
Abstract
Introduction:
Ingestion of common household cleansing products resulting in a need for intubation is not uncommon in Hong Kong. The objective of this study was to determine the factors that affect the mortality in this group of patients.
Methods:
This was a retrospective cohort study conducted in the Hong Kong Poison Information Centre, encompassing data from all Accident and Emergency Departments in Hong Kong over the period of 1 January 2008 to 31 January 2019. This study was conducted by recruiting all patients who had ingested common household cleansing products and required intubation in the same hospital admission. The outcome was death. The study aimed to look at risk factors associated with mortality.
Results:
Seventy-seven patients were included in the final analysis. The median age was 53 years. The mortality rate was 21%. Univariate analysis (at p < 0.05) indicated that (1) older age, (2) ingestion to intubation time more than 12 h, (3) not admitted to intensive care unit, (4) complication of chest infection, (5) complication of fast atrial fibrillation, and (6) complication of acute kidney injury were factors associated with higher mortality rate. Among these, older age and development of acute kidney injury were statistically significant (p < 0.05) on multivariate analysis.
Conclusion:
Among patients who ingested household cleansing products and required intubation, older age and development of acute kidney injury were factors strongly associated with mortality.
Introduction
Common household cleansing products in Hong Kong include Dettol and related products (e.g. Walch and Lenndorf), multipurpose cleaners (e.g. Swipe, floor cleaner and kitchen cleaner), bleach, and surfactants (e.g. detergents, shampoo, and laundry fluids). They are commonly classified as irritants when ingested. Ingestion of these chemicals, especially Dettol, appeared to be a popular suicidal method among the Hong Kong population. 1
These products have a common effect of causing aero-digestive tract irritation,2–8 when ingested in small to moderate amounts, and central nervous system depression,9–11 when ingested in large amounts. Severe poisoning can result in cardiopulmonary arrest. 9 The irritation on the gastrointestinal tract causes vomiting and a predisposition to development of aspiration pneumonia.9,12 Endotracheal intubation would be needed in these situations.
Strong caustics were not included in this study as they have a significantly different chemical composition and pharmacokinetic profile on human body compared to the aforementioned chemicals. 12 In addition, strong caustics are not a commonly possessed cleaning product in household use.
Methods
Study design
This was a retrospective cohort study based on the territory-wide database of the Hong Kong Poison Information Centre (HKPIC) and Clinical Management System. The parent data set included cases encountered by clinical frontline staff and surveillance data from routine reporting of poisoning cases by all Accident and Emergency Departments (AED) under the hospital authority. The study population was screened from the total case load that the HKPIC had received during that period, which was about 4000 cases per year. Demographic data of the patients were reviewed from the patients’ electronic health record.
Patients who ingested common household cleansing products and required intubation in the same hospital admission were included. We collected data from 1 January 2008 to 31 January 2019. Ninety-one patients were identified from the HKPIC database. Exclusion criteria included (1) unknown ingestion time; (2) ingestion chemical charted as “unknown cleansing product,” but with clinical course highly suggestive of a strong caustic; (3) patients who died as a result likely due to another different co-ingested poison; and (4) patients who were certified death before hospital admission. Case notes were reviewed by two authors to arrive at the decision of case exclusion.
The products ingested were classified into four groups, namely: (1) Dettol and Dettol-related products, (2) multipurpose cleaners, (3) bleach, and (4) surfactants. Dettol and Dettol-like substances are common household antiseptic products available in the market. Typical active ingredients include chloroxylenol, dichloroxylenol, isopropyl alcohol, and pine oil. Multipurpose cleaners are household cleaners that are used to clean floors and furniture. Local examples include Swipe® and Green water. Typical active ingredients include low concentration of alkali, surfactants, organic solvents, pine oil, and isopropyl alcohol. Household bleach typically contains <10% sodium hypochlorite as the active ingredient. Surfactants are household or laundry detergents. If more than two products were ingested, the one with the larger volume was chosen as the major component for analysis. The results are listed in Table 1.
General characteristics of all patients and results of statistical analysis related to mortality.

The relationship between age and mortality was tested based on Wilcoxon rank-sum test, while the other factors were based on Fisher’s exact test.
The relationship toward mortality was tested using multivariate logistic regression model.
