
Abstract
Background:
Epistaxis is one of the most common emergencies in the department of otolaryngology, which gives a burden to the health care system.
Objectives:
This study aimed to investigate the patients’ characteristics of hospital admission with epistaxis and provide an optimized protocol.
Methods:
This study was a retrospective analysis of patients with epistaxis admitted to The Third Affiliated Hospital of Sun Yat-sen University in Guangzhou, China. The data were analyzed in terms of gender, age, seasonal differences, length and expenses of hospitalization, pathogenesis of epistaxis, primary medical management before hospital admission, bleeding sites, and treatment.
Results:
A total of 387 patients were included, which consisted of 270 males and 117 females with an average of 43 years. Most patients could be identified with underlying diseases, and the most commonly observed bleeding site was Little area (n = 164). Most patients received electrocauterization as a precision medical treatment (n = 288). The duration of hospitalization length ranged from a mean of 5.17–4.48 days, and the expenses of hospitalization ranged from a mean of RMB 4881–4951 yuan over the last 5 years.
Conclusion:
Most patients with epistaxis could be treated as outpatients by endoscopic electrocauterization, and hospitalization is indicated when patients need improvement of poor general condition, posterior packing, embolization, or surgery. This study enables to provide an optimized protocol for patient with epistaxis.
Introduction
Epistaxis, defined as active bleeding from the nose, is a common problem with a significant cost to the health care system. 1 Patients suffering from sudden epistaxis are initially treated by otolaryngologists in the emergency departments, with the assistance of other physicians at the same time.2,3 Approximately 60% of individuals are thought to experience epistaxis at least once in their lifetime, with 6% requiring medical attention.4,5
Management of patients with epistaxis begins with resuscitating patients (when airway, breathing, or circulation of patients is unstable), seeking out the bleeding sites, managing epistaxis, and treating the underlying diseases. 6 Multiple therapeutic algorithms for epistaxis management are observation, electrocauterization, anterior with or without posterior nasal packing, endoscopic nasal sinus surgery, and embolization. 7 Meanwhile, many studies concerning the management of epistaxis and comparing the cost of different interventions have been published.1,8 However, the characteristics of patients requiring hospital admission for epistaxis have not been defined, and few reports about the optimized protocol have been published. 6
Based on the data of patients with epistaxis admission in the department of otolaryngology, we described patients’ characteristics with hospital admission for epistaxis and suggested an optimized protocol in epistaxis management for relieving the burden of health care system.
Methods
A retrospective study was performed on patients with epistaxis who discharged from the Department of Otolaryngology Head and Neck Surgery, The Third Affiliated Hospital of Sun Yat-sen University in Guangzhou, China. Electronic medical record was queried with a diagnosis of epistaxis (ICD-10: R04.001) from January 2014 to December 2018. In this work, we had tried but failed to obtain the written consents from those patients, and we make sure that no mention of specific name, gender, age, or address is present in this article. This study was reviewed in accordance with the ethical standards of the hospital ethics committee and the World Medical Association Declaration of Helsinki.
For analysis of epistaxis, data were retrieved from subjects in terms of the following: sex, age, seasonal differences, length, and expenses of hospitalization. Pathogenesis of epistaxis such as sinonasal diseases, hypertension, cardiovascular diseases, liver diseases, traumas, blood diseases, nasopharyngeal carcinoma, and hereditary hemorrhagic telangiectasia, and primary medical management before hospital admission, such as observation, anterior nasal packing, posterior nasal packing, and electrocauterization, were all recorded. Bleeding sites were confirmed using endoscopy, and those points were anatomically represented as Little area; nasal septum; inferior, middle, or superior turbinate; inferior, middle, or superior nasal meatus; and olfactory cleft and nasopharynx.
Treatment includes observation, electrocauterization, anterior with or without posterior nasal packing, endoscopic nasal sinus surgery, and embolization. Successful treatment was defined as no recurrent epistaxis after management and no readmission for epistaxis within 24 h of hospital discharge.
