
Abstract
Background:
Thoracic impedance monitoring able to detect pneumonia in the very early phase of emerging infiltration prior the patient developed remarkable clinical symptoms. However, no studies have yet been conducted on the usefulness of predicting pneumonia patient outcomes with parameters from electrical cardiometry.
Objective:
In the present study, we evaluated whether parameters measured by electrical cardiometry can predict clinical outcomes including mortality and length of hospital stay in patients with community-acquired pneumonia in the emergency department.
Methods:
Demographic, clinical and laboratory data were collected from enrolled patient. Electrical cardiometry monitoring was done with a portable electrical cardiometry device connected to the body surface sensor. The continuous data from electrical cardiometry were recorded, and parameters were stored on the electrical cardiometry device automatically and then the data were downloaded for further analysis.
Results:
Thoracic fluid content has shown to be significantly higher in the intensive care unit admission group and in the death group. Expired patients had higher value of thoracic fluid content at emergency department admission. From a receiver operating characteristics curve analysis, thoracic fluid content presented fair AUC values of 0.72 (95% confidence interval, 0.71–0.74) and 0.73 (0.62–0.82) for prediction of 28-day mortality and intensive care unit admission. Arterial partial pressure of oxygen (PaO2), the ratio of arterial partial pressure of oxygen to inspired oxygen fraction (PaO2/FiO2 ratio) also showed excellent AUC value for prediction of mortality and intensive care unit admission.
Conclusion:
Electrical cardiometry monitoring indicated new possibility to anticipate prognosis of community-acquired pneumonia patient. Increased thoracic fluid content value would relate worse outcome of the patient like mortality and intensive care unit admission. Electrical cardiometry monitoring allows real-time measurements of thoracic fluid content without restraining the patient or invasive catheters.
Introduction
Community-acquired pneumonia (CAP) is a major infection-related cause of hospital admission and mortality in elderly patients that often leads to intensive care unit (ICU) admission and subsequent mechanical ventilation. 1 Initial treatment of CAP includes administration of sensitive antibiotics and supportive measures. Emergency department (ED) physicians should understand a patient’s prognosis for rapid and proper management of CAP.
Several scoring systems are available to predict the outcomes of CAP patients and to help clinicians assess the severity of the illness. The CURB-65 is the most popular simple severity scoring system that uses five variables that include age over 65, new onset confusion, elevated respiratory rate (RR), low blood pressure (diastolic ⩽ 60 mmHg or systolic ⩽ 90 mmHg) and elevated blood urea nitrogen (BUN) to assign a 6-point score (0–5). Scores correlate with low (0–1), intermediate (2) and high risk (>3) for short-term mortality. 2 Pneumonia severity index (PSI) scores help to delineate the severity of CAP patients who are at low risk for short-term mortality and eligibility for outpatient care. 3 PSI categorizes patients into four risk classes based on 30-day mortality rates. Patients with a score of 70 or less are classified into class II, 71–90 into class III, 91–130 into class IV and more than 130 into class V. From a study comparing aged-matched control subjects, PSI was reported to reflect patient short-term and long-term mortality. 4 Shock index and hypoxemia (SIPF) score is a combined scoring system that combines the shock index (heart rate (HR)/systolic blood pressure) >0.7 (1 point) and the ratio of arterial partial pressure of oxygen to inspired oxygen fraction (PaO2/FiO2; P/F ratio) <250 (1 point). Eldaboosy et al. 5 discovered that SIPF is an accurate predictor with higher predictive power than PSI and CURB-65 for intensive care admission due to CAP. Although these scoring systems have been proven useful, they usually comprise multiple parameters from demographic data or laboratory data, which are collected separately throughout clinical practice. However, a method is needed to continuously assess outcomes based on how the patient’s condition changes at the bedside.
