
Abstract
Background:
Penetrating injury can encompass a large spectrum of injuries dependent on the penetrating object, the location of entry, and the trajectory of the object through the human body. Therefore, the management of penetrating injuries can be challenging and often requires rapid assessment and intervention. No universal definition of penetrating injury exists in the literature and little is known about the demographics and outcome of penetrating injury in the Netherlands.
Objective:
A research was carried out to ascertain the size and outcome of penetrating injuries in two level-one trauma centers in the Netherlands.
Methods:
Using the trauma registry of the Radboud University Medical Center in Nijmegen and VU University Medical Center in Amsterdam, all patients with penetrating injury were identified who were admitted to these level 1 trauma centers in the period between January 1, 2009, and January 1, 2014. Penetrating injury was defined as an injury that caused disruption of the body surface and extended into the underlying tissue or into a body cavity. Data concerning age, gender, mechanism of injury, Glasgow Coma Scale, number of injuries, type of injury, and Injury Severity Score were collected and analyzed. Patient results were stratified by Injury Severity Score.
Results:
In total, 354 patients were identified, making up around 2% of all admitted trauma patients 3.1% (VU Medical Center) and 1.6% (Radboud Medical Center). Patients were overwhelmingly male (83.1%) and median age was 36 years (range = 1–88 years). Most injuries were caused by stabbings (51.1%) followed by shootings (26.3%). Admission to the intensive care unit occurred in 41.1% of all patients. Median stay in the intensive care unit was 5.1 days (range = 1–96 days) and median total hospital stay was 8 days (range = 1–95 days). Mortality among these patients was 7.1%, ranging from 0% among patients with Injury Severity Score 1–8 to 100% in patients with Injury Severity Score > 34. High mortality figures were associated with injuries caused by firearms (19.4%), injuries to the head (27.9%), and alleged assaults (10.9%). Differences in demographics between the two centers were not significant.
Conclusion:
Penetrating injury is a relative rare occurrence in the Netherlands compared with other countries. It is associated with high mortality and substantial hospital costs. The incidence of penetrating injuries is higher in metropolitan areas than in rural areas. A universal definition of penetrating trauma should be agreed upon in order to ensure that future studies remain free of bias, and also to ensure that data remain homogeneous.
Introduction
The management of penetrating injuries can be challenging and often requires rapid assessment and intervention. Penetrating injuries with a high Injury Severity Score (ISS) usually arise from stabbing and shooting wounds. The incidence of such injuries varies according to country and region. In 2014, a total number of 33,594 people died as a result of fipeople injuries in the United States, accounting for 16.8% of all injury deaths that year. 1 In the United Kingdom, 4614 injuries were caused by the use of firearms during the period 2007–2008, and 212 cases of homicide occurred through the use of sharp objects during the period 2005–2006.2,3 The median cost of patients with penetrating trauma in England and Wales was estimated at £7983 (9082 Euros) per patient, compared with blunt trauma at £9530 (10,842 Euros) per patient. In addition, the same study found 1365 patients with penetrating injuries, corresponding to 3.7% of the total number of trauma patients.4,5 A Norwegian study has shown that patients from rural areas (with low-density populations) have a higher prehospital mortality risk than patients from urban areas. The factors proposed to explain this include response time, time and distance of primary transport, the limitation of specialized care in rural areas, and rapid triage. Furthermore, rural municipalities experience more traffic injuries compared with metropolitan areas, where self-harm and assault-related injuries are more common. 6 There are few studies on the epidemiology and outcome of patients with penetrating injuries in the Netherlands. In the Amsterdam area (regio traumanet AMC), 109 cases of penetrating injuries by shooting or stabbing were reported in 2015, accounting for 1.7% of all trauma cases. 7 A study by Lansink et al. 8 reported a 70% increase of patients with penetrating trauma in 2007–2010 compared with 2003–2007, indicating a greater need for adequate care. No mortality figures were given concerning these specific groups. A greater understanding of the etiology and pattern of such injuries can help to improve the management, and ultimately the outcomes, of these patients. This study aims to shed insight into patient outcomes and demographics in both rural (Nijmegen) and urban (Amsterdam) areas of the Netherlands for patients with penetrating injuries.
Methods
The Radboud University Medical Center (Radboudumc) and VU University Medical Center (VUmc) both have a level 1 trauma center and provide supra-regional tertiary care, covering approximately four million inhabitants. Both of these level 1 trauma centers keep an official registry of all patients admitted, using the Abbreviated Injury Score (AIS) Dataset (update 2008) to calculate the ISS. We identified all patients with penetrating injuries admitted during the period between January 1, 2009, and January 1, 2014. We extracted the data from Radboudumc and VUmc hospital databases and retrieved the details of patients admitted for penetrating injury during the abovementioned period. Data on age, gender, injured anatomical areas, injury etiology, number of injuries, ISS, length of stay in the intensive care unit (ICU), and mortality were collected. Injury severity was measured using the ISS. For the grouping of ISS, we used the categories used by Christensen et al.: 4 1–8, 9–15, 16–24, 25–34, and 35–75. The primary outcome was mortality, defined as in-hospital death occurring during the first 30 days after trauma with length of stay as a secondary outcome, stratified for the ISS. 9 Death occurring after 30 days following trauma is more likely to be caused by other conditions. 10 Furthermore, we compared mortality rates between different geographical regions. Spearman’s rank order correlation was used to analyze possible correlations between crime rate, firearm possession, and incidence of penetrating injuries. We reviewed the literature extensively regarding the use of the term penetrating injury, using the Pubmed, Embase, and Cochrane libraries. Most papers on this topic do not give a clear definition of penetrating injury, but rather refer to the data provided by trauma registries.