The volume of ingestion was categorized into subgroups of (1) small (⩽150 mL), (2) moderate (151–500 mL), and (3) large (⩾501 mL). This was related to two to three mouthfuls of ingestion, being approximately less than a volume of 150 mL; one regular size bottle commonly sold in the local market would usually be at least 500 mL in quantity.
For the analysis on ingestion to intubation time, a cut-off time of 12 h was used consistent with previous studies, which proposed that delayed airway obstruction (⩾12 h) after Dettol ingestion was uncommonly seen. 3 The time of ingestion was determined by history, collateral information from witnesses, and/or other circumstantial evidence as charted on medical record. The time of intubation was defined either by the registration time of post-intubation chest radiography or by the operation theater record. Analysis was done on whether ingestion to intubation time ⩾12 h was associated with higher mortality.
Acute kidney injury (AKI), the acute change in estimated glomerular filtration rate (eGFR), was defined according to the creatinine criteria of Kidney Disease Improving Global Outcomes (KDIGO) classification. 13 Serum creatinine levels at the AED and in ward were obtained. An increase in serum creatinine by ⩾0.3 mg/dL (⩾26.5 µmol/L) within 48 h after admission and/or an increase in serum creatinine to ⩾1.5 times baseline within the previous 7 days was defined as AKI by the KDIGO classification. Complication of chest infection was defined as patients who had at least two signs or symptoms (cough, pleuritic chest pain, shortness of breath, temperature more than 38°C, and crackles or bronchial breath sounds), plus radiographic confirmation, 14 as determined by the treating clinician and evidenced on medical record. Complication of fast atrial fibrillation was defined as development of atrial fibrillation as evidenced by the electrocardiography with a rate equal or more than 100 beats/min, confirmed by treating clinicians and evidenced on medical record. Complications that had a minimal occurrence with 0% or a 100% mortality rate are listed in Table 2.
Table of complications.

SVT: supraventricular tachycardia.
Included deep-vein thrombosis, pulmonary embolism, and inferior vena caval thrombosis.
Included non–ST-elevated myocardial infarction and ST-elevated myocardial infarction.
Statistical analysis
Statistical analysis was performed by R (statistical language program). Age was analyzed using Wilcoxon rank-sum test to compare the difference in median age between the survival and mortality group. Categorical factors were analyzed with Fisher’s exact test. A multivariate logistic regression was performed on the significant factors from the univariate analysis. A value of p < 0.05 was regarded as statistically significant.
Results
A total of 91 patients were identified. Fourteen patients were excluded based on the exclusion criteria. Seventy-seven subjects were included in the final analysis (Figure 1). The male-to-female ratio was 3:7. The median age of all patients was 53 years (range: 15–91). The median age of survival group was 47 years and that of the death group was 82 years.

Flow chart of exclusion.
Seventy-six patients (99%) were in a well-functioning state and graded independent on the scale of Activities of Daily Living. Seventy-two cases were intentional ingestion, accounting for the majority (94%). Four patients (5%) had accidental ingestion and one patient’s (1%) intention was unclear.
For the product ingested, Dettol and Dettol-like products accounted for 55%, multipurpose cleaners 23%, bleach 17%, and surfactants 5%. The median volume ingested was 300 mL (range: 15–1800 mL). Nine patients (12%) had co-ingestion of two or more kinds of household cleansing products. No cases had ingested bleach together with acids. Twenty cases (26%) had co-ingestions of other drugs including alcohol, hypnotics, rodenticide, paracetamol, antihistamine, amlodipine, diclofenac, famotidine, and salicylates. One case had intentional carbon monoxide inhalation poisoning.
For intubation reason, 34 patients (44%) had a low Glasgow Coma Scale state (GCS ⩽ 8), 50 patients (65%) had features of upper airway obstruction (UAO), and 5 patients (6%) had cardiac arrest. The patient can present with more than one feature. For intubation site, 52 patients (67%) were intubated in the AED, 9 patients (12%) in the general ward, 9 patients (12%) in the intensive care unit (ICU), and 7 patients (9%) in the operation theater. The median ingestion to intubation time was 2 h (range: 15 min to 73 h). For patients intubated in the AED, the median AED to intubation time was 24 min (range: 4 to 157 min). For patients not intubated in the AED, the median AED to intubation time was 5 h (range: 30 min to 73 h). Seven patients (9%) had ingestion to intubation time ⩾12 h (range: 13–73 h). Sixty-seven patients (87%) were admitted to ICU, and 10 patients (13%) were admitted to general ward.