Acute pulmonary infection is characterized by alveolar epithelial and vascular endothelial damage leading to increased permeability pulmonary oedema and alveolar fluid collection. 6 Alveolar fluid clearance is associated with clinical outcomes of pneumonia patients including mortality, duration of mechanical ventilation and degree of oxygenation. 7
Electrical cardiometry (EC) is a noninvasive method that measures stroke volume (SV) determined by calculating beat-to-beat changes in the electrical impedance of the chest and neck. This method can measure cardiac output (CO) noninvasively and continuously at the bedside. 8 Previous studies have highlighted the benefits of using EC for checking hemodynamic parameters such as CO and SV. It has been increasingly utilized in the analysis and treatment of dyspnoeic patients.9,10 The thoracic fluid content (TFC) is a measure of water contained in the lungs and pulmonary vasculature that is obtained from EC. Increased TFC is associated with higher alveolar permeability which is the sum of interstitial, alveolar, intracellular and lymphatic fluids, but not pleural effusion. 11 Intra-alveolar fluid is generally elevated in pneumonia with airspace consolidation, and it can be hypothesized that TFC and decreased impedance are markers of pneumonia severity; however, no study has been conducted on predicting clinical outcomes of patients with pneumonia using EC parameters.
Therefore, we proposed that EC measurements could be used to predict dyspnoeic CAP patient outcomes and help determine if intensive care is needed. In the present study, we evaluated whether parameters measured by EC can predict clinical outcomes including mortality, length of hospital and ICU stay in patients with CAP.
Method
Design, patients and emergency treatments
A retrospective chart review was undertaken at a 24-bed ED of The Catholic University of Korea, Daejeon St Mary’s Hospital, a 600-bed secondary medical centre. The study protocol was reviewed and approved by the institutional review board of Daejeon St Mary’s Hospital, (DC18RESI0109). We used data from medical records of patients who complained of dyspnoea (UMLS (unified medical language system) code: 207059009) on ED arrival between April 2017 and March 2018 and who were diagnosed with pneumonia (ICD-10; J10.0, J10.1, J10.8, J11.0, J11.1, J11.8) at hospital discharge. Patients with a history of pulmonary lobectomy or lung trauma were excluded. Patients finally diagnosed with other diseases such as pulmonary embolism, congestive heart failure, renal disease and hematologic disorders including anaemia were also excluded from this study. Patients with dyspnoea in this study were treated with oxygen therapy via a nasal prong or facial mask, and routine antibiotics were administered after blood culture in the ED in accordance with CAP guidelines. 12
Data collection
Demographic, clinical and laboratory data of enrolled patients were collected from the medical records. Information on medical treatment including oxygen supplementation and ventilator support were also documented from the medical records.
EC monitoring
Four surface electrodes were placed on the patient’s skin: first on the left neck below the ear, second on the left midline at the base of the neck, third on the midaxillary line at the level of the xiphoid and the fourth one was placed on the lower left thorax approximately 5 cm below the third electrode (Figure 1). A portable EC (ICON, Osypka Medical GmbH, Berlin, Germany) was connected to the sensor cable. The information from electrical impedance was recorded and parameters such as CO, TFC, SV variation (SVV) and flow time corrected (FTC) were calculated 3 times with 5-min intervals and stored on the device automatically. The data were then downloaded into a spreadsheet as continuous data for further analysis.