Penetrating trauma in the literature
In the literature, different terms are used to describe injuries caused by a penetrating object. The most commonly used are penetrating injury, penetrating trauma and wounds, penetrating (medical subject headings). These terms were thus used for the literature search. Sharp injury is another term used by some as opposed to blunt injury. The use of the term sharp injury, however, is problematic, because it is also used to refer to injuries by sharp objects that occur in a healthcare setting. Second, penetrating injury can be caused by objects which are not sharp. For the remainder of the article, we used the term penetrating injury. Although penetrating injury is widely used in the literature, no clear definition exists for the term. One of the first reports to use the term is an article by Ruddock 11 from 1840, in which he describes the case of constable who incurred a stabbing injury. What follows are many articles which can be divided into three groups according to their use of the term penetrating injury. The first group uses a definition of penetrating injury, but only for one specific anatomical region. For example, there is an article by Mutabagani et al. 12 on penetrating injuries to the neck. Another example is penetrating traumatic brain injury, which is defined as traumatic brain injury accompanied by dural penetration. 13 This specific definition is useful for the region mentioned for comparing figures with other data, but cannot be applied to other regions of the body. Furthermore, having a specific definition for each anatomical region would be both complicated and would intensify the collecting and classifying of injuries. The second group of articles consists of studies that gained their data and their distinctions between penetrating and non-penetrating injuries from trauma registries.4,14 The most commonly used databases are the American National Trauma Data Bank (NTDB) and the United Kingdom Trauma Registry (TARN). The last group of articles are studies which use their own hospital data with no definition given of penetrating injury. By glancing through their data, it becomes evident that the vast majority of these articles concern patients with either gunshot or stab wounds.15,16 Other causes of penetrating injury are not included. Although gunshot and stab wounds are responsible for most cases of penetrating injury, there are other causes such as blasts, impalement, and objects penetrating the body during accidents.
With no clear definition to be found in the literature, we were compelled to choose an appropriate definition of penetrating injury. We sought a definition that was logical and could easily be applied in practice. We chose to use the one from Stedman’s Medical Dictionary, which defines penetrating injury as an injury accompanied by disruption of the body surface that extends into the underlying tissue or into a body cavity. Injuries that do not extend to the underlying tissue or body cavity are injuries that are neither severe nor complicated. Wounds caused by animal bites, glass, and saw wounds were excluded from the present study as most studies do not take these into account. Saw wounds and animal bites are wounds that are mainly a combination of tear and penetration. 17
Results
We identified 354 patients with penetrating injuries during the 5-year study period. 259 cases were from the VUmc database and 95 were from the Radboudumc database. This was 3.1% (VUmc) and 1.6% (Radboudumc) of all admitted trauma patients, respectively. 179 patients (50.6%) had an ISS score of 1–8, 81 patients (22.9%) 9–15, 56 patients (15.8%) 15–24, 29 patients (8.2%) 25–34, and nine patients (2.5%) scored 35–75 (Table 1). Patients were predominantly male (83.1%) and the median age was 36 years (range = 1–88 years). The main cause of injury was stabbing (51.1%), followed by shooting (26.3%). The remainder (22.6%) were caused by other types of penetrating injury, mainly accidental. Alleged assaults accounted for 52% of all cases, followed by accidents (33.9%). The remainder (14.1%) were self-inflicted. The most frequently harmed body regions were the limbs (46.9%), thorax (34.7%), and abdomen (31.6%). More than 12% of the patients sustained head injuries. Four spinal injuries were recorded. Almost 61% of the patients showed a single injury, the remainder having more than one injury, and approximately one tenth incurring three or more injuries. The mean number of injuries in the total population was 1.5. The median length of total hospital stay was 8 days (range = 1–95 days), with patients with an ISS of 25–34 having the longest stay (median = 29.4 days) (Table 2). About 41.1% of all patients were admitted to the intensive care unit with a median length of stay of 5.1 days (range = 1–96 days). A trend can be noted that patients with increasing ISS generally have longer spells of hospital care, until they reach an ISS of 35–75. These patients tend to decease within 24 h of hospital admission and therefore have shorter hospital and intensive care unit stays. The overall mortality rate among patients with penetrating injuries is 7.1%, ranging from 0% among patients with ISS 1–8 to 100% in patients with ISS 35–75 (Table 3). Males have a higher mortality rate than females (7.5% vs 5%, respectively). High mortality figures were associated with injuries caused by firearms (19.4%), injuries to the head (27.9%), and alleged assaults (10.9%). Penetrating injuries that were caused by objects other than firearms and knives did not cause any deaths. Injuries to the limbs and abdomen had a very low mortality rate (3.6% and 5.4%, respectively). The most significant causes of death were exsanguination and severe brain injury. In our assessment of the data, the only significant difference was that of the VUmc Medical Center having more than twice the incidence of penetrating trauma than Radboudumc. No other significant differences were found between the two hospitals.
