
Abstract
Background:
Retraining and retention for basic life support skills after initial basic life support education are important for high-quality basic life support performance at the scene.
Objectives:
We investigated whether delivery of a personal-training video clip reduced basic life support skill degradation in laypersons.
Methods:
After a basic life support layperson training course, the participants were randomized to the video group and control group. The layperson learners in the video group were provided with a video clip of themselves during basic life support education course and a follow-up text message every 3 months after initial basic life support course. The control group only received a follow-up text message every 3 months, without a video clip. The performances of all participants were reviewed initially and after 12 months in each group.
Results:
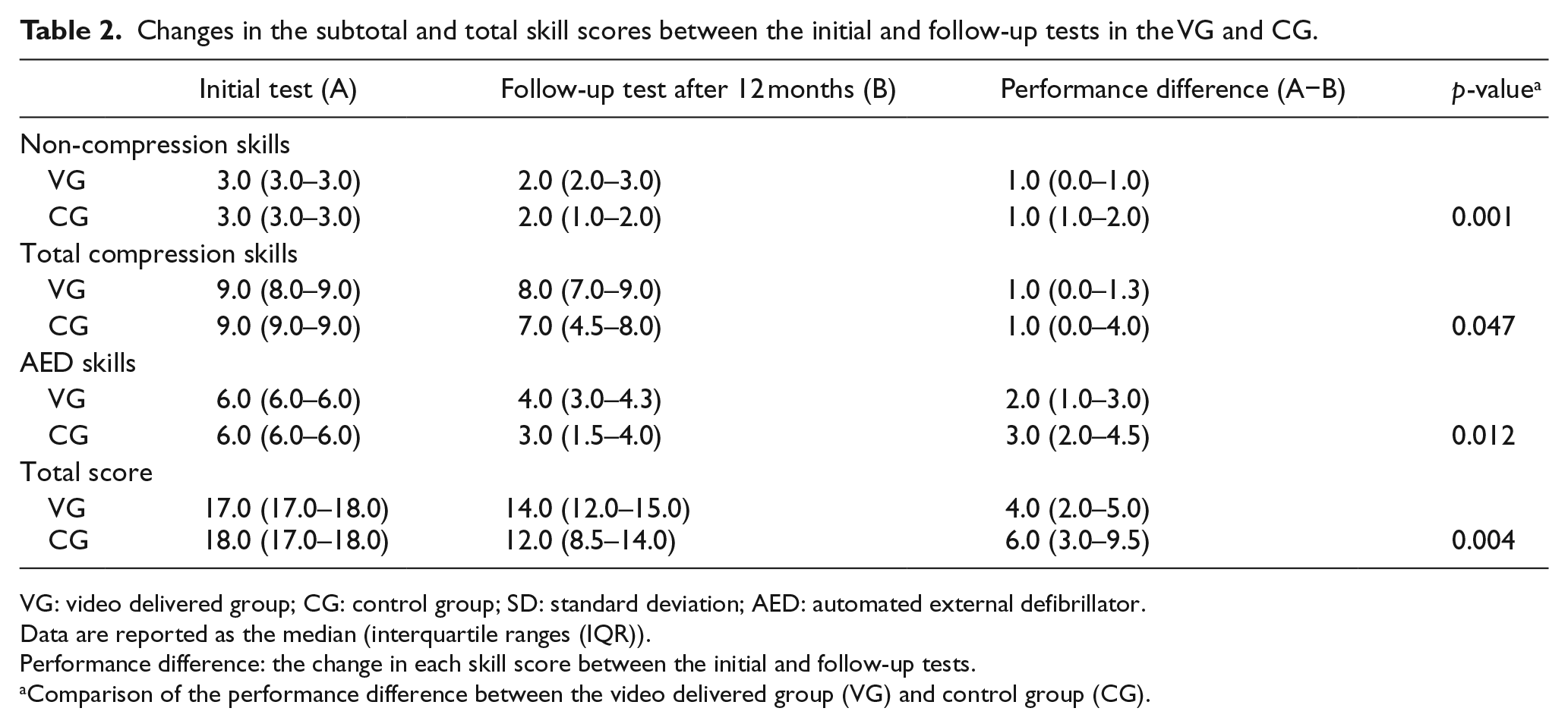
The total number of participants was 186. Among them, 22 in the video group and 29 in the control group completed the follow-up and final basic life support skill tests. In the control group, basic life support skill level of the participants was at 60.1% after 12 months compared with the initial test and 79.8% in the video group. The performance differences in each basic life support skill score between the initial and follow-up test at 12 months were significantly different between the video group and control group: non-compression, 0.0 (0.0–1.0) versus 1.0 (1.0–2.0); compression, 1.0 (0.0–1.3) versus 1.0 (0.0–4.0); automated external defibrillator, 2.0 (1.0–3.0) versus 3.0 (2.0–4.5) and total score, 4.0 (2.0–5.0) versus 6.0 (3.0–9.5), respectively (all p-values < 0.05).
