
Abstract
Background:
Triage plays a critical role in mass casualty incidents by optimizing the use of medical resources. The Formosa Fun Coast (Baxian Water Park) dust explosion incident in 2015 revealed the lack of resources in the Taiwanese medical system to handle large-scale burn and scald casualties; however, this incident resulted in only 3% mortalities (15/499) by the end of 2015.
Objective:
This study aims to examine the key features and correlated factors of the prehospital setting in 15 mortalities.
Materials and methods:
This retrospective cohort study enrolled all patients from the Formosa Fun Coast incident (N = 499). The follow-up period was from 27 June to 31 December 2015. We first examined the correlation between patient survival and various variables and then tested the correlation between survival-correlated variables and the level of hospitals that provided treatment.
Results:
The survivor and nonsurvivor groups shared similar distributions of all study variables. Emergency medical technician performed the triage assessment, and the Baux score correlated with patient survival. This study further tested whether the hospital level correlated with the emergency medical technician–performed triage assessment or Baux score. A chi-square test revealed that the emergency medical technician–performed triage assessment and Baux score correlated with patient survival, thereby indirectly affirming the planning, training, and auditing of the Taiwanese emergency medical technician system.
Conclusion:
The lack of the effect of the hospital level on patient mortality indicated that mortality might be related to the severity of burn injury rather than the level of hospital chosen for initial treatment, besides being related to a satisfactory emergency medical technician–performed triage system.
Keywords
Introduction
The simple triage and rapid treatment (START) system is an on-site, prehospital triage method of classifying patient severity in the event of large-scale casualties. START facilitates the treatment of the maximum number of patients in the shortest time and divides patients into four classes based on the condition of patients’ airway, breathing, circulation, and disability, thereby determining their priority for treatment or transfer to a hospital. 1 , 2 This system enhances the speed and appropriateness of not only medical treatment delivery but also the transfer of patients to hospitals. According to the “Guidelines for Emergency Medical Operation in Health Agencies and Medical Institutions regarding Mass Casualty Incidents,” the term “mass casualty” refers to any single incident or disaster that has or is anticipated to have more than 15 victims requiring emergency medical care. When the severity of injury or number of victims from an incident or disaster exceeds the capacity of the local medical system, the incident or disaster can be referred to as a mass casualty incident.
For an incident wherein there are numerous burned and scalded patients who require medical treatment, the revised Baux score can function as a triage method and is more effective than other triage methods in estimating patient mortality. 3 In addition to performing triage, a comprehensive system and regulations are necessary to allocate adequate medical resources. The relevance of proper triage methods is exemplified by the 9/11 incident in the United States that prompted a collaboration between burn and scald centers in different states, contributing to the establishment of a triage system for preventing backline medical resources from being occupied by patients with minor medical conditions during emergencies. Laws and regulations on transferring patients to backline hospitals have also been developed.4–6
In qualified hospitals across Taiwan, there are 295 beds for burn and scald patients (167 in intensive care units and 128 in burn units), and 122 of these beds (41.4%) are located in northern Taiwan. Of these 122 beds, 89 (73.0%) are in the medical center. Notably, few differences exist between medical and nonmedical centers. First, medical centers have trauma team availability within 10 min and adequate workforce to deal with a mass casualty. Second, a medical center has on-call sub-specialty physicians, such as a plastic surgeon and chest physician, all the time (24/7). Third, a medical center can take over patients transferred from a nonmedical center when patients’ care is beyond its capability.