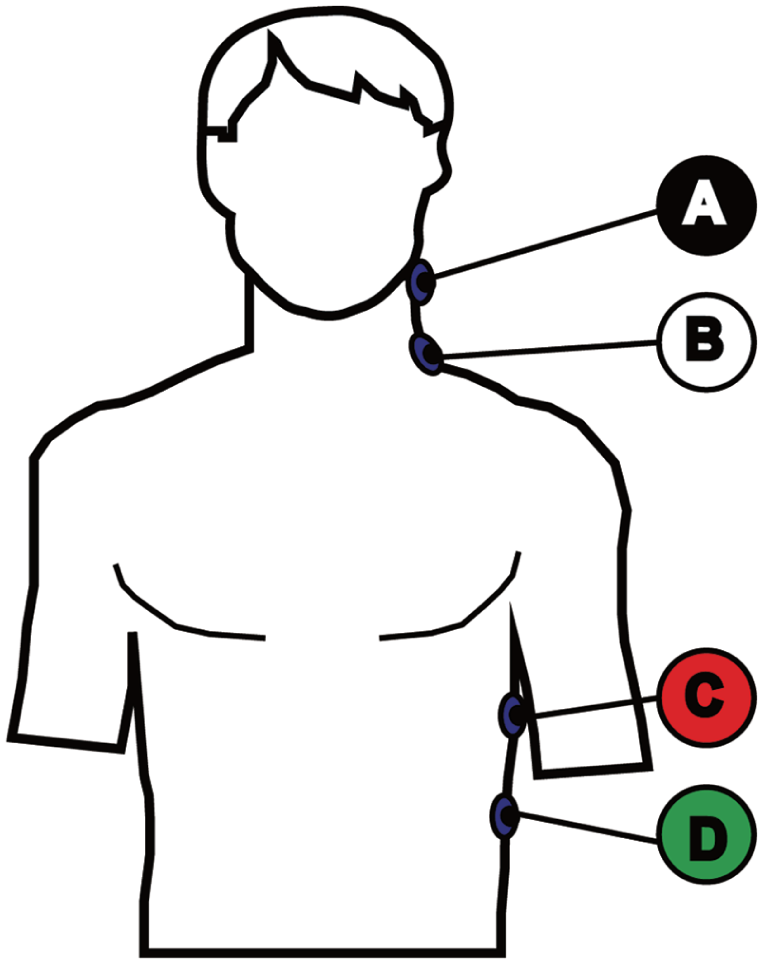
The electrical cardiometry sensors are located on the body surface.
Clinical outcome measurement
The primary outcome was mortality of pneumonia patients within 28 days of the ED visit. Secondary outcomes were length of hospital stay, measured in days, as the difference between the date of the ED visit and the date of discharge. Length of ICU stay was measured in days as the difference between the date of admission to the ICU and date of transfer to the general ward, including same-day transfers in the hospital.
Statistical analysis
Data were summarized as means and standard deviations for continuous normally distributed variables, frequencies and percentages for categorical variables. A chi-square test was used to compare discrete variables between the two groups. Fisher’s exact test or two-tailed Student’s t-test was used for comparison of continuous variables, as appropriate. Pearson’s correlation test was used to determine the strength of the relationship between two continuous variables. Logistic stepwise regression was performed with factors observed to be associated with mortality and ICU admission with a p value <0.20 when groups were compared. The adjusted odds ratios of mortality and ICU admission (95% confidence interval (CI)) were calculated for all independent factors. We generated receiver operating characteristic (ROC) curves for mortality at 28 days and ICU admission. The area under the ROC curve (AUC) and cut-off values were calculated using the Hanley–McNeil test. DeLong’s test was used to compare the ROC curves. All statistical procedures were performed using RStudio Version 0.98.932 (Boston, MA). Statistical significance was defined by p-values less than 0.05.