Conclusion:
Delivery of a basic life support personal-training video clip to laypersons who received basic life support training can reduce performance degradation at 12 months.
Introduction
Out-of-hospital cardiac arrest (OHCA) is a leading cause of death worldwide. The incidence of OHCA in adults was more than 300,000 in the United States in 2016. 1 Despite advances in medical science, the survival outcomes for OHCA have remained low. Survival to hospital discharge after OHCA was 10.4%, and survival with good functional status was 8.4% in the Cardiac Arrest Registry to Enhance Survival (CARES) in 2017. 1 Extensive efforts have been invested to increase survival, and the best-known technique to date is the rapid initiation of cardiopulmonary resuscitation (CPR) and defibrillation at the scene.2,3 However, although rescue calls may be activated immediately in many cases, more than several minutes may pass before a health-care provider arrives at the scene. Therefore, without bystander-initiated CPR, there is no chance of preventing irreversible brain injury in victims. 4 To decrease mortality and improve neurological outcomes in cardiac arrest patients, immediate initiation of high-quality bystander CPR by laypersons is the cornerstone of the pre-hospital chain of survival. 5 Unfortunately, the majority of cardiac arrest victims do not receive bystander CPR, and it is difficult for bystanders to overcome the physical and emotional obstacles against performing CPR. 6
High-quality and continuous basic life support (BLS) education is essential to increase laypersons’ confidence and willingness to rapidly perform cardiac resuscitation at the scene. 7 Currently, conventional instructor-led education is the most common way of educating laypersons on BLS skills. However, it is difficult to hold enough courses where many people can participate, and the programmes of BLS education for the unspecified general public do not increase the rate of bystander CPR. 8 Furthermore, retraining and long-term retention for BLS skills after the initial BLS education, as well as the dissemination of the initial CPR training, are also important. 9 In previous studies, BLS knowledge and skills would deteriorate in as little as 2 or 3 months after the initial BLS training.9,10
With the development of multimedia and communication systems, video- or computer-assisted self-instruction represents a great alternative to replace conventional education.9–12 The transmission and playback of videos have become easier with the spread of mobile smartphones. People can engage in video-based learning frequently, and learning is, therefore, no longer limited by time and space. Taking video clips of trainees themselves and using them in education would be helpful to encourage confidence and motivation of trainees.13,14 However, limited evidence is available on retraining and long-term retention for BLS skills among laypersons using video clips delivered via mobile smartphones. The aim of this study was to evaluate whether providing individuals with personal-training video clips of themselves via mobile smartphones improved the retention rate of BLS skills in laypersons.
Methods
Study design and population
This study was a randomized controlled trial conducted in an academic training hospital CPR Training Centre between January 2013 and December 2014. This study was performed in compliance with the Declaration of Helsinki (Fortaleza, Brazil, 2013) and approved by the institutional review board of our institute (IRB No. 16-2012-19). All layperson trainees who received the BLS education course were eligible for the study. All the subjects were provided with information about the research, and the study was conducted among those who voluntarily participated. All participants were provided written informed consent. Health-care providers, associated students and people who had a medical occupation were excluded from participating. Trainees who could not perform CPR, pregnant women, individuals who could not participate in the follow-up test and people who did not use smartphones were also excluded.
Study setting and protocol
Approximately 120 BLS provider classes are held in our training site per year. The laypersons can participate in the BLS provider classes voluntarily. The BLS programme for laypersons included 1 h of theoretical education, 1.5 h of technical practice and 1.5 h of test with remediation. The theoretical education programme included the following: (1) instructions for recognizing cardiac arrest and making an emergency call, (2) instructions for chest compression and mouth-to-mouth ventilation at a ratio of 30:2 and (3) instructions for using an automated external defibrillator (AED). The theoretical course used a digital video disc (DVD) published by the Korean Association of Cardiopulmonary Resuscitation (KACPR). All training courses were conducted by instructors certified from KACPR or American Heart Association.
After the completion of the initial training, all trainees had a test for BLS provider course. The entire test process for the BLS provider course was recorded by the same instructor who provided the BLS course. After the initial test, all trainees were provided with the study information and decided whether to participate in the research study. Participants who agreed to enrol in the study were provided informed consent. The participants were randomized to one of two training groups for each follow-up visit: the video delivered group (VG) or control group (CG). Randomization was performed by a computer-generated random number table. Based on the previous studies those revealed BLS knowledge and skills would deteriorate in as little as 2 or 3 months after the initial BLS training,9,10 we chose the exposure interval as 3 months. The subjects in the VG were provided with a video clip of themselves during BLS education course and a follow-up text message which contains the BLS training summaries every 3 months after the initial BLS course. The video file was up to 20MB in size, with the duration of 50 s to 1 min. The CG only received a follow-up text message which contains the BLS training summaries every 3 months, without the video clip (Figure 1). All the personal-training video clips were transmitted using a mobile free-messaging application (KakaoTalk; Kakao Corp., Jeju-do, Korea) by investigators who did not participate in the test process. A total of four follow-up messages with or without a video clip were sent to each participant during the study period.