Patient characteristics.
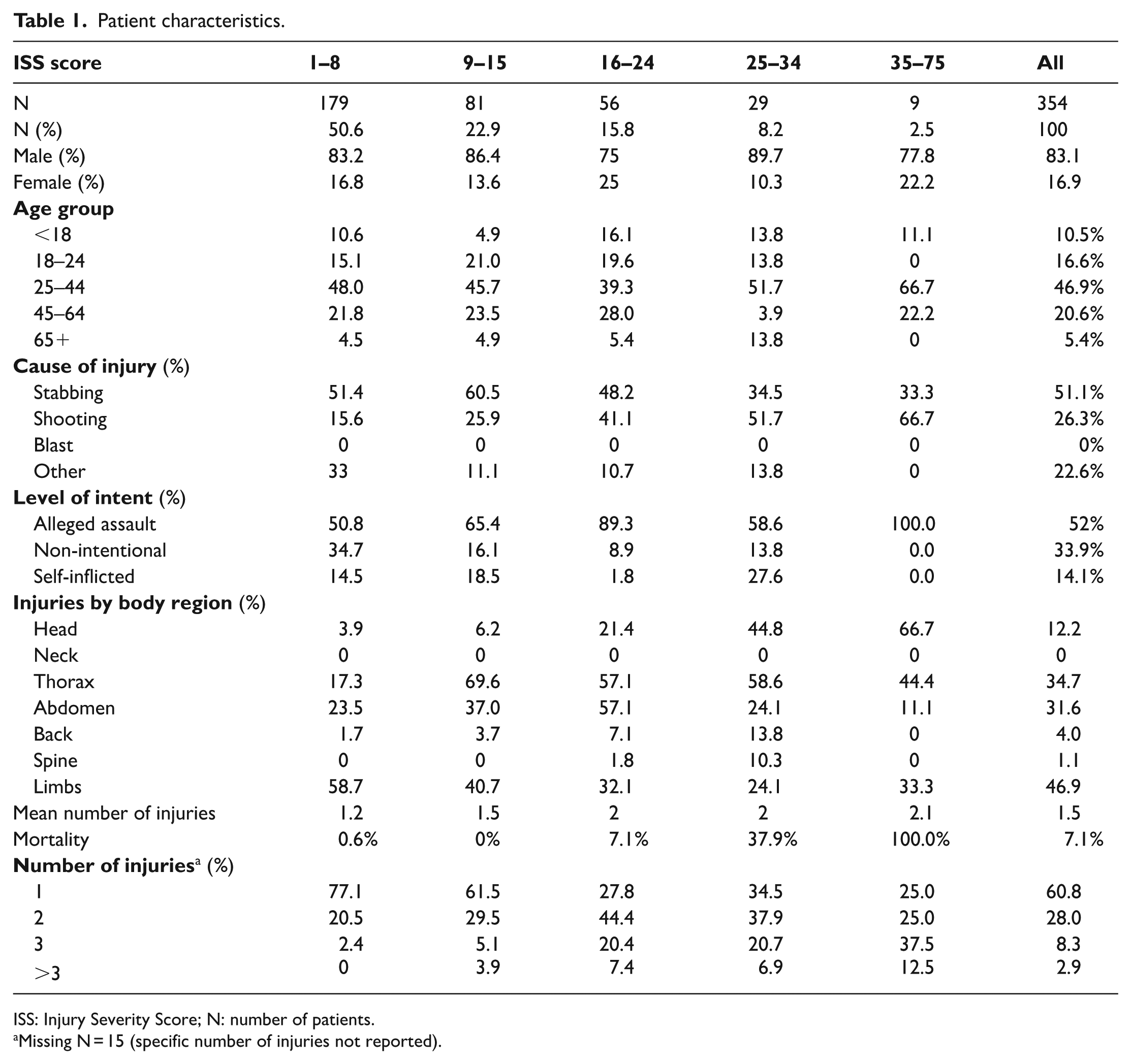
ISS: Injury Severity Score; N: number of patients.
Missing N = 15 (specific number of injuries not reported).
Treatment characteristics.