Results
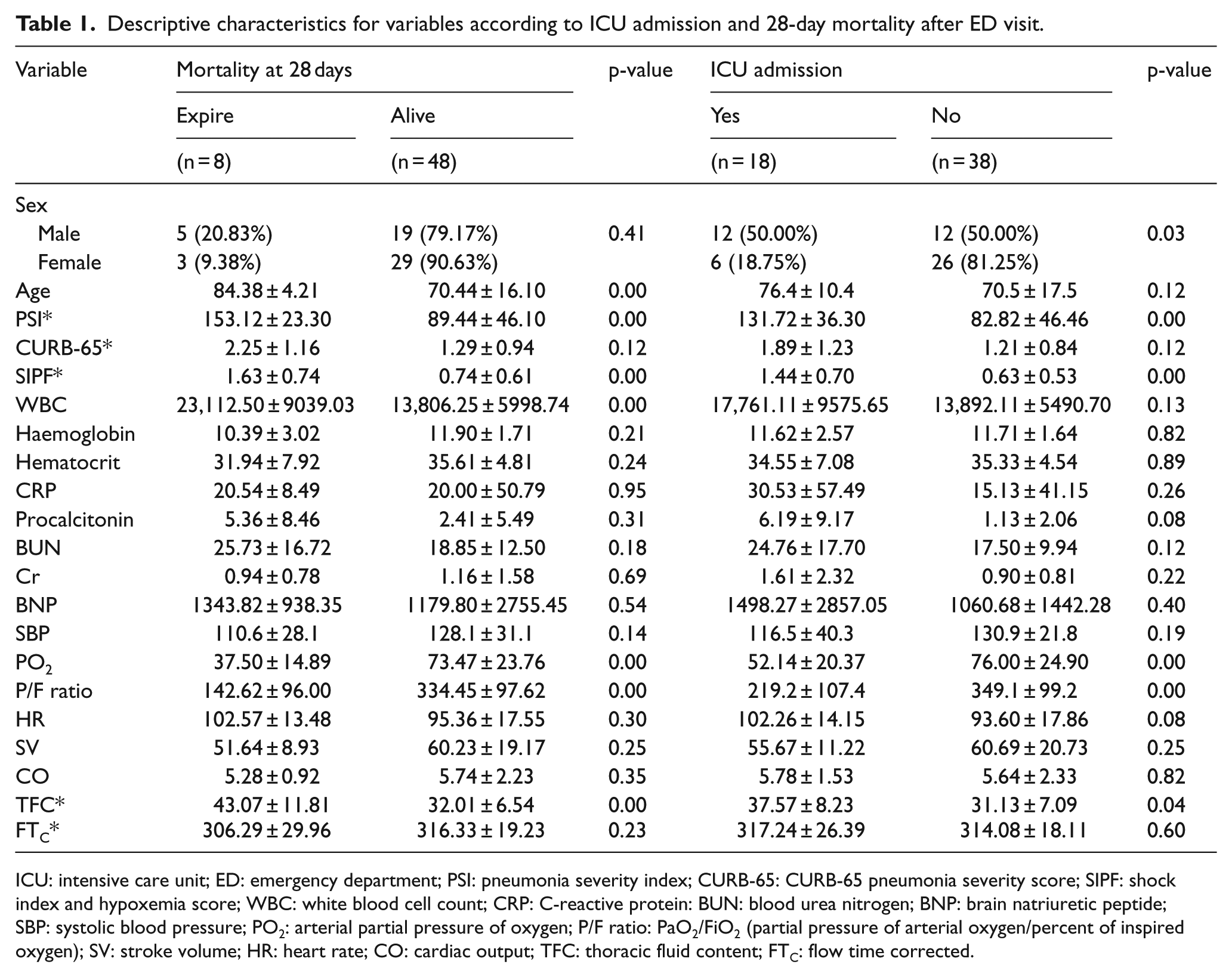
During the study period, 2,135 patients had ICD-10 codes corresponding to pneumonia, among the total of 22,752 patients aged 18 years or older who visited the ED. Overall, 368 patients were selected excluding those who had been transferred from other hospitals, who were discharged from ED and those without dyspnoea (Figure 2). Among them, EC monitoring was completed for 56 patients at the ED and fulfilled the clinical data collection criteria for analysis. There were 24 (42.9%) male patients and 32 (57.1%) female patients with age ranges of 30–106 years (72.08 ± 12.45). The mortality rate within 28 days was 14.28%, and the age within this group was higher than the survivors (p < 0.001); however, gender distribution was not associated with mortality. The PSI and SIPF scores were higher for expired patients than for those who survived (p < 0.001). White blood cell (WBC) count was significantly lower but the PaO2 and P/F ratio were significantly higher in those who survived. The CURB-65 score did not appear to be different between the two groups (Table 1).