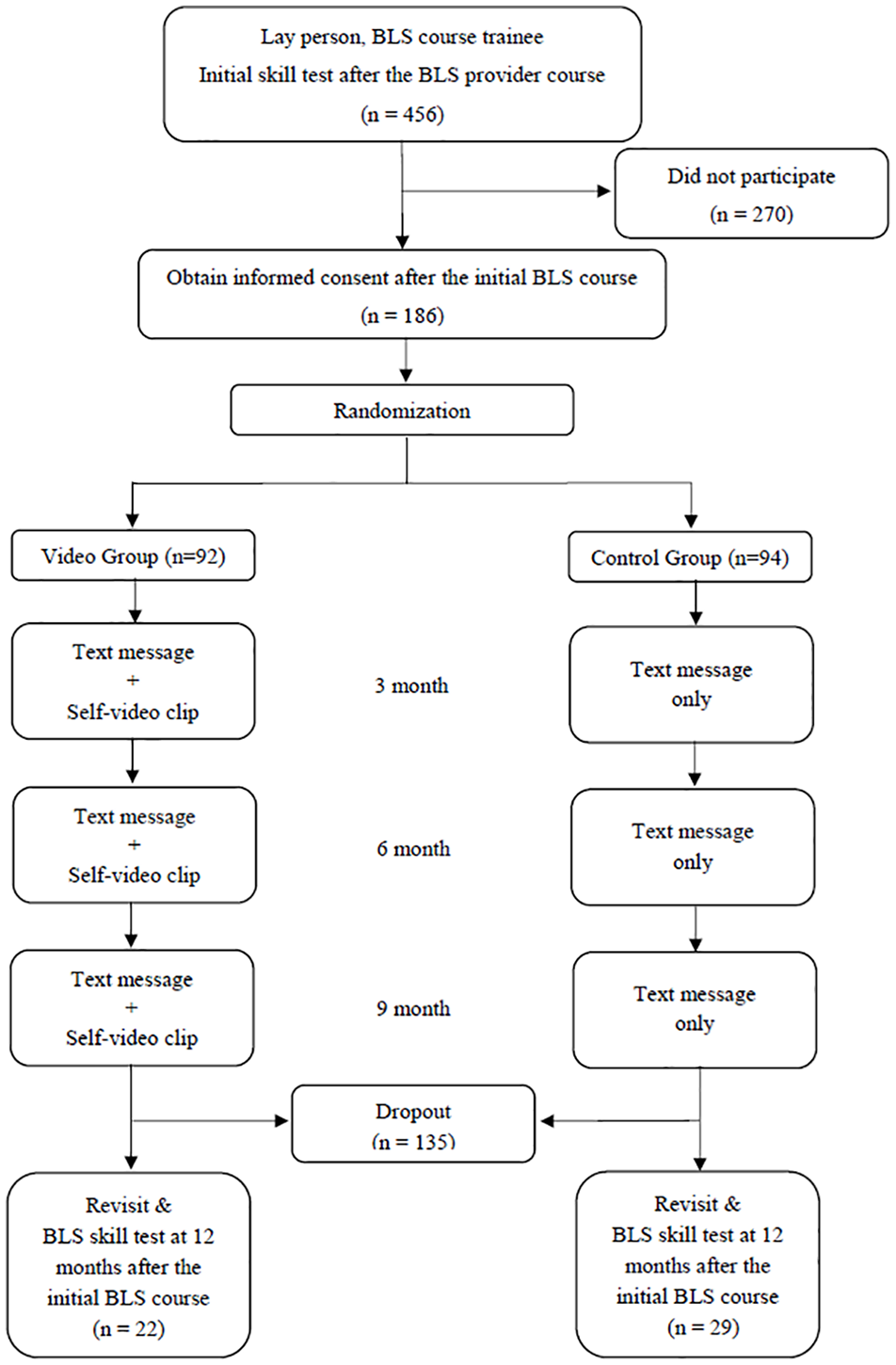
Flow diagram of subject participation in the study.
BLS skill retention was tested at 12 months after the initial BLS course. The same test programme was administered during the follow-up test by the same instructor who initially evaluated the participants. All the subjects who participated in the BLS follow-up test received a personal first-aid kit worth approximately US$30 as a reward. Until the end of the follow-up test, the BLS instructors were blinded to which participants received video clips. After the follow-up test, the investigator identified whether a subject had received the text message and video clip or had been educated by another institution. The initial and follow-up test results were recorded on the case report sheet and analysed (Figure 2).