Results
Patients’ demographics
A total of 387 patients were admitted to our hospital with epistaxis; those patients consisted of 270 males with an average of 42 years (range from 2 to 87 years) and 117 females with an average of 44 years (range from 4 to 87 years). A downward trend was observed in the number of patients from 2014 to 2018, which indicated that patients required for hospitalization with epistaxis were decreased each year (Figure 1(a)). However, in terms of seasonal differences with epistaxis, there was no significant difference in the number of patients presented with epistaxis in each month (Figure 1(b)). Meanwhile, males are more likely to be admitted with epistaxis than females (the ratio of male and female was 1:0.43). Taking patients in all generations into consideration, the majority of patients in this study were in the age of 20 to 60 years, with fewer juveniles and the aged (Figure 1(c)).
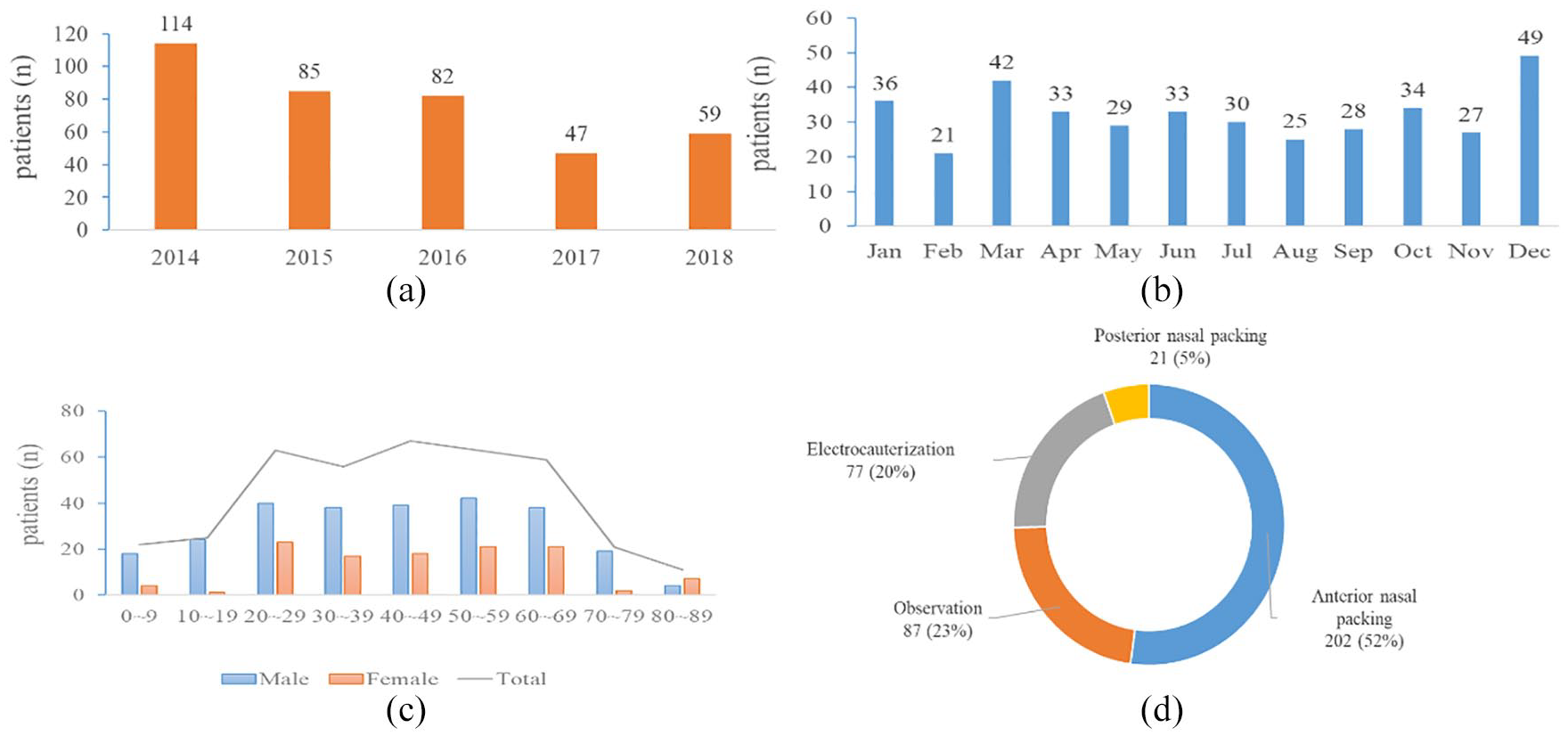
Characteristics of patients with epistaxis: (a) numbers of patients for hospital admission in each year, (b) monthly analysis of patients, (c) age analysis of patients and (d) analysis of primary medical management before hospital admission.