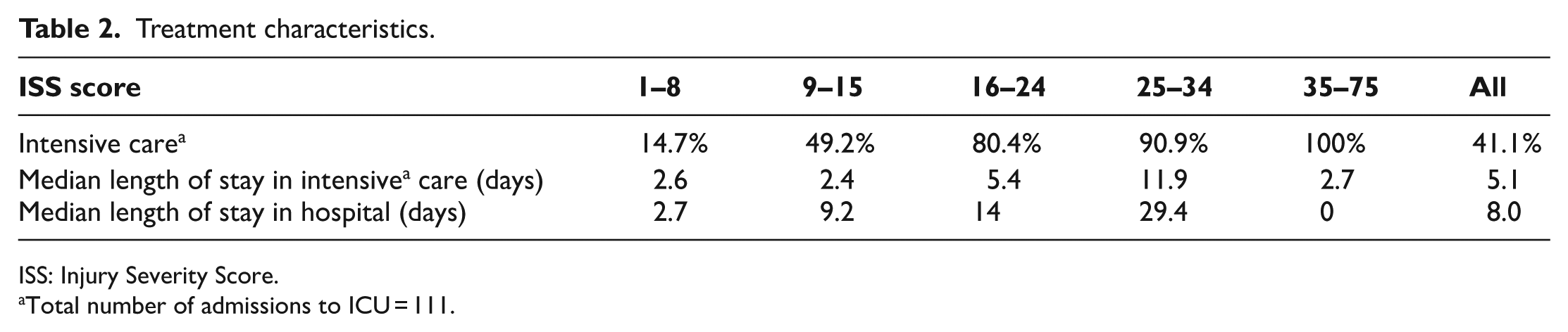
ISS: Injury Severity Score.
Total number of admissions to ICU = 111.
Mortality percentage stratified by ISS score.
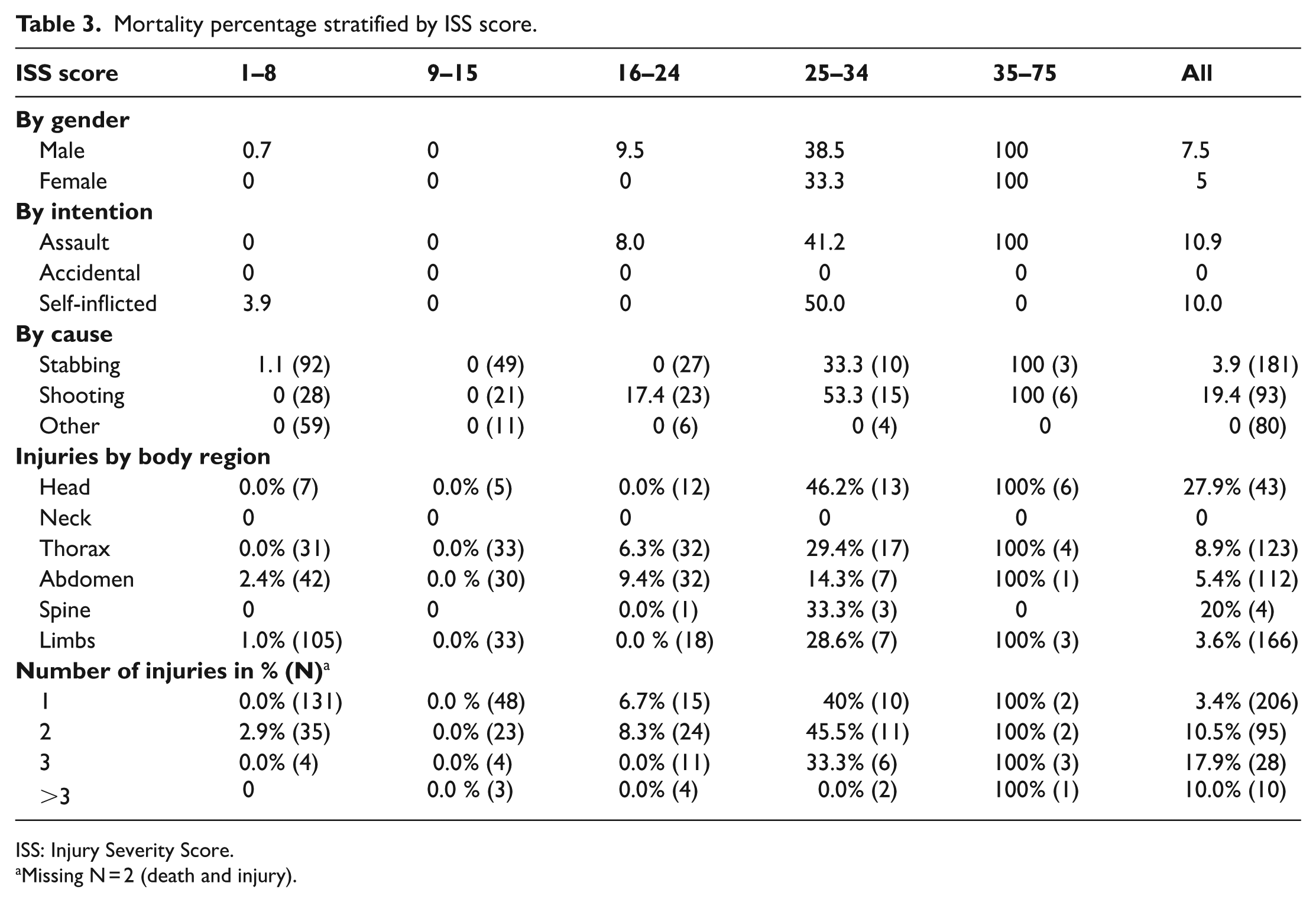
ISS: Injury Severity Score.