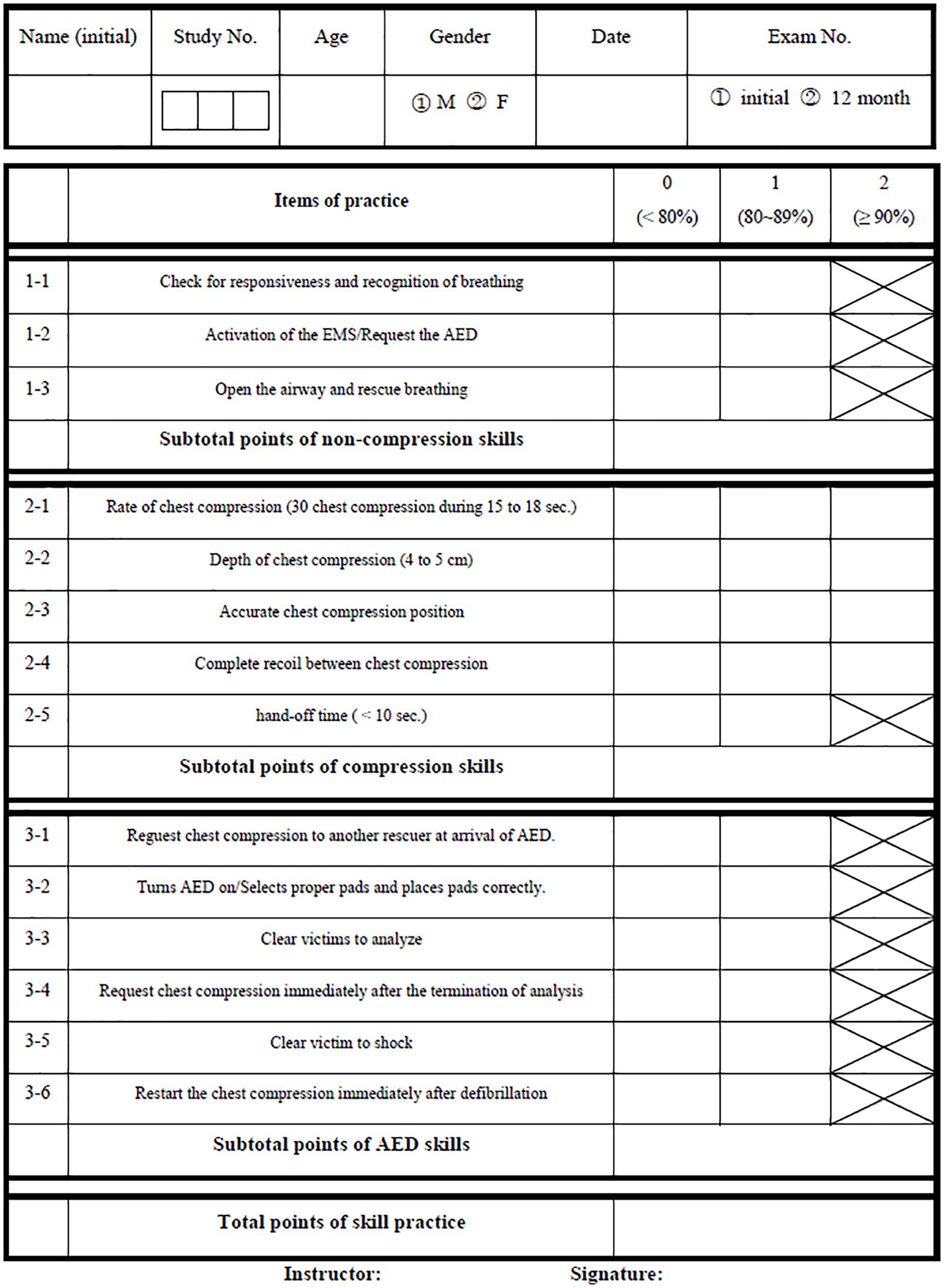
Checklist of the BLS training course for laypersons. The ticked boxes with cross indicate that the trainees can only receive a 0 or 1 in this item. If the trainee achieves < 80%, 80%–89% or ⩾ 90% of each item, the instructor gives a score of 0, 1 or 2 in each item, respectively.
Outcome measures
The primary outcome was the difference in BLS skill retention at 12 months after the initial BLS course between the VG and CG. The performance difference, which was defined as the change in each skill score between the initial and follow-up test, was used to indicate BLS skill retention. We assessed the quality of the participants’ BLS skills using a manikin simulator (Resusci® Anne; Laerdal Medical, Stavanger, Norway) during the initial and follow-up tests and the tests included the following skill parameters: (1) recognize cardiac arrest and ask for help by activating emergency medical services, (2) three cycles of single-rescuer CPR, including chest compressions and mouth-to-mouth ventilation and (3) two-rescuer CPR with the AED. The performances of all participants were recorded by one rater using a practice checklist that included a total of 18 points (3 points for non-compression skills, 9 points for compression skills and 6 points for AED skills) (Figure 2).