Forty-four patients did not develop any complications (57%). Chest infection was seen in 26 patients (34%), with a mortality rate of 46%. Fast atrial fibrillation was seen in eight patients (10%), with a mortality rate of 88%. Among the cases with fast atrial fibrillation, only two patients in the mortality group had a documented medical history of atrial fibrillation. AKI was seen in eight patients (10%), with a mortality rate of 88%. Among the cases with AKI, none had a documented medical history of renal impairment.
Statistical analysis
Statistical analysis results—univariate analysis
The median age of the survival group and that of the death group were analyzed by the Wilcoxon rank-sum test. The results showed that the median age of the two groups was different with a statistical significance (W = 94.5, p value < 0.001).
For categorical factors, Fisher’s exact test showed that ingestion to intubation time ⩾12 h, not admitted into ICU, complications of chest infection, fast atrial fibrillation, and AKI had a statistically significant impact on the patient’s mortality rate (at p < 0.05).
The relative risks (RR), absolute risk increase (ARI), and number needed to harm (NNH) with 95% confidence interval (CI) of the identified significant factors in univariate analysis are listed in Table 3: (1) ingestion to intubation time ⩾12 h had an RR of 3.33, ARI of 40%, and NNH of 2.5; (2) not admitted into ICU had an RR of 4.02, ARI of 45.1%, and NNH of 2.2; (3) complications of chest infection had an RR of 4.70, ARI of 36.3%, and NNH of 2.8; (4) fast atrial fibrillation had an RR of 6.71, ARI of 74.5%, and NNH of 1.3; and (5) AKI had an RR of 6.71, ARI of 74.5%, and NNH of 1.3.
Univariate analysis—relative risk (RR), absolute risk increase (ARI), and number needed to harm (NNH) with 95% confidence interval (CI).

ICU: intensive care unit.
Statistical analysis results—multivariate logistic regression
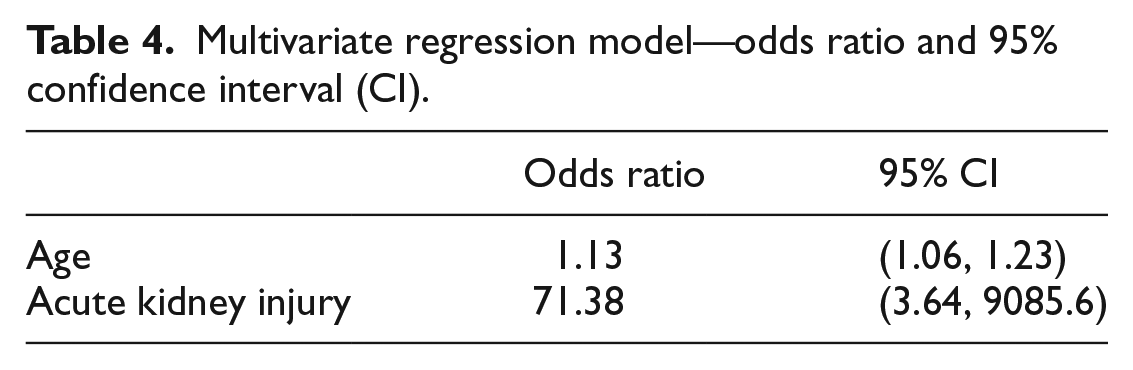
The multivariate logistic regression results showed that of the six factors (namely, age, ingestion to intubation time ⩾12 h, not admitted to ICU, chest infection, fast atrial fibrillation, and AKI), only age and AKI were statistically significant at 95% confidence level in the multivariate model. As such, we retained only the factors age and AKI into a second multivariate logistic regression model. The results and fitted parameters of the second model were consistent with that from the first model. The R2 value of the final logistic regression model was 0.547. The odds ratio and 95% CIs are listed in Table 4. Odds ratio for older age was 1.13 and that for AKI was 71.38.
Multivariate regression model—odds ratio and 95% confidence interval (CI).
Discussion
This is by far the largest local retrospective cohort study in Hong Kong on patients who ingested common household cleansing products and required intubation. We aimed to recruit severely poisoned but not medically futile (certified in AED or had a Do-Not-Attempt Cardiopulmonary Resuscitation (DNA-CPR) code) patients. To our knowledge, there are no previous studies focusing on this subgroup of patients. There were sporadic fatal case reports9–11 due to ingestion of household common products, but there was no specific research on the associated risk factors related to mortalities. Our study sought to examine the risk factors related to mortality in this defined group of severely poisoned patients.