Missing N = 2 (death and injury).
We also assessed the correlation between the crime rate and the incidence of penetrating trauma using the available data but found no significant correlation, as shown in Figure 1. This means that the crime rate is not a direct indicator for the prevalence of penetrating injury. Furthermore, the correlation between firearm possession and the incidence of penetrating trauma was assessed and is shown in Figure 2. A statistically significant relationship was found suggesting that with higher rates of gun ownership, the prevalence of penetrating injury rises.
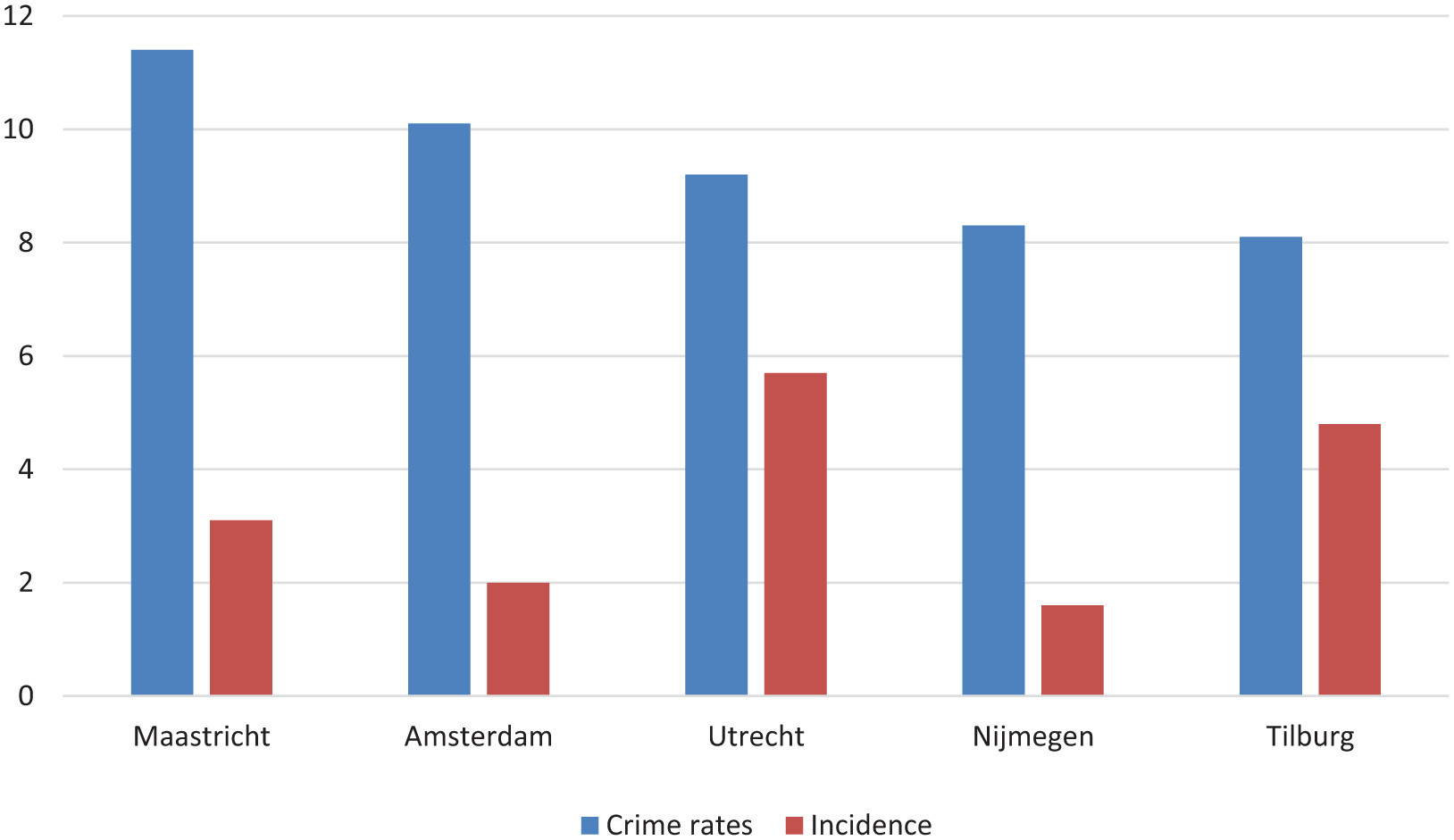
Data concerning the occurrence of crime in the different regions in the Netherlands in relation to the incidence of penetrating injury.8,18–21 No clear correlation can be seen as there are regions with relatively low crime rates but have a higher incidence of penetrating injury compared to regions with higher crime rates. Spearman’s correlation was not significant.