Statistical analyses
We estimated that the rate of decline in BLS skill retention among laypersons and health-care providers would be at least a 10% decrease for every 2 months.9,10,12 According to our experience and the results of pilot studies, we assumed the video delivery could reduce the rate of CPR skill reduction by 50%. Based on our estimation using effect size = 0.80, α = 0.05 and power = 80%, 52 subjects were required as the sample size calculated by the software G*Power version 3.1 (G*Power, Düsseldorf, Germany). Considering the pure layperson participants and the follow-up period10,12 and based on our previous experience that more than two-thirds of the layperson participants were lost to follow-up during 1 year, we assumed a potential dropout rate as 70% for the study period. Therefore, a total of 174 subjects were required.
Continuous variables were reported as the median with interquartile ranges (IQR) and categorical variables as the number with percentage. Mann–Whitney U test, X2 test or Fisher’s exact test were used as appropriate to compare the differences in baseline characteristics and performances on the initial and follow-up tests. Generalized estimating equations (GEE) method was used to evaluate the possible associations between age, gender, video delivery and time. Therefore, p-value < 0.05 were considered statistically significant, and the significance levels quoted were two-sided. The statistical analyses were performed using SPSS version 21.0 (SPSS, Chicago, IL, USA).
Results
During the study period, 456 BLS course trainees attended the BLS course and initial skill test. Among these trainees, 186 were participated in the study. All the participants were randomized to the VG or CG, 92 were in the VG and 94 were in the CG, respectively. A total of 135 participants (72.6%) did not attend the follow-up test after 12 months. Finally, 51 subjects completed the follow-up BLS test, of whom 22 (43.1%) had received the personal-training video clips (Figure 1). Baseline characteristics of the participants are shown in Table 1. The number of female participants was 43 (84.3%). The mean age of the participants was 34 years. There were no significant differences in age and gender between the groups.
Baseline characteristics of the participants.
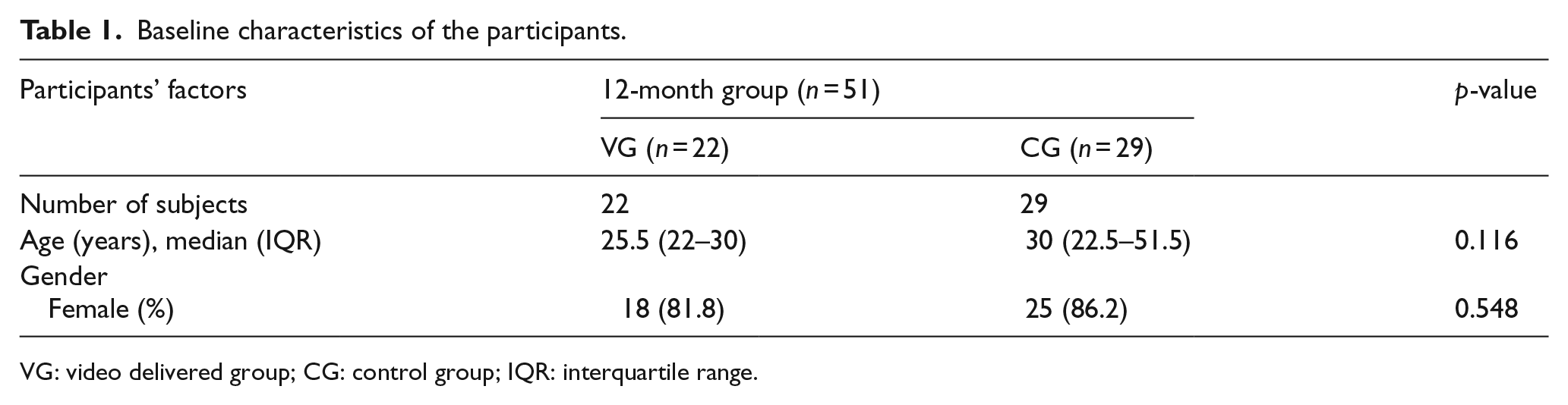
VG: video delivered group; CG: control group; IQR: interquartile range.
After the initial training, all participants showed high performance on the BLS skills. Most of them acquired perfect scores (18 points), and the mean total score of each group was greater than 17 points in the initial skill test. After 12 months, skill deterioration was markedly prevented in the VG across all the test parameters. The performance differences in each skill between the VG and CG after 12 months were as follows (median (IQR)): non-compression skills, 1.0 (0.0–1.0) versus 1.0 (1.0–2.0), (p = 0.001); compression skills, 1.0 (0.0–1.3) versus 1.0 (0.0–4.0), (p = 0.047); AED skills, 2.0 (1.0–3.0) versus 3.0 (2.0–4.5), (p = 0.012) and total score, 4.0 (2.0–5.0) versus 6.0 (3.0–9.5), (p = 0.004), in the VG versus CG, respectively (Table 2).