Age
Older age was associated with higher mortality based on both univariate analysis (p < 0.001) and multivariate analysis (p = 0.001). All patients below the age of 65 years survived (mortality rate 0%). The mortality rate for patients aged above 65 years was 53%. The implication could be as age advances, there would be less physiological reserve toward the poisonous effect of the chemicals, and thus older patients are more prone to complications and death. At the same time, an extreme old age puts the patient on a lower admission triage category into the ICU. This may explain why admission into the ICU was significant on univariate analysis (p = 0.004) but not on the multivariate analysis (p = 0.955), as ICU admission may be a confounding factor related to older age.
Chemical profile
The difference in mortality rate between patient groups ingesting different types of chemicals did not reach the significant level of p < 0.05 (p = 0.059). Surfactant group may appear to have an unexpectedly high mortality rate of 75%, but surfactant cases in total were the least among the four subgroups, accounting for only 5% (4 of 77). This was in line with the common observation that ingestion of surfactant seldom leads to a need for intubation. As for the three mortality cases in the surfactant group, two patients developed chest infection and one patient developed AKI. These findings may suggest that if the ingestion of surfactants led to a need for intubation, the clinical seriousness should not be underestimated.
Our statistics did not suggest that the volume ingested was directly related to mortality (p = 0.686). One possible explanation was that the ingested products could vary in preparation and dilution methods, thus the volume ingested may not precisely reflect the true dosage of the poison. The differences in concentrations would also lead to varying irritating power of the chemical on the aero-digestive tract. Nonetheless, a mentally depressed patient may not be able to volunteer an accurate ingestion history, and it would be difficult for a witness to note the ingested volume precisely.
One previous study suggested that co-ingestion of a mixture of household cleansing products can produce an antagonistic, additive, or synergistic effect. 15 In our study, co-ingestion of two or more cleansing products was not related to higher mortality (p = 0.675).
Ingestion to intubation time
Ingestion to intubation ⩾12 h was statistically significant in the univariate analysis (p = 0.031) but not on the multivariate regression model (p = 0.052).
