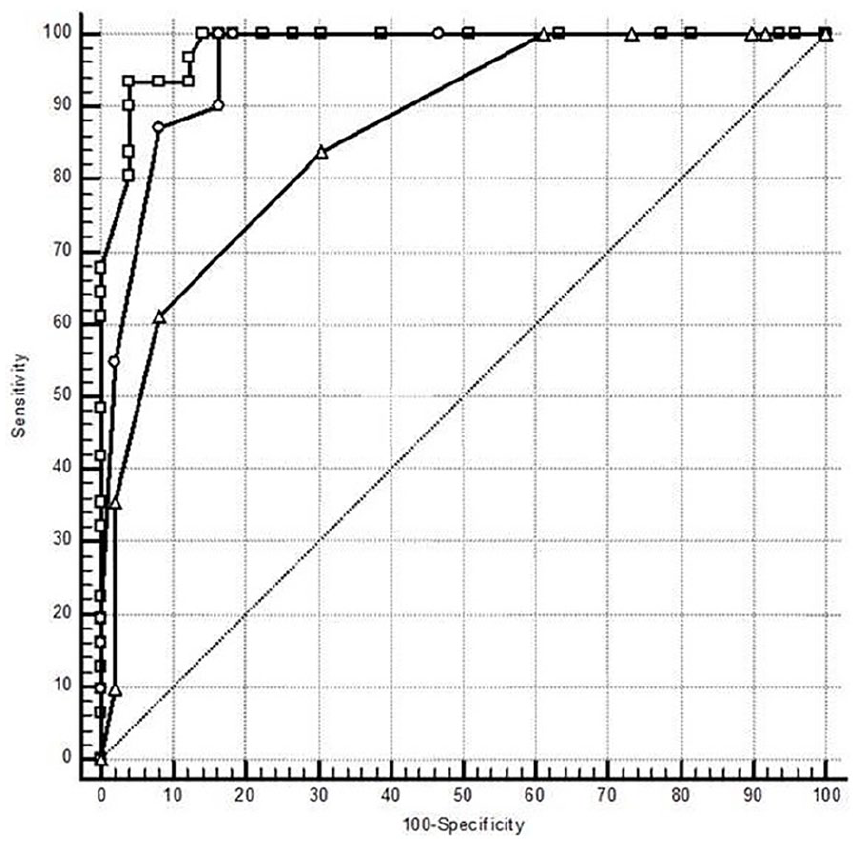
Comparison of ROC curves of BIS, GCS, and CCI data.
Comparison of AUC of the ROC curves of BIS, GCS, and CCI data.
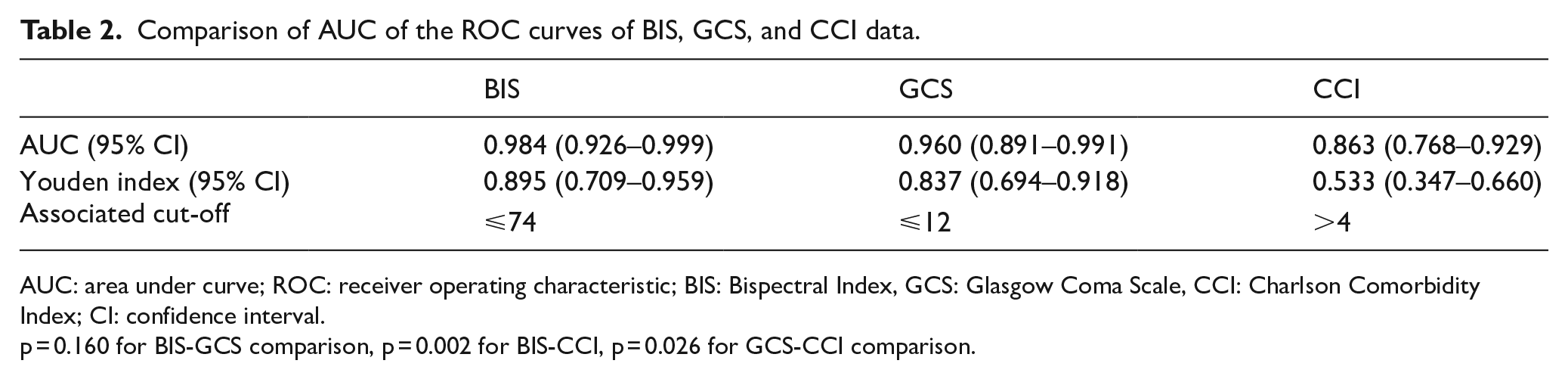
AUC: area under curve; ROC: receiver operating characteristic; BIS: Bispectral Index, GCS: Glasgow Coma Scale, CCI: Charlson Comorbidity Index; CI: confidence interval.
p = 0.160 for BIS-GCS comparison, p = 0.002 for BIS-CCI, p = 0.026 for GCS-CCI comparison.