Primary medical management
A total of 202 patients were treated with anterior nasal packing using non-absorbable materials, and 77 patients were treated by electrocauterization. Besides, there are 87 patients received conservative treatment of observation because hemostasis has been achieved by the time of arrival. Meanwhile, posterior nasal packing was required in 21 patients for inefficiency of anterior nasal packing (Figure 1(d)). However, no patient received arterial ligation, embolization, or endoscopic nasal sinus surgery as primary management.
Pathogenesis of epistaxis
Pathogenesis of epistaxis was also identified in our work (Table 1), and the most common pathogenesis was sinonasal diseases, and there were 69 patients in this group. Other groups included cardiovascular diseases but are not limited to hypertension (89 patients), liver diseases (23 patients), traumas (13 patients), blood diseases (11 patients), nasopharyngeal carcinoma (8 patients), hereditary hemorrhagic telangiectasia (6 patients), and craniofacial fibrous dysplasia (1 patient).
Pathogenesis of patients presenting with epistaxis.

Hospitalization length and expenses
As shown in our study, there maybe a downward trend in the average length of hospitalization, from a mean of 5.17 days in 2014 to 4.48 days in 2018 (Figure 2(a)). However, the expenses of hospitalization showed an possible upward trend, from a mean of RMB 4881 yuan in 2014 to RMB 4951 yuan in 2018 (Figure 2(b)).

Characteristics of patients with epistaxis: (a) length of hospital stay in each year, (b) expenses of hospitalization in each year, and (c) analysis of bleeding sites for patients.
Bleeding sites of epistaxis
As for the bleeding sites of epistaxis, the most commonly observed site was Little area in our study, and there are 164 patients in this group (Figure 2(c)). Meanwhile, the bleeding site of other groups includes olfactory cleft (34 patients), nasal septum (33 patients), middle nasal meatus (31 patients), inferior nasal meatus (19 patients), inferior turbinate (14 patients), nasopharynx (8 patients), superior turbinate (6 patients), and middle turbinate (4 patients). However, our data showed that no bleeding sites were confirmed in 74 patients for hemostasis had been achieved before admission or after nasal packing.
Treatment for epistaxis
According to the distribution of bleeding sites, it was convenient for us to find out the bleeding sites, optimize the mode of treatment, and explore a minimally invasive and precision treatment for epistaxis. In this study, the offending arteries of epistaxis are mainly Kiesselbach’s plexus, followed with sphenopalatine artery and anterior or posterior ethmoidal artery.
In primary medical treatment, there were 87 patients who received conservative treatment of observation for non-continuing bleeding. In those patients, 40 patients with rebleeding during the hospitalization had received electrocauterization, while 47 patients were observed without intervention.
In the group of 223 patients with anterior or posterior nasal packing, after removal of the packing materials, 36 patients were observed without intervention, 171 patients received treatment of electrocauterization, and 4 patients underwent endoscopic nasal sinus surgery. Because of severe bleeding, in the group of eight patients with nasopharyngeal carcinoma, hemostasis stopped in two patients after embolization and removal of nasal packing and three patients with recurrent nasopharyngeal carcinoma gave up treatment, while three patients with recurrent nasopharyngeal carcinoma made a choice of transferring to another hospital for further treatment. Meanwhile, we had six patients with hereditary hemorrhagic telangiectasia and one patient with craniofacial fibrous dysplasia; during the treatment, we had little choice but to perform anterior nasal packing using absorbable materials after electrocauterization.
Discussion
In China, according to National Health and Family Planning Commission, the service radius of an emergency medical sub-station is about 3–5 km, equipped with experienced physicians, completed rescue equipments, and medicine, which provide effective treatment for critically ill patients. Most patients with epistaxis are initially treated by otolaryngologists in the emergency departments, with the assistance of physicians and then hospital admission. 9 The purpose of this study was to describe patients’ characteristics of hospital admission with epistaxis in the department of otolaryngology in Guangzhou and provide a model of optimized protocol for epistaxis management.