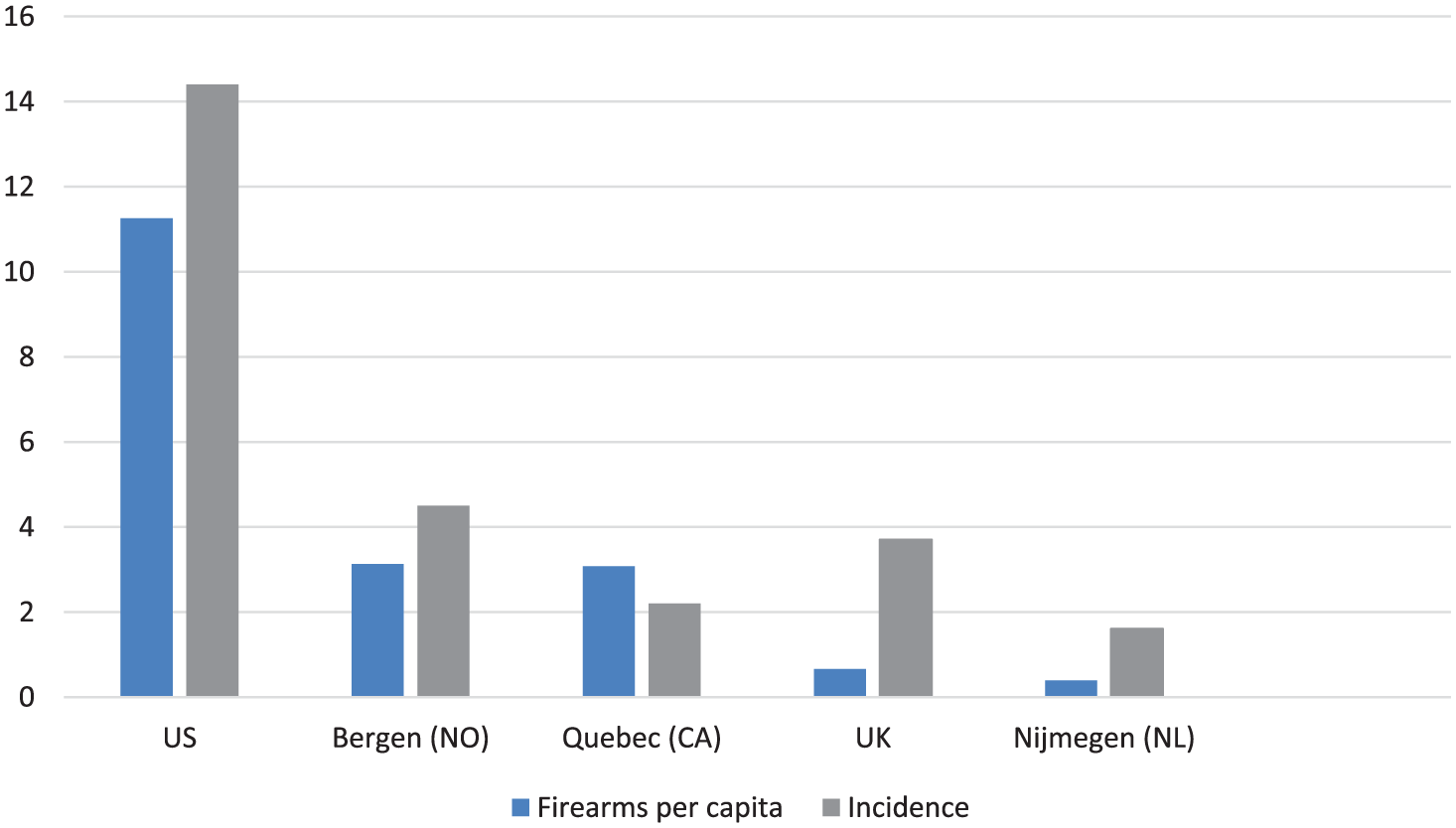
Amount of firearm ownership in different countries related to the incidence of penetrating injury.4,22–24 Spearman’s rank order correlation gives a high correlation, 0.900 with significance at 0.05 level, indicating there is a high correlation between the possession of firearms in a population and the occurrence of penetrating injury.