For the associated cut-off values, sensitivity and specificity of BIS were 93.6% and 95.9%, respectively; sensitivity and specificity of GCS were 100.0% and 83.7%, respectively; and sensitivity and specificity of CCI were 83.9% and 69.4%, respectively. However, the accuracy of BIS was 95.0% with a +LR of 22.9 and a –LR of 0.07, the accuracy of GCS was 90.0% with a +LR of 6.1 and a zero –LR, and the accuracy of CCI was 75.0% with a +LR of 2.7 and a –LR of 0.23 (Table 3).
Cross-tabulation of BIS, GCS, and CCI results by the occurrence of in-hospital mortality.
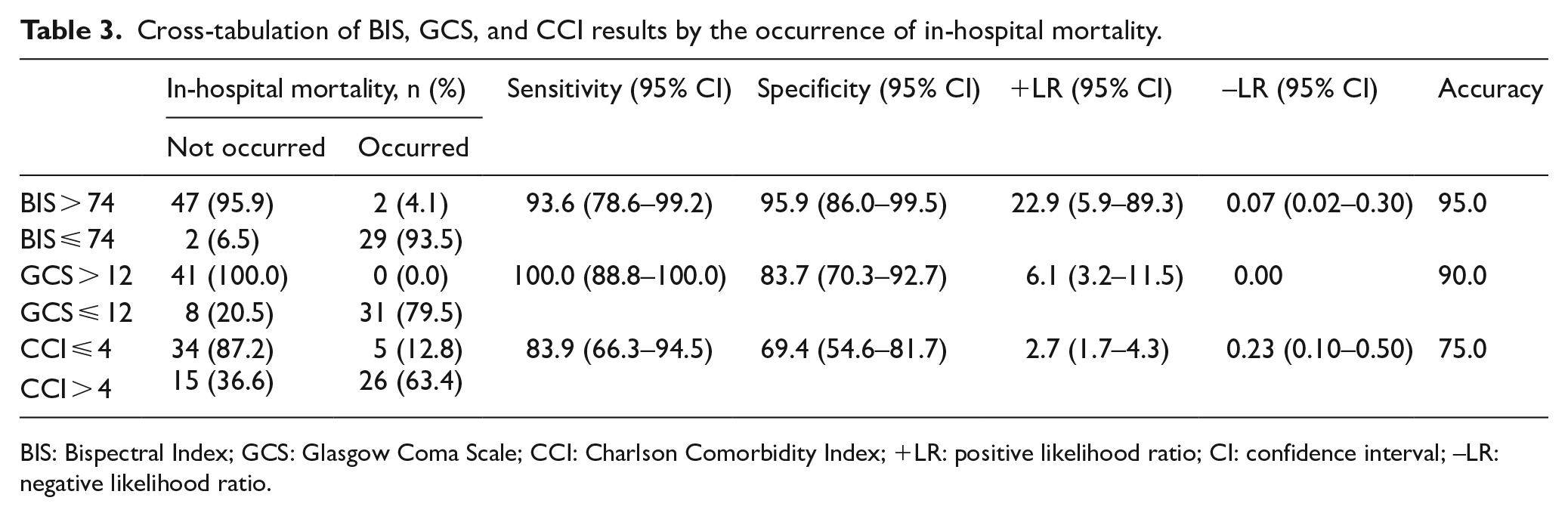
BIS: Bispectral Index; GCS: Glasgow Coma Scale; CCI: Charlson Comorbidity Index; +LR: positive likelihood ratio; CI: confidence interval; –LR: negative likelihood ratio.
Discussion
There were a lot of studies in the literature designed to investigate the correlation between BIS scores and the neurological outcome, morbidity, and mortality in brain injured or other comatose patients including brain trauma, cerebral hemorrhage, and cardiac arrest. 11 Although IS patients were included to the general patient groups in several studies, the sub-group analyses for the IS patients were not performed in those studies.16,18 As of our review of the literature, probably this is the first study designed to investigate predictive role of early BIS scoring for mortality only in patients with IS admitted to ED.