Among the seven patients who had ingestion to intubation time ⩾12 h, only one case was due to late presentation (presented to AED 13 h after ingestion). The other six were decided for intubation after admission. As such, ingestion to intubation ⩾12 h appeared mostly related to a late decision to intubate. Therefore, cases whose decision to intubate were made after admission, either in the general ward or in the ICU, were studied to see whether they show features of requiring intubation already in the AED (Table 5).
Clinical details of ward or ICU intubation.
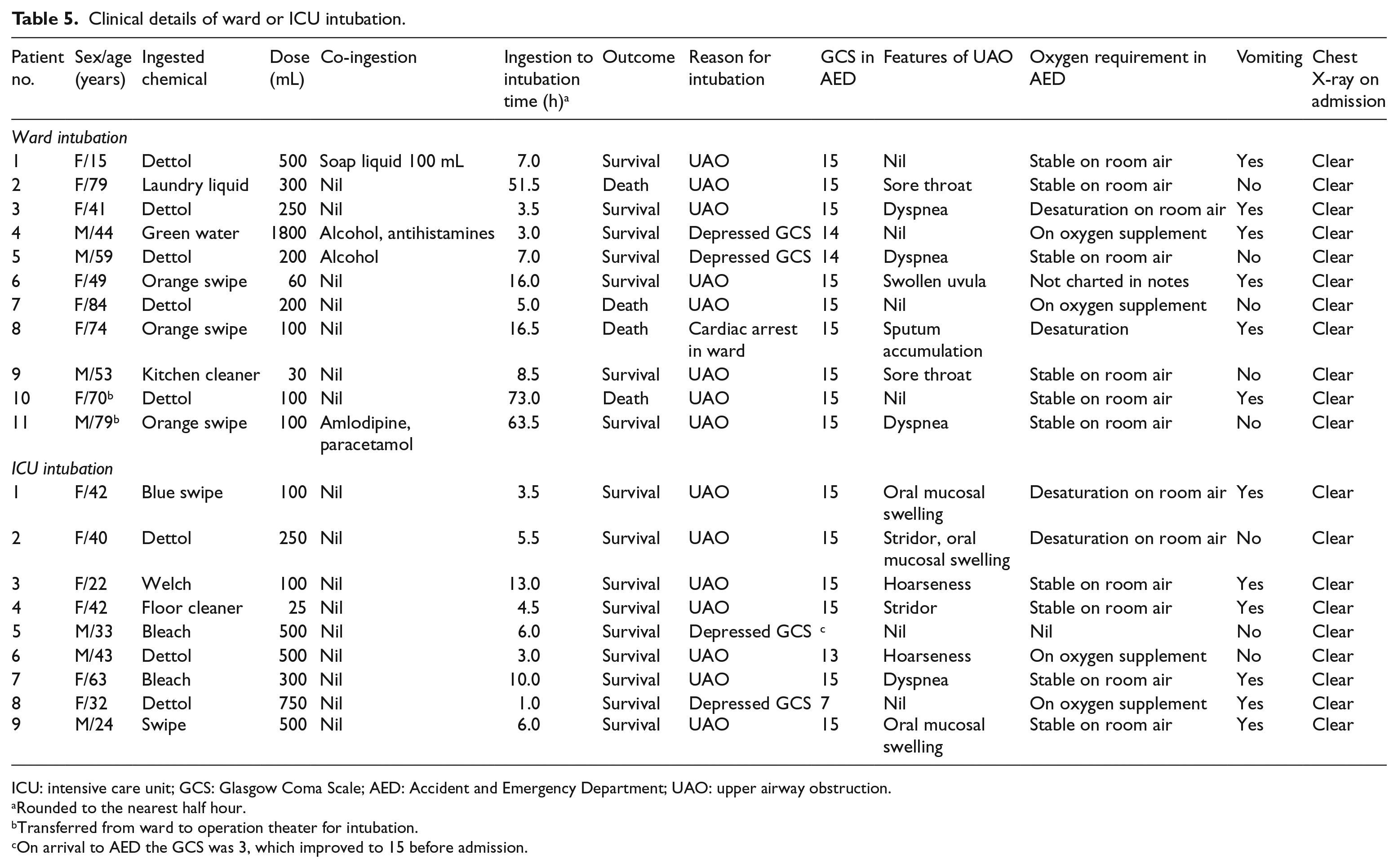
ICU: intensive care unit; GCS: Glasgow Coma Scale; AED: Accident and Emergency Department; UAO: upper airway obstruction.
Rounded to the nearest half hour.
Transferred from ward to operation theater for intubation.
On arrival to AED the GCS was 3, which improved to 15 before admission.
Eleven patients (14%) were admitted to a general ward for monitoring and later intubated. The two patients intubated due to low GCS in the ward showed confusion at the AED with depressed GCS. The eight patients intubated due to UAO in the ward had clinical features of UAO and/or desaturation at the AED. The one patient intubated at cardiac arrest in the ward had wheezing, desaturation, and vomiting at the AED. The data showed that all 11 patients who were decided for intubation in the general ward probably had features of warranting intubation already in the AED. The ingestion to intubation time was further prolonged if the patient was sent for intubation in an operation theater. The mortality rate among general ward intubated cases was 36%.
Nine patients (12%) were admitted to the ICU for monitoring and later intubated. The two patients intubated for low GCS in the ICU had a depressed GCS in AED. The seven patients intubated for UAO in the ICU had features of UAO in the AED. Again, the data showed that all patients intubated in the ICU probably had features of warranting intubation already in the AED. The mortality rate among ICU intubated cases was 0%.
For patients admitted but not intubated, upper airway condition and the conscious level should be closely monitored. In a previous case report, delayed UAO resulting in a need for intubation can happen as late as 48 h after ingestion. 2 Another case series over a 4-year period later suggested that a delayed need of airway intervention later than 12 h was unlikely. 3 In our study, there were seven patients (9%) who were intubated after 12 h. The result was that the mortality rate was significantly higher in the late intubation group on univariate analysis but not on multivariate regression. This may be due to the interconnected relationship between delayed intubation, aspiration pneumonia, and old age, with old age accounting for a larger effect. The statistics may suggest that for these patients, an early intubation strategy may be of benefit, but a larger sample size would be needed to verify its statistical significance.