Discussion
This is one of the first studies to describe the characteristics and outcomes of patients with penetrating injuries in the Netherlands, comparing the data of two large level 1 trauma centers in different geographical areas, urban (VUmc) and rural (Radboudumc). Penetrating injury is a relative rare occurrence in the eastern region of the Netherlands in contrast to the more urbanized western part of the country. Compared with other regions in the world, the incidence of penetrating injury in the Netherlands is limited (see Table 44,8,10,14,18–21,23–31). In addition, the population density and availability of critical medical care in both urban and rural areas varies more throughout the wider world compared with the Netherlands, the latter having a high population density and well-established trauma network in its provinces. After reviewing the existing literature, we conclude that there is no clear definition of penetrating injury. Furthermore, most of the articles found in the literature do not report the data homogeneously. This makes comparing our figures with other national and international data difficult and subject to bias. As we currently have no other means of comparing our figures, it remains worthwhile to use these sources. Comparing national figures with those in the article of Lansink et al., 8 which describes the patient population of a level 1 trauma center in the central Dutch city of Utrecht, in which they were able to identify 303 cases during an 8 year period, accounting for 5.7% of all trauma patients, then these figures are clearly substantially higher than in this study. The percentage difference shows that the difference in absolute numbers of patients with penetrating injuries is not explained by the greater numbers of admitted patients but can be explained either by the increased occurrence of this type of injury, or by the use a different definition of penetrating injury. In another article by Vles et al. 20 concerning trauma care in the southern city of Tilburg during the period 1996 to 1998, the authors found 137 patients with penetrating injury, accounting for 4.8% of all patients. Again, we note the higher absolute and relative numbers when compared with our own figures. As mentioned earlier in a report of the Amsterdam area concerning trauma care, there were 192 cases of penetrating injury in the year 2012, accounting for 3.1% of all trauma cases. 18 A more recent study by Boot et al. 32 which included only penetrating injuries caused by shootings and stabbings, notes a mortality rate of 17% and 3% for injuries from shootings and stabbings, respectively. Our results showed 19.4% and 3.9%, respectively. Although our figures were higher, they are not readily comparable because of the absence of injury severity in the former article. It is difficult to find explanations for the regional differences of penetrating injury in the Netherlands. Explanations should be sought in the differences in crime levels, the availability of weapons, the level of urbanization, and social conditions. No significant correlation could be found, however, between crime rates and the incidence of penetrating injury when comparing different regions in the Netherlands. The possibility exists that certain types of crime are related to penetrating injury, although not crime as a whole. Even with these differences between regions, the occurrence of penetrating trauma in the Netherlands is, in general, relatively low.
Patients with penetrating as % of total trauma patients and mortality.
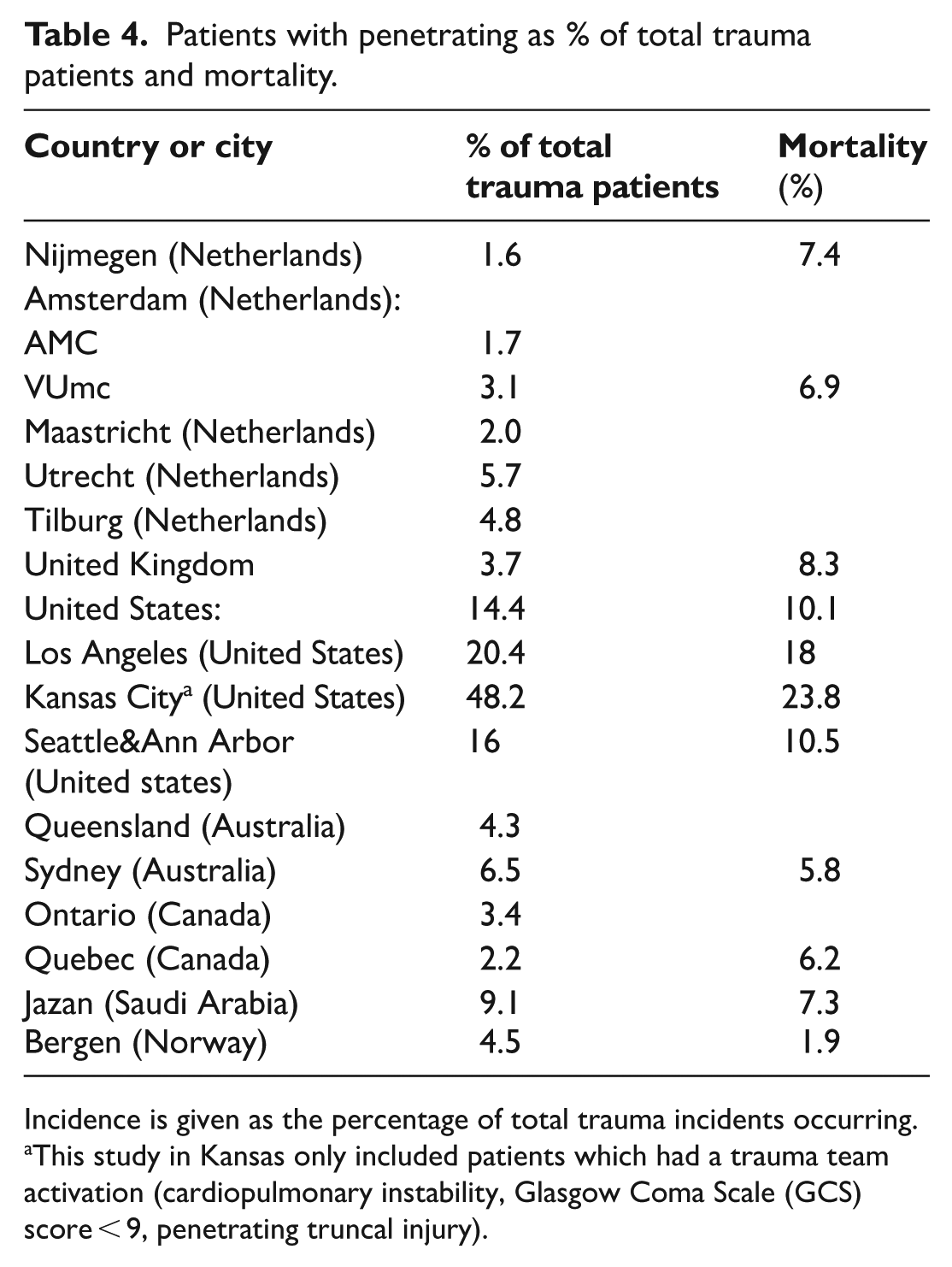
Incidence is given as the percentage of total trauma incidents occurring.