Before the Formosa Fun Coast dust explosion incident on 27 June 2015, Taiwanese officials had neither substantial experience in handling a large-scale burn casualty incident nor any corresponding treatment plans. The Formosa Fun Coast dust explosion resulted in 499 victims (15 mortalities and 484 victims with different levels of burns and scalds) by the end of 2015, which exceeded the total number of hospital beds available in Taiwan for burns and scalds. Studies conducted abroad have shown a marginal decrease each year in the number of burn and scald medical centers and hospital beds for burn and scald patients. 7 Therefore, the maximum medical treatment capacity of hospitals is attained through triage, and the burns and scalds handling capacity of hospitals is optimized by conducting regular educational training sessions and establishing a centralized processing mechanism for burns and scalds–related resources. During the Formosa Fun Coast dust explosion incident, overall 41,648 physicians (measured in person-days) provided care for burn patients (a maximum of 829 physicians within 1 day). Moreover, the overall expenditure on health personnel’s incentive allowance was New Taiwan Dollar 300 million (US dollars 10 million). The Formosa Fun Coast dust explosion incident placed a heavy burden on the Taiwanese medical system, revealed the system’s inadequacies, and provided the managers of the emergency medical system an opportunity to amend its shortcomings and redesign it to be more comprehensive. Because of support from the entire medical system, the number of deaths (n = 15) caused by the Formosa Fun Coast dust explosion incident was lower than what was originally expected. At the present stage, determining different prognoses of patients of similar age is crucial.
Materials and methods
This study was based on a retrospective cohort of all patients from the Formosa Fun Coast dust explosion incident (N = 499), and the follow-up period of patients was from 27 June to 31 December 2015 (187 days). Study variables were sex, age, emergency medical technician (EMT) triage assessment, emergency severity index, burn and scald classification, total body surface area (BSA) of burn, Baux score (BSA + patient’s age), patient’s transport method to hospitals, and the level of hospitals that provided subsequent treatment. These variables were tracked between 27 June and 17 August 2015 (50 days). Integration of original data and statistical analysis of data were conducted separately by different research assistants. First, data were analyzed using descriptive statistics. Second, the correlation between each study variable and patient mortality was tested. Subsequently, variables that correlated with patient survival were tested to observe whether they correlated with the hospital level. Pearson’s correlation was used to determine the relationship between patient survival and study variables. A p value of ⩽0.05 was considered statistically significant, and all analyses were performed using SPSS statistical software for Windows, version 19.0 (SPSS, Chicago, IL, USA).
Results
The patients were divided into two groups: survivors (n = 484) and nonsurvivors (n = 15), with an average of 44% BSA in all the patients. The two groups shared similarity regarding average age and sex. Most of the patients were sorted to more severe levels, as evidenced by both the emergency severity index and EMT-performed triage assessment. Regarding the 15 mortality cases, all suffered from burn injury of >50% BSA (average 72.8% BSA), only 2 patients died within 1 week from respiratory failure, and 13 died from sepsis-related multiple organ dysfunction syndrome. Overall, 248 patients (49.7%) suffered a scalding injury of >40% BSA. Regarding the emergency severity index, most patients were Level 1 or Level 2 (100% of nonsurvivors; 74.7% of survivors).
Based on the EMT-performed triage assessment, conditions of most patients were of high or medium severity (100% of nonsurvivors; 79.6% of survivors). The burn and scald classification and Baux score were higher in the nonsurvivor group; most nonsurvivors had a third-degree burn (86.7%) and a Baux score of more than 50 (100%). In addition, most of the patients (n = 355; 71.1%) were sent to medical centers for treatment initially (66.7% of nonsurvivors; 71.3% of survivors; Table 1). The results of the correlation analysis between each variable and patient mortality revealed that EMT-performed triage assessment (p = 0.0478) and Baux score (p = 0.0062) correlated with patient survival. However, the hospital level did not correlate with patient survival (p = 0.6977; Table 2).
Age and number distribution of the survivor and nonsurvivor groups.