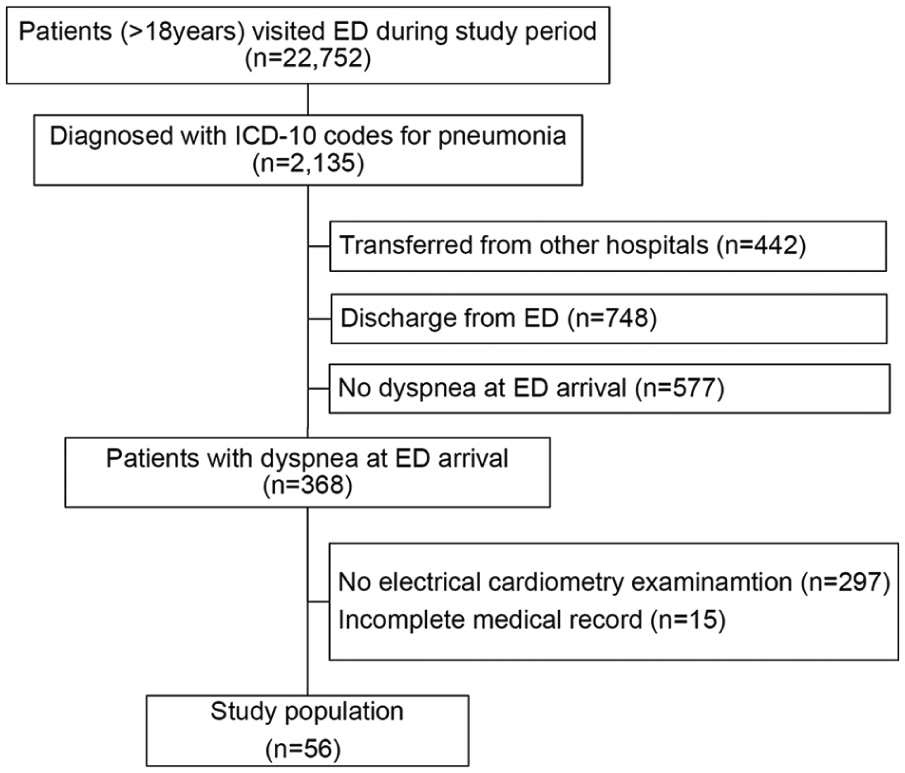
Stepwise selection of patients.
Descriptive characteristics for variables according to ICU admission and 28-day mortality after ED visit.
ICU: intensive care unit; ED: emergency department; PSI: pneumonia severity index; CURB-65: CURB-65 pneumonia severity score; SIPF: shock index and hypoxemia score; WBC: white blood cell count; CRP: C-reactive protein: BUN: blood urea nitrogen; BNP: brain natriuretic peptide; SBP: systolic blood pressure; PO2: arterial partial pressure of oxygen; P/F ratio: PaO2/FiO2 (partial pressure of arterial oxygen/percent of inspired oxygen); SV: stroke volume; HR: heart rate; CO: cardiac output; TFC: thoracic fluid content; FTC: flow time corrected.
A higher number of male patients were admitted to the ICU than female patients (Table 1). PSI and SIPF were higher in patients admitted to ICU but the CURB-65 scores were not. Patients admitted to the ICU had lower PO2; P/F ratio was related to ICU admission. The P/F ratio was most closely related to mortality and ICU admission (p < 0.01). Among the parameters obtained from EC, TFC was shown to be significantly higher in expired patients than those who survived (p = 0.03) and higher in those admitted to the ICU compared to those admitted to general wards (p = 0.05). The correlation coefficient between the TFC and P/F ratio was 0.37 with good correlation (p = 0.01).