This study in Kansas only included patients which had a trauma team activation (cardiopulmonary instability, Glasgow Coma Scale (GCS) score < 9, penetrating truncal injury).
A study assessing penetrating trauma in England and Wales identified 1365 patients, corresponding to 3.7% of the total number of trauma records. 4 The overall mortality rate of these patients was 8.3%. We have a comparable mortality rate of 7.5%. When examining the data more closely, some interesting similarities and differences can be noted. High mortality rates were related to shooting (11%) and stabbing (9%). We also noticed in our study the same relation but different figures for shootings and stabbings (19.4% and 3.9%, respectively). Regarding hospital stays, the same relation can be seen. Patients with more severe traumas need longer hospital stays unless they have an injury severity likely to be terminal. An important difference is a higher mortality rate for patients with accidental injuries than patients involved in alleged assaults. In our study, we found the opposite. It is unclear why this is not the case in England and Wales. A greater availability of firearms, and thus more accidents with these weapons, is not an explanation. The United Kingdom has 3.78 firearms per 100 citizens, 33 compared with the 3.9 firearms per 100 citizens in the Netherlands. 34 In the United States, we find substantially higher figures. The Los Angeles area, for instance, has an incidence rate of more than 20% of patients with penetrating injury. The same can be said about the mortality rate of 18% (Table 4). These high figures may be explained by the greater availability of weapons, and indeed of higher caliber firearms, as shown earlier in Figure 2. This figure shows an increase in the incidence rate of penetrating injury with increasing gun ownership, the exception being the United Kingdom, where gun ownership is relatively low but where the incidence rate of penetrating injury is high. One reason for this is that a large proportion of the incidents of penetrating injury in the United Kingdom are caused by stabbing. In spite of this, a significant correlation was found between the numbers of firearms and the incidence rate of penetrating injury.
Certain limitations can be noted in our study. It offers a retrospective character, and as such we have noted that some cases were incomplete and sometimes unclear. Second, we rely on data that was not specifically collected for our research, resulting in probable selection bias and, potentially, missing cases. In addition, our patient database consists of two different hospitals and therefore the possible relations between patient and treatment characteristics will be vulnerable to bias. Patients were coded in a similar fashion (using the same Dutch trauma coding system) but by two different centers, meaning that one center might judge a case differently from the other. This could be an explanation for the difference in case size between Radboudumc (95 cases) versus VUmc (259 cases). A larger study including all eleven level-1 trauma centers in the Netherlands might well identify factors important for outcomes, and also for comparing standards of care. Third, and most important, with no clear definition of penetrating trauma in the literature, comparing our results with other studies is a practice fraught with risks and bias. A consensus on a clear definition for this type of injury should be agreed upon by leading trauma organizations. Without comparing, data would be less meaningful.
Conclusion
In summary, penetrating injury is a relative rare occurrence in the Netherlands compared with other countries. It is associated with high mortality and substantial hospital costs. The incidence of penetrating injuries is higher in metropolitan areas than in rural areas. A universal definition of penetrating trauma should be agreed upon in order to ensure that future studies remain free of bias, and also to ensure that data remain homogeneous.
Footnotes
Author contributions
Q.G.H.R. wrote the manuscript, collected data, and performed statistical analysis. A.C. assisted in writing and collecting data. J.P., L.M.G.G., G.F.G., and E.C.T.H.T. contributed in reviewing and writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data are not publicly available for legal reasons.
Informed consent
This article does not contain any studies with human participants or animals performed by any of the authors.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors and did not need ethical approval from our institutional review board.
Human rights
This study conforms to the ethical guidelines of the 1975 Declaration of Helsinki.