Changes in the subtotal and total skill scores between the initial and follow-up tests in the VG and CG.
VG: video delivered group; CG: control group; SD: standard deviation; AED: automated external defibrillator.
Data are reported as the median (interquartile ranges (IQR)).
Performance difference: the change in each skill score between the initial and follow-up tests.
Comparison of the performance difference between the video delivered group (VG) and control group (CG).
The percentage decrease in each skill score between the initial test and follow-up test scores was as follows: non-compression skills, 79.4% versus 54.5%; compression skills, 90.5% versus 71.4%; AED skills, 64.3% versus 46.1% and total score, 79.8% versus 60.1%, respectively. The retention of BLS skills and AED knowledge in the VG were superior to those in the CG. There was no correlation between BLS skill performance and gender, and an inverse relationship was observed for age. After adjusting for age, the decrease in BLS skill performance was still significantly reduced in all skill fields in the VG (Table 3, Figure 3).
Age-adjusted comparison of BLS skill retention between the initial and follow-up.
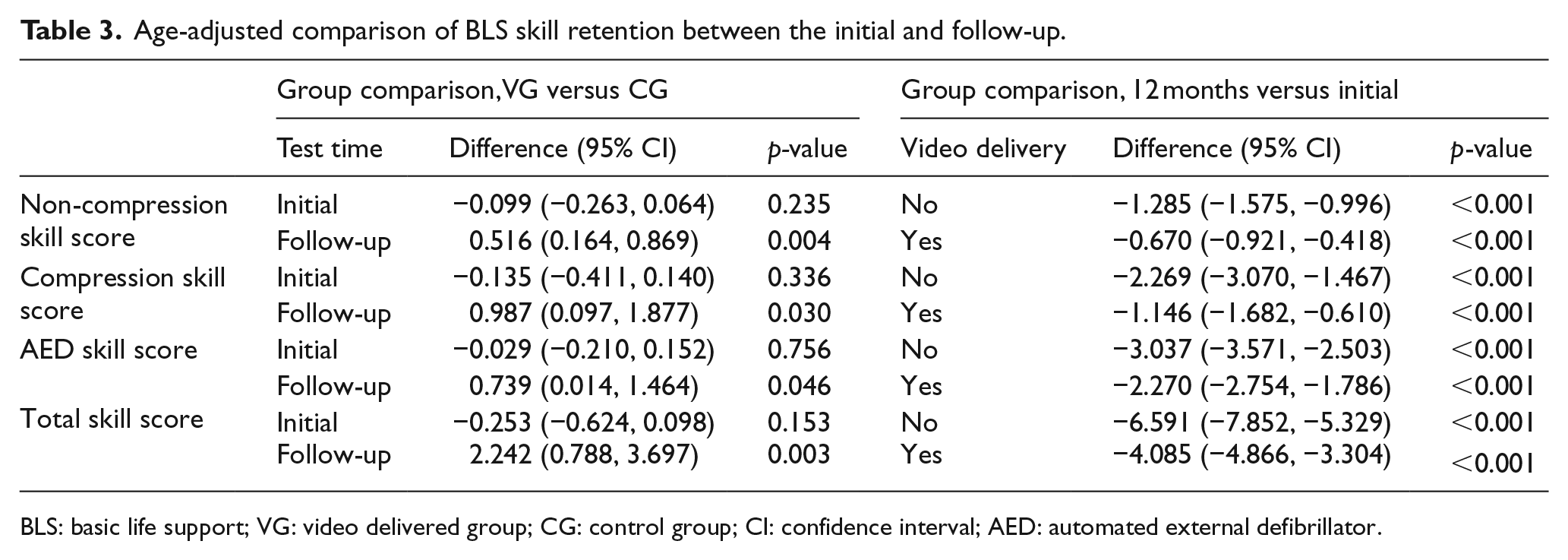
BLS: basic life support; VG: video delivered group; CG: control group; CI: confidence interval; AED: automated external defibrillator.