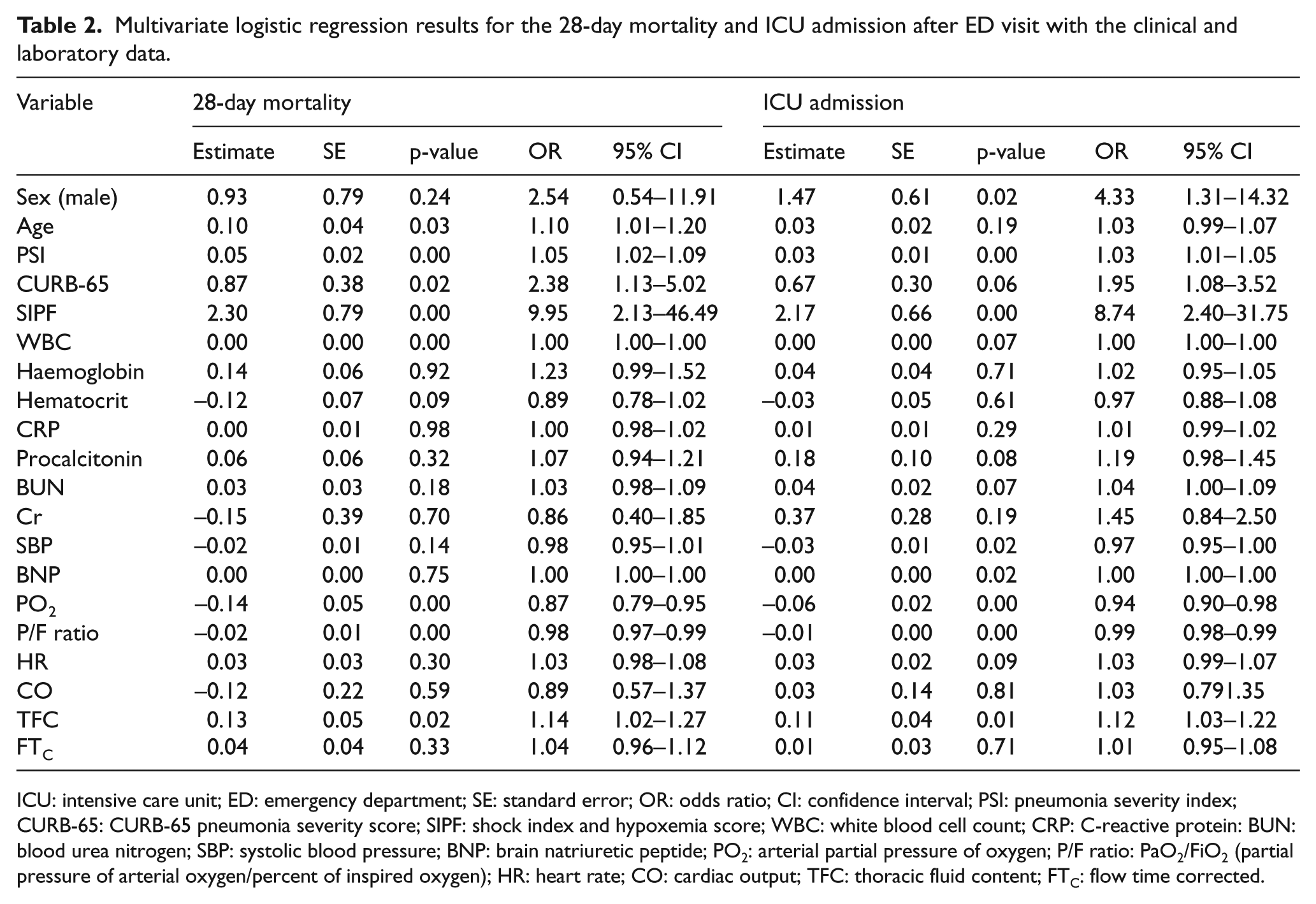
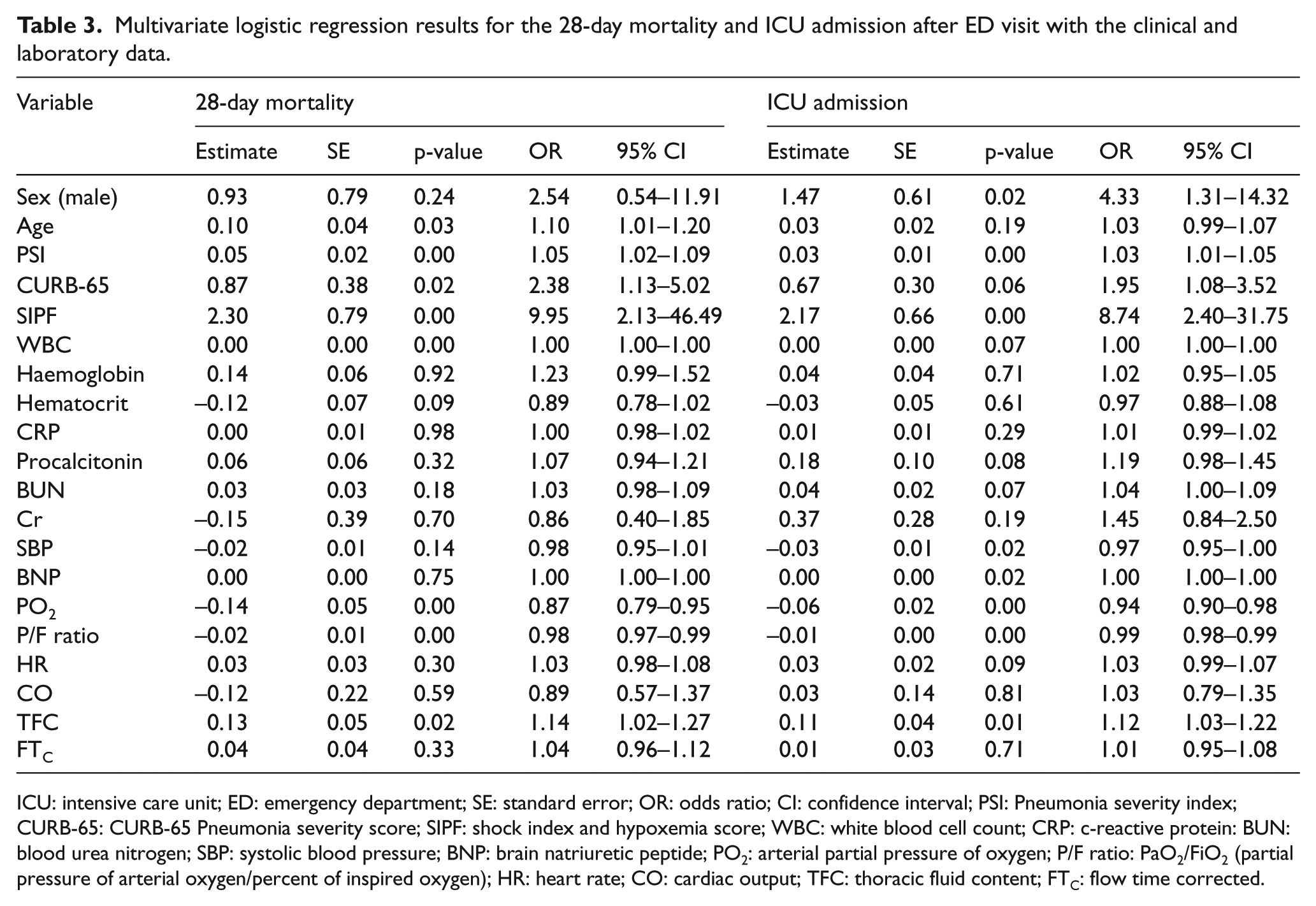
Factors including patient age, PSI, CURB-65, SIPF scores, WBC count, PaO2, and P/F ratio were significantly related to 28-day mortality based on the multivariate logistic regression (p < 0.05, Table 2). Of the parameters extracted from the EC, TFC was the most important parameter with a strong association to 28-day mortality (p = 0.03). Expired patients had a higher TFC value compared to survivors (43.07 ± 11.81 vs 32.01 ± 6.54) at ED (Table 2). The right half of Table 2 summarizes results from multivariate logistic regression for ICU admission. Male patients were prone to ICU admission compared to females (p = 0.02). The PSI, CURB-65 and SIPF scores were higher in those admitted to the ICU. The BNP (brain natriuretic peptide) level, PaO2 and P/F ratio were significant predictors for the ICU admission. TFC was also a factor associated with ICU admission (p = 0.01).