In our study, males were more likely to be admitted with epistaxis than females, with the ratio of 1:0.43. Different from other studies, 10 patients observed were more than 50 years old, in their 60s and 70s, but the majority of patients in our study were in their 20s to 60s, with less juveniles and the aged.
Studies indicated several risk factors for epistaxis-related hospital admission; the majority of these factors are patient related, such as sex, age, sinonasal diseases, coagulopathy, hematologic malignancy, and cardiovascular disease, including but not limited to hypertension. Evidence of seasonal variation of epistaxis is mixed, and the influence of season on epistaxis is not clear, may be due to population characteristics, comorbidities in different regions, or geographic variation. Patients with epistaxis predominantly appeared in the lower temperature months, because the temperature is associated with higher blood pressure and damaged nasal mucosae.11–13 In our study, there were no significant differences in the number of patients presented with epistaxis in each month and maybe more young people along with less varied temperature in Guangzhou all the year.
At the same time, the duration of hospitalization length ranged from a mean of 5.17–4.48 days, and the expenses of hospitalization ranged from a mean of RMB 4881–4951 yuan in 2014–2018. In other studies, the mean length of hospitalization of epistaxis admission was 2.9 days in England, 1 and costs of epistaxis admissions were extremely high, ranging from US$6282 to US$22,347 when arterial embolization was performed. 14
Therefore, we suggested an optimized protocol for epistaxis management. As the bleeding sites were visible by endoscopy, most cases of epistaxis can be successfully cured using electrocauterization in outpatient. Medical treatment such as electrocauterization was thought to be the most effective treatment method for epistaxis, 15 and the medical cost of electrocauterization is cost-efficient. First-aid measures should be provided by the emergency physician, and resuscitation was needed when airway, breathing, or circulation of patients was unstable. Hospitalization is indicated when patients need improvement of poor general condition, posterior packing, embolization, or surgery. Pathogenesis of epistaxis was given individual treatment subsequently. Posterior packing or surgery should be taken into account for all those patients, for example, ligation or coagulation of the sphenopalatine artery by endoscopy. However, if surgical treatment failed or the patient at risk of hemorrhagic shock, embolization was a reasonable alternative.16,17
We described the demographic features of patients with epistaxis and suggested an optimized protocol for epistaxis management, which was applicable to both otolaryngologists and non-ENT specialists. However, there was still a limitation in this study. It is a single-institute retrospective study of patients with hospital admission, and many outpatients were not analyzed, which is exposed by its nature to several biases.
Conclusion
We describe the patients’ demographics and bleeding sites of epistaxis with hospital admission over the last 5 years. Most of the bleeding sites could be easily cured by electrocauterization in outpatient. Hospitalization is indicated when patients need improvement of poor general condition, posterior packing, embolization, or surgery.
Footnotes
Acknowledgements
The authors thank members of Department of Otolaryngology Head and Neck Surgery, The Third Affiliated Hospital of Sun Yat-sen University for their assistance in preparing this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Undergraduate Teaching Reform Research Project of Sun Yat-sen University (no. 82000-18842502).
Availability of data and materials
A retrospective study was performed from patients with epistaxis who discharged from the Department of Otolaryngology, The Third Affiliated Hospital of Sun Yat-sen University in Guangzhou, China. Electronic medical record was queried with a diagnosis of epistaxis (ICD-10: R04.001) from January 2014 to December 2018.
Informed consent
If this article is a case study, then a separate consent document signed by the patient is required; otherwise, a single statement is required. In this work, we described a retrospective study of patients with hospital admissions for epistaxis, but we had tried but failed to obtain the written consents from those patients. We make sure that no mention of specific name, gender, age, or address is present in this article.
Ethical approval
All papers reporting animal and human studies must include a statement as to whether written consent was obtained from the local Ethics Committee or Institutional Review Board. In this work, we described a retrospective study of patients with hospital admissions for epistaxis, we make sure that no mention of specific name, gender, age, or address is present in this article. This study was conducted according to the ethical standards and the World Medical Association Declaration of Helsinki and under approval from the ethics committee of our hospital.
Human rights
This study was conducted according to the World Medical Association Declaration of Helsinki.