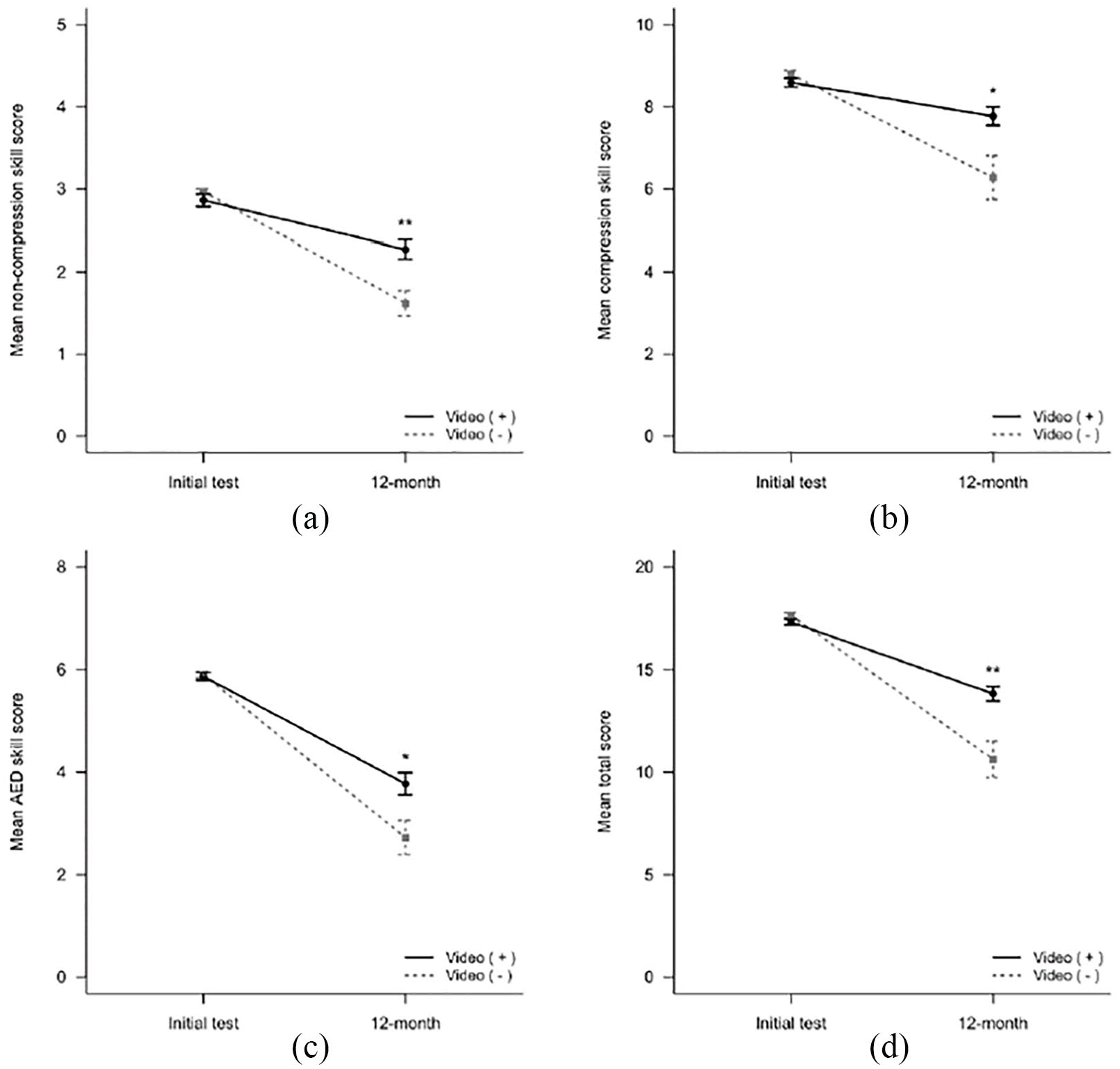
Age-adjusted mean skill scores on the BLS test according to the delivery of the video clips at 12 months: (a) Non-compression skill score. (b) Compression skill score. (c) Automated external defibrillator skill score. (d) Total score. Perfect scores for each test were 3, 9, 6 and 18 points, respectively.
Discussion
Retraining trained people is just as important as the dissemination of the initial CPR training. According to previous studies, BLS knowledge and skills decline in as little as 2–6 months.9,10,12,15–17 Therefore, high-quality CPR cannot be achieved in the field without adequate retraining using appropriate methods and intervals.
In our study, we found that the CPR performances of laypersons who were provided with personal-training video clips via a mobile smartphone remained strong over time. The 12-month-test scores of the VG were significantly higher across all skill fields (non-compression skills, compression skills, AED skills and total scores) than those of the CG. We also found that the delivery of the personal-training video clips prevented BLS skill degradation below a certain level until 12 months after the initial BLS education course, even after adjusting for age. This study showed that the BLS skill performance after 12 months was degraded to 60% of that in the initial BLS skill test. This result was similar to that of a previous study which was conducted in hospital staff, but not in laypersons. 11 In this study, BLS performance after 12 months was deteriorated to half of the level compared to that in the initial training. The percentage changes in each skill between the initial test and follow-up test scores in our study were as follows: non-compression skills, 79.4% versus 54.5%; compression skills, 90.5% versus 71.4%; AED skills, 64.3% versus 46.1% and total score, 79.8% versus 60.1%, respectively.