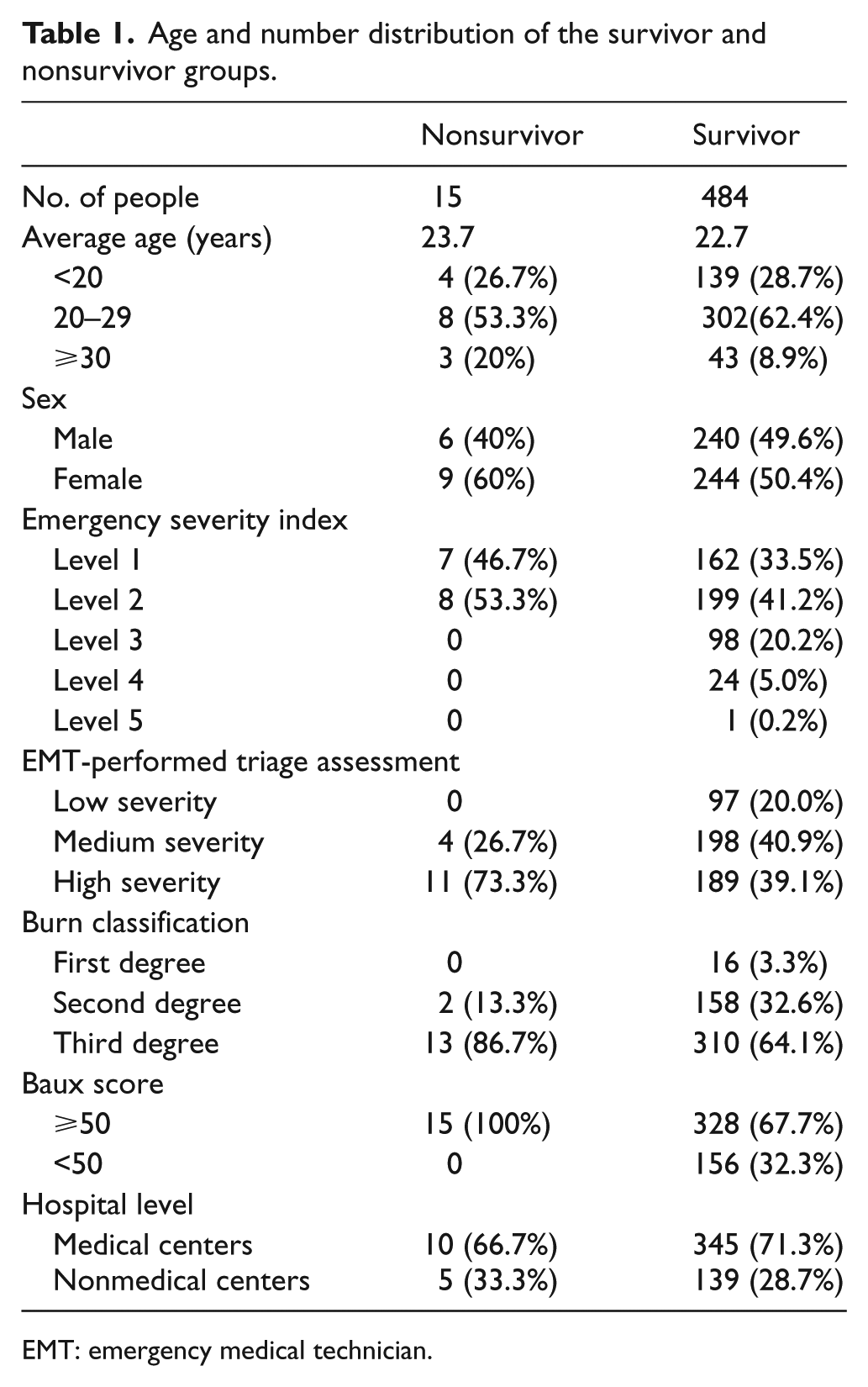
EMT: emergency medical technician.
Correlation between patient survival and study variables.