The presented study shows that a BIS value, measured for a short period of time after the admission of ED, is correlated with the prognosis. We identified a cut of point of 74 for BIS estimated by Youden J indexes and BIS value <74 was significantly associated with in-hospital mortality. Also, the predictive performance of early BIS scoring is higher than GCS score and CCI. In a recent study, Miao et al. demonstrated a similar BIS value associated with high mortality. They reported that the recorded maximum BIS scores ⩽71.5 were related to the high risk of mortality during follow-up in patients with hypoxic ischemic encephalopathy after resuscitation. 26
BIS monitoring was first used to assess the hypnotic effects of general anesthetics and sedatives. 27 BIS score ranges from 0 (equivalent to EEG silence) to 100. BIS values 65–85 are recommended for sedation, whereas values of 40–60 are recommended for general anesthesia. 10 After that, the association between BIS index and the depth of coma had been studied in head injured or other comatose patients.12,28 And finally, a lot of researchers have investigated the predictive performances of BIS scoring for neurological outcome or mortality in different clinical conditions such as after brain injury and other comatose patients in the last decades.10,15–17,21,29,30 Dou et al. 10 found that BIS values >42.5 were correlated with the prognosis of comatose patients in ICU. Fabregas et al. 16 studied a model relating BIS to the probability of recovery of consciousness in patients with severe brain injury. They found that the patients with BIS values >52.25 and with BIS values >69.0 have a probability of recovering consciousness higher than 0.5 and 0.9, respectively. Myles et al. 21 studied prediction of neurological outcome using BIS monitoring in patients with severe ischemic hypoxic brain injury undergoing emergency surgery. They demonstrated that an abnormal BIS trace, defined as either a persistently low BIS and/or electroencephalographic burst suppression not explained by hypnotic drug administration or hypothermia, was strongly associated with poor neurological outcome. In a recent study, the researchers investigated the predictive value of the BIS for the post-operational consciousness recovery and they showed that it might be a potential tool for predicting the consciousness recovery in intracerebral hemorrhage patients undergoing hematoma evacuation. 29
GCS are commonly used to evaluate the patient’s neurological status in ICU. 11 It is also used to prognostic model in patients with brain injury and other comatose clinical conditions in ED.4,7,28 However, it has inherent inter-observer variability and therefore mild changes can be observed in one clinician to another.7,11 BIS is an objective, non-invasive, and repeatable measure of brain function derived from EEG data and converted by mathematical algorithm into a continuous numerical value.31
The IS patients are generally over 65 years of age and always have critical primary diseases such as hypertension, diabetes, cardiogenic and respiratory system disorders, and also have high neurological disability and death.1,26 In the present study, all patients were over 65 years and almost all patients have at least one comorbid condition, their mean CCI was 5. Even then, sensitivity, specificity, and accuracy of BIS score in predicting the prognosis of patients with IS were higher than the GCS and CCI.
A limitation of the study is the small number of patients and that might bias the results. In addition, BIS values were monitored only at the admission in ED and were not continued in present study. Therefore, only one BIS value for each patient was taken into consideration for the performed analysis.
In conclusion, the BIS score improved discrimination and classified patients with higher mortality better than both GCS and CCI, thus our results suggested the significance of BIS and its plausible use in clinical practice to predict stroke outcome. In addition, it is easy to perform, it is transportable, and it represents the data of patients in real time. Careful evaluation of BIS score at admission to ED and interpretation of patient’s BIS score together with clinical signs and existing risk factors can help to generate a conclusion about mortality. This approach also can improve communication between healthcare workers and patient’s relatives by sharing accurate information to their patients at a very early stage. These results should be supported conducting clinical trials in greater populations.
Footnotes
Author contributions
The study concept was made by S.T.A.G, I.A., M.Z.K., and A.O.K.; design—I.A., M.Z.K., A.O.K., and A.E.; supervision—S.T.A.G., A.O.K., A.E., and Z.C.; resources—S.T.A.G., I.A., A.E., and Z.C.; materials—I.A., A.O.K., A.E., and Z.C.; data collection and/or processing—S.T.A.G., I.A., M.Z.K., A.O.K., A.E., and Z.C.; literature search—S.T.A.G., I.A., M.Z.K., and A.O.K.; writing manuscript—S.T.A.G., I.A., M.Z.K., A.O.K., A.E., and Z.C.; critical review—S.T.A.G., I.A., A.O.K., and Z.C.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data were obtained from patients who admitted to Ataturk University Medical Faculty Emergency Department.
Ethical approval
Ethics committee approval was received for this study from the Ethics Committee of Ataturk University Medical Faculty (2019—season number: 4, desicion number: 2).
Human rights
There is no violation of human rights for the article.
Informed consent
An informed consent form was obtained from each patient who consented to join the study.