Only a few studies have evaluated CPR skill performance and retention at 12 months after the initial training in laypersons.17,18 However, these studies were limited in that all the participants were young university students or members of a company that manufactures CPR equipment. Our study subjects had the advantage of no other bias except for voluntary participation in the CPR education course. Compared with previous studies, this is the first study to show the effects of personal-training video clip delivery via a mobile device on laypersons’ BLS skill retention for up to 12 months. Moreover, this is the only study to consider the effect of the interaction between video delivery and age on BLS skill retention. Although age negatively affected BLS skill retention, gender did not seem to play a role in retention. These results are consistent with previous studies. 19
Many studies have tried to decide the appropriate CPR retraining time, but it is still uncertain. 7 Woollard et al. 20 suggested that the recommended interval for refreshing training should be no longer than 7 months to minimize the effects of skill deterioration. However, with the limitation in the instructor-led BLS education associated with time and training space, it is almost impossible for non-health-care providers to take the time to undergo BLS retraining every 6 months. Only a few laypeople can repeatedly participate in CPR retraining, such as the people who need to acquire or renew their certification.
Recently, alternative educational methods, such as the use of videos or computers, have been spotlighted to replace conventional instructor-led CPR education. Some studies have suggested that traditional education was superior to video-based CPR education, but video- and/or computer-based self-instruction with hands-on practice may be an effective educational method to replace conventional instructor-led courses. 6 The trainees seemed to benefit from the video clips of themselves to motivate CPR training and bystander-initiated CPR, and approximately half of the participants shared the videos with their acquaintances through social network services (SNS). This additional effect not only reduces CPR skill deterioration but also attracts public interest and participation in BLS. Additional time and cost savings are also expected.
Interestingly, AED skill deterioration occurred rapidly compared with other BLS skills, even in the group who received the video clips. AED skills are known to deteriorate more rapidly than compression skills according to previous studies.21,22 Video delivery alone did not prevent the decrease in AED skills effectively because the participants had to manipulate machines that they had not handled before. Supplementary methods, such as hands-on sessions or video clips that focus on using an AED, should be considered to maintain AED skill retention.
This study has several limitations. First, our study subjects were laypersons who voluntarily participated in the CPR education course. Therefore, we assumed a potentially high dropout rate of 70% based on our previous experience, which indicated that more than two-thirds of such participants were lost to follow-up during 1 year. The findings were consistent with our study results. The high dropout rate might be one of the main reasons for the exclusion of lay participants from previous studies. This study is the first study investigating BLS skill retention by laypersons for up to 12 months. Our study will assist educators and researchers in charge of CPR education. Furthermore, this study can be used as a reference standard for dropout rate in future studies investigating laypersons’ BLS skill retention.
Second, we did not know the education level or previous BLS training involving individual participants during this study. The participants exhibited heterogeneous levels of education. However, the education level and past BLS training experience of each participant affects BLS performance and retention of BSL skills following the initial BSL training. It might also be considered as a potential selection bias involving the study subjects.
Third, the video clips were delivered via a mobile smartphone; participants who did not have smartphones or those were not familiar with smartphones were excluded. In Korea, although the mobile smartphone penetration rate for people younger than 60 years is more than 90%, two-thirds of the population over 60 years do not use smartphones. 23 Therefore, our findings may not be generalized to elderly people.
Fourth, the number of female participants was dominant than the number of male participants despite randomization. It might be a potential for selection bias. However, this difference was not statistically significant between the VG and CG. In both previous studies and the current study, gender did not affect skill retention after video clip delivery. 19
Fifth, chest compressions and ventilation were not evaluated using a quantitative method. The simulation equipment used in this study could not quantify the compression quality. Although compression quality was evaluated by the same researcher to minimize the inter-rater differences, a quantitative analysis is necessary in the future study.
Sixth, we confirmed that all the participants in the VG had received and downloaded the video clips during the study period, but we did not report the playback times of each subjects in the VG. The number of video playbacks might have been different for each member in the VG. However, if video delivery is used for BLS retraining, the number of playbacks after file delivery cannot be enforced; therefore, the number of viewing times was not limited to reproduce the actual conditions.
Finally, the performance of the participants was measured using a manikin simulator. Therefore, it is unclear whether our findings can be generalized to an actual cardiac arrest situation.
Conclusion
We concluded that for laypersons, the delivery of a BLS personal-training video clip via a mobile smartphone could reduce BLS skill performance deterioration at 12 months after the initial education course. All BLS instructors should be aware of the significant declines in performance of non-compression and AED skills compared with compression skills among laypersons.
Footnotes
Author contributions
K.M.Y. and J.S. contributed to the conception and design of the study; S.J.L., H.J.L., J.H.J. and Y.J.S. contributed to the acquisition of data; K.M.Y., S.J.L., H.J.L. and S.Y.H. contributed to analysis and interpretation of data; K.M.Y., J.S. and S.J.L. drafted the article; K.M.Y., J.S. and S.Y.H. revised the article critically for important intellectual content and all authors have approved the final version of the article to be submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
The datasets generated and analyzed during the current study are available from the corresponding author.
Ethical approval
This study was approved by the institutional review board of Boramae Medical Centre (IRB No. 16-2012-19).
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
Informed consent
Written informed consent was obtained from all the participants for their anonymized information to be published in this article.