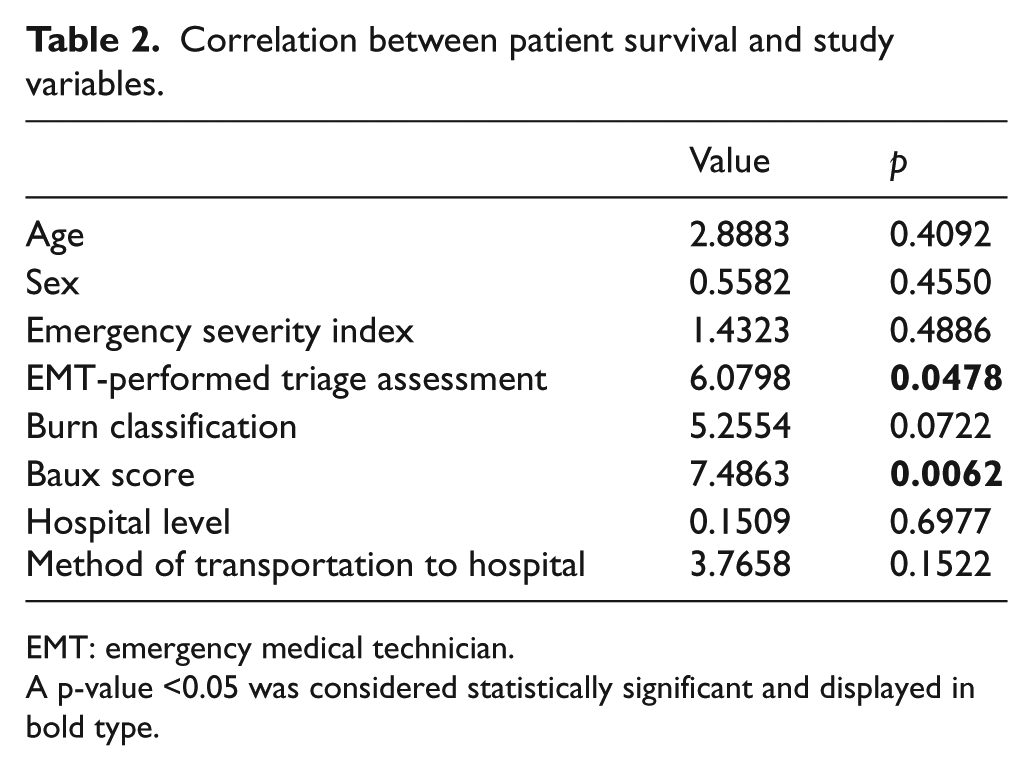
EMT: emergency medical technician.
A p-value <0.05 was considered statistically significant and displayed in bold type.
This study examined whether EMT-performed triage assessment and Baux score correlated with the hospital level. Results demonstrated that EMT-performed triage assessment correlated with the hospital level (p = 0.0067). This finding may be attributed to the comprehensive EMT training system and auditing practice of training institutions, which ensure EMT competency in transferring patients to a suitable hospital (Table 3).
Correlation between the hospital level and EMT-performed triage assessment and Baux score.
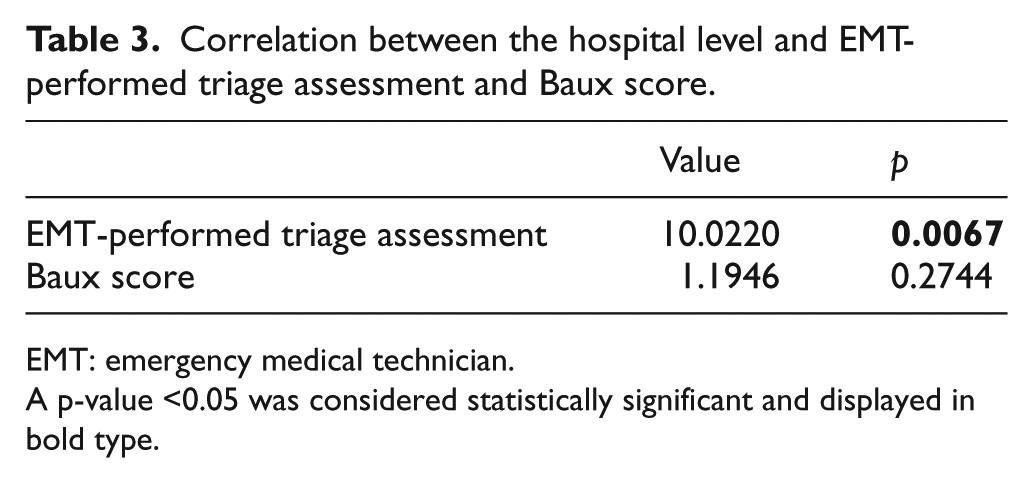
EMT: emergency medical technician.