Complications relating to mortality
Chest infection was statistically related to mortality in the univariate analysis (p < 0.001) but not in the multivariate analysis (p = 0.992). It was difficult for our study to determine whether the patients suffered from aspiration pneumonia, hospital-acquired pneumonia, or ventilator-associated pneumonia from the limited clinical notes available. The statistical insignificance on multivariate model might be again related to the interconnected relationship between delayed intubation, aspiration pneumonia, and old age.
Fast atrial fibrillation was statistically related to mortality in the univariate analysis (p < 0.001) but not on the multivariate regression model (p = 0.065). Some studies showed that the ingested cleansing product chemical molecules could be found on the vasculature of the lung, liver, kidney, and brain capillaries on post-mortem examination,6,8,15 and it could be that the chemical had also deposited on the cardiac cells resulting in dysfunction. In the literature, there was a case report noting nodal tachycardia after Dettol ingestion. 16 Studies showed that atrial fibrillation and the effect of causing tachycardia-related cardiomyopathy was associated with increased mortality compared to sinus rhythm, especially in the elderly.17–19 Although the multivariate regression model indicated that fast atrial fibrillation may represent a confounder related to elderly age, this complication with a high mortality rate (88%) should be noted during the clinical course.
AKI was statistically related to mortality in both univariate analysis (p < 0.001) and multivariate analysis (p = 0.03). Previous studies showed that ingestion of these chemical irritants can lead to AKI.11,20–24 Renal impairment was suggested to be due to a direct toxic effect of the chemical on the kidney, including deposition of chemicals on the tubular epithelial cells in loop of Henle 21 and the Bowman’s capsule, 11 causing acute tubular necrosis and renal cortical necrosis.6,24 At the same time, renal impairment could be due to hypotension during cardiovascular collapse and part of the multiorgan failure sequelae. 20 As such, the importance of monitoring the renal function during the clinical course of household cleansing product ingestion should be noted.
Other complications with 100% mortality
In our study, there was one patient who was known to be affected with colonic stenting for colorectal carcinoma; he developed a block of the stent after Dettol ingestion, resulting in intestinal obstruction, bowel ischemia, and eventually death. There was one case report in the literature of a patient developing intestinal obstruction after ingestion of kitchen detergent. 25 Intestinal obstruction after ingestion of common household cleansing products remains a rare but potentially fatal complication, which should be paid attention to when treating patients with pre-existing gastrointestinal conditions.
In our study, ST-segment elevation myocardial infarction (STEMI) and non–ST-segment elevation myocardial infarction (NSTEMI) were seen in four patients, resulting in 100% mortality. In an appropriate clinical context, STEMI is defined as ST-segment elevation (ST-elevation) or new left bundle-branch block on the electrocardiogram (ECG). While NSTEMI is defined as the absence of persistent ST-elevation with elevated cardiac biomarkers. 26 The data in our study were subtracted from clinical notes determined by treating clinician. None of these patients had a coronary angiography or intervention done. This complication with 100% mortality may represent a state of terminal illness and should be noted in the clinical course.
Upper gastrointestinal bleeding and the need for oesophageal-gastro-duodenoscopy
There were previous studies suggesting that oesophageal-gastro-duodenoscopy (OGD) may increase the risk of aspiration in patients who ingested household cleansing products and had an impaired consciousness; thus, OGD is not required unless other causes of gastrointestinal bleeding were suspected.5,27,28 In our study, only two patients (3%) had features of upper gastrointestinal bleeding, and they had other co-existing factors predisposing to bleeding besides the household cleansing product ingestion. One patient developed coffee ground vomiting after bleach ingestion, with co-ingestion of warfarin-related rodenticide, and elevated international normalized ratio (INR) time. One patient with known cirrhosis and esophageal varices developed complications with bleeding of the varices after Dettol ingestion. Otherwise no patient had upper gastrointestinal bleeding. A dedicated study focusing on the relationship of aspiration pneumonia with OGD may be a meaningful topic for future research.
Difficult airway
Potential difficult airway in intubating a UAO could be challenging for the clinician and hazardous for the patient. In our study, there was only one patient who was charted to have a difficult airway at intubation. She was intubated in the AED for features of UAO, where two doctors (one emergency physician and one anesthetist) failed to intubate. She was eventually intubated by a senior anesthetist. She suffered from peri-intubation cardiac arrest. She was extubated on day 8 and survived till hospital discharge 8 weeks later.