A p-value <0.05 was considered statistically significant and displayed in bold type.
Discussion
This incident at Formosa Fun Coast, a recreational water park, resulted from starch-based powder explosion and is considered the worst incident of large-scale trauma in Taiwan. Most of the injured patients were healthy and aged between 10 and 30 years. Most patients were sent to medical centers, possibly because of a higher number of medical centers in northern Taiwan (N = 9) than any other part of Taiwan. 8 After initial treatment, 288 patients (57.7%) were admitted to the intensive care unit, and 49 hospitals all over Taiwan were involved in the subsequent treatment of all patients. However, most patients could be transferred directly to high-level hospitals because of their burn or scald severity assessment based on EMT-performed triage assessment results. Among nonsurvivors, 10 patients died in medical centers. This study divided patients into survivor and nonsurvivor groups before conducting a chi-square test to analyze the remaining study variables. Among 15 mortalities, only 2 patients (13.3%) died within 1 week, and 9 patients (60%) died within 1 month, 4 patients (26.7%) died after 1 month. Among nonsurvivors, 3(20%) were transferred to other hospitals after initial treatment because of the need for a burn care unit, and mortality owing to secondary infection after 1 week may be related to the percentage of the scald injury rather than the hospital level. Results showed that EMT-performed triage assessment and Baux score correlated with patient survival, thereby suggesting that EMTs performed satisfactory preliminary triage assessment when handling patients. Consequently, this finding indirectly affirms the effectiveness of the planning, training, and auditing of the Taiwanese EMT system. 9
The hospital level did not affect the patient survival, which can be attributed to the fact that regardless of whether a hospital is a medical center, a regional hospital, or a district hospital, it can offer the required emergency trauma treatment and has adequate intensive medical care facilities. Risk factors for mortality in burn patients were female gender, burn size, and old age. 10 In this incident, survival correlated with the Baux score and EMT triage assessment. Most of the patients in this incident were young; thus, the severity of burn injury and the percentage of BSA were the main factors of mortality. Nonetheless, the result was also related to the application of the preliminary triage, which enabled patients with relatively severe conditions to be sent to higher-level hospitals and receive extensive medical care. Consequently, this study further analyzed whether the hospital level correlated with the EMT triage assessment or Baux score. Results determined that the EMT-performed triage assessment and hospital level were correlated. In addition, the EMT-performed triage assessment correlated with patient survival and hospital level; however, the hospital level did not correlate with patient survival, which can be attributed to an insufficient number of cases or transfer of patients to another hospital after the initial treatment. Despite the lack of inhalation-injury-related data, results demonstrated that the Baux score correlated with patient survival. Therefore, the Baux score can undoubtedly serve as an on-site patient triage tool, provided it is revised in accordance with medical advancements to ensure that the tool complies with current medical standards. 11
Conclusion
The lack of the effect of the hospital level on patient mortality indicated that mortality is associated with the severity of burn injury rather than the level of hospital which performed the initial treatment, besides being dependent on a satisfactory EMT-performed triage system. A correlation analysis among the hospital level, EMT-performed triage assessment, and Baux score revealed that only EMT-performed triage assessment correlated with the hospital level.
Footnotes
Author Contributions
Tsung-Hsi Wang was responsive for manuscript writing, Hui-An Lin for data collection, Wei-Fong Kao for table drafting, and Chun-Chieh Chao for revision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Exempted the requirement of informed consent approved by IRB.
Ethical approval
This study was approved by the Institutional Review Board of Kaohsiung Veterans General Hospital.
Human rights
There is no objection to human rights in this study.