Intubation duration, re-intubation, and the need of tracheostomy
The median intubation duration among survived patients was studied. The calculation was done after excluding the one case who had unknown extubation time, the one case who required re-intubation, and the four cases who were weaned from an endotracheal tube to a tracheostomy tube. The median intubation duration among different sets of patients is listed in Table 6. The median intubation duration for all patients was 2.0 days; for complication-free patients, it was 1.8 days; for patients with complications, it was 3.7 days; and for patients with chest infection, it was 4.2 days. These results may suggest that for those with a non-complicated clinical course, an intubation duration of 2 days may be sufficient for the depressed mental state and the UAO to subside. However, further study to examine the optimal intubation duration and extubation timing is needed.
Median intubation duration. a

After excluding unknown extubation time, weaned to a tracheostomy tube and/or required re-intubation.
Four cases in our study required re-intubation. One case appeared to be a premature extubation signified by re-intubation in the same day. The other three cases were re-intubated for development of chest infection. The premature extubation case survived, while all re-intubated cases due to chest infection died.
Four cases in our study were weaned from an endotracheal tube to a tracheostomy tube. One case had surgical tracheostomy performed 13 days post-ingestion, due to persistent supraglottic edema. The reasons and timing for the three other cases were not clearly charted. It was noted in the literature that prolonged laryngeal edema and severe upper airway stenosis can occur after ingestion of household cleansing products. 29
Limitations
This retrospective cohort had a small sample size due to the rarity of the disease occurrence. To increase sample size as much as possible, we traced subjects as far as to the start of the HKPIC electronic recording system. There were potential biases in our study. Our parent data set was from a voluntary reporting basis by clinicians; therefore, potential selection bias would arise if the attending medical staff did not seek toxicology advice from the HKPIC and at the same time did not report the case to the HKPIC. That said, noting the fact that our study focused on the intubated patients, we believe that it is likely that the clinician would seek toxicological advice from HKPIC when treating these critically ill patients.
Second, potential information bias could arise from non-entry of data. The clinician may accidentally not chart the development of different complications in the clinical notes. Same situation could occur for the record on the patient’s upper airway condition. If the patient was intubated due to low GCS or cardiac arrest, the clinician may not notice the upper airway condition. At the same time, the upper airway conditions were mostly charted as clinical assessments like mucosal swelling, drooling or hoarseness. The majority of the cases did not have a formal charting of the laryngeal grading at intubation or a bronchoscopy done throughout their admission.
In our study, 20 patients (26%) had co-ingested other drugs and 9 patients (12%) had a mixture of cleansing product ingestion. The decision to intubate and clinical course was partly complicated by these non-fatal co-ingestions, although statistically it was not significant. Many areas about the systemic effect of these chemicals on human body when ingested were not well understood in pathophysiological terms. There are many aspects in this topic that can be further studied as suggested in the text above.
Conclusion
In conclusion, our study provides early evidence that older age and AKI were associated with higher mortality rate among patients who ingested household cleansing products and required intubation. Chest infection and fast atrial fibrillation, although not completely supported by all our statistical analyses, appear to be potentially serious complications associated with higher mortality, which we suggest clinicians to pay attention to. An early decision to intubate may be of benefit, and monitoring of this group of patients should preferably be in an ICU.
Footnotes
Acknowledgements
The authors would like to thank Dr Tse Man Li of the Hong Kong Poison and Information Centre for his intellectual support to their study.
Authorship
L.S. designed and conceptualized the study, analyzed the data, and drafted the manuscript for intellectual content. C.C.K. interpreted the data and revised the manuscript for intellectual content. A.Y.K.L. designed and conceptualized the study, interpreted the data, and revised the manuscript for intellectual content. D.C.K.M. had a major role in acquisition and interpretation of the data and revised the manuscript for intellectual content. All the authors approved the article to be published. All authors participated sufficiently in the work to take public responsibility for appropriate portions of the content. The authors alone are responsible for its contents and writing of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data were retrieved from the HKPIC and Clinical Management System database of HA.
Ethical approval
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by The Kowloon Central Cluster Ethics Committee of the Hospital Authority Hong Kong (Ref.: KCC/KEC-2018-0276).
Human rights
There were no human rights conflicts to declare.
Informed consent
Written informed consent was not necessary because no patient data have been included in the manuscript.