Multivariate logistic regression results for the 28-day mortality and ICU admission after ED visit with the clinical and laboratory data.
ICU: intensive care unit; ED: emergency department; SE: standard error; OR: odds ratio; CI: confidence interval; PSI: pneumonia severity index; CURB-65: CURB-65 pneumonia severity score; SIPF: shock index and hypoxemia score; WBC: white blood cell count; CRP: C-reactive protein: BUN: blood urea nitrogen; SBP: systolic blood pressure; BNP: brain natriuretic peptide; PO2: arterial partial pressure of oxygen; P/F ratio: PaO2/FiO2 (partial pressure of arterial oxygen/percent of inspired oxygen); HR: heart rate; CO: cardiac output; TFC: thoracic fluid content; FTC: flow time corrected.
We tried to identify the clinical and laboratory data from EC related to the length of ICU and hospital stay using the multivariate regression test. Average length of ICU stay was 10.7 ± 6.2 days for patients admitted to ICU. Factors associated with length of ICU stay were PSI, CURB-65, SIPF, procalcitonin, PaO2, the P/F ratio and TFC (Table 4). Of these factors, CURB-65 was only related to length of hospital stay. In addition, HR among the EC parameters was also related to the length of hospital stay (Table 3).
Multivariate logistic regression results for the 28-day mortality and ICU admission after ED visit with the clinical and laboratory data.
ICU: intensive care unit; ED: emergency department; SE: standard error; OR: odds ratio; CI: confidence interval; PSI: Pneumonia severity index; CURB-65: CURB-65 Pneumonia severity score; SIPF: shock index and hypoxemia score; WBC: white blood cell count; CRP: c-reactive protein: BUN: blood urea nitrogen; SBP: systolic blood pressure; BNP: brain natriuretic peptide; PO2: arterial partial pressure of oxygen; P/F ratio: PaO2/FiO2 (partial pressure of arterial oxygen/percent of inspired oxygen); HR: heart rate; CO: cardiac output; TFC: thoracic fluid content; FTC: flow time corrected.
The ROC curves plotted from the data are represented in Figure 3. The PSI and P/F ratio showed highest AUC values of 0.93 (95% CI, 0.75–1.00) and 0.93 (0.69–1.00), respectively, for prediction of 28-day mortality (Figure 3(a)). The AUC of TFC for 28-day mortality prediction was 0.72 (0.71–0.74) which was similar with the AUC of CURB-65. Only CURB-65 has a significantly lower AUC value than PSI from the DeLong’s comparison for ROC curves to compare the ability to predict 28-day mortality (Table 4). The prediction for ICU admission using all variables was associated with lower AUC values than the mortality prediction (Figure 3(b)). The PSI and P/F ratio was associated with the highest AUC value of 0.82 (0.69–0.91) and 0.82 (0.69–0.91), respectively, for ICU admission. And the PaO2 and PSI showed high AUC values for predicting ICU admission. TFC was associated ICU admission with an AUC value of 0.73 (0.62–0.82) which was comparable to the AUC of SIPF and PaO2. Based on DeLong’s comparison, there was no significant difference TFC’s predictability and that of other scores in predicting ICU admission (Table 4). CURB-65 showed the lowest predictability which was significantly lower than that of PSI for ICU admission. The cut-off value of TFC was found to be 36.0 (sensitivity = 71.4; specificity = 75.0) for 28-day mortality and 32.5 (sensitivity = 70.6; specificity = 68.4) for ICU admission (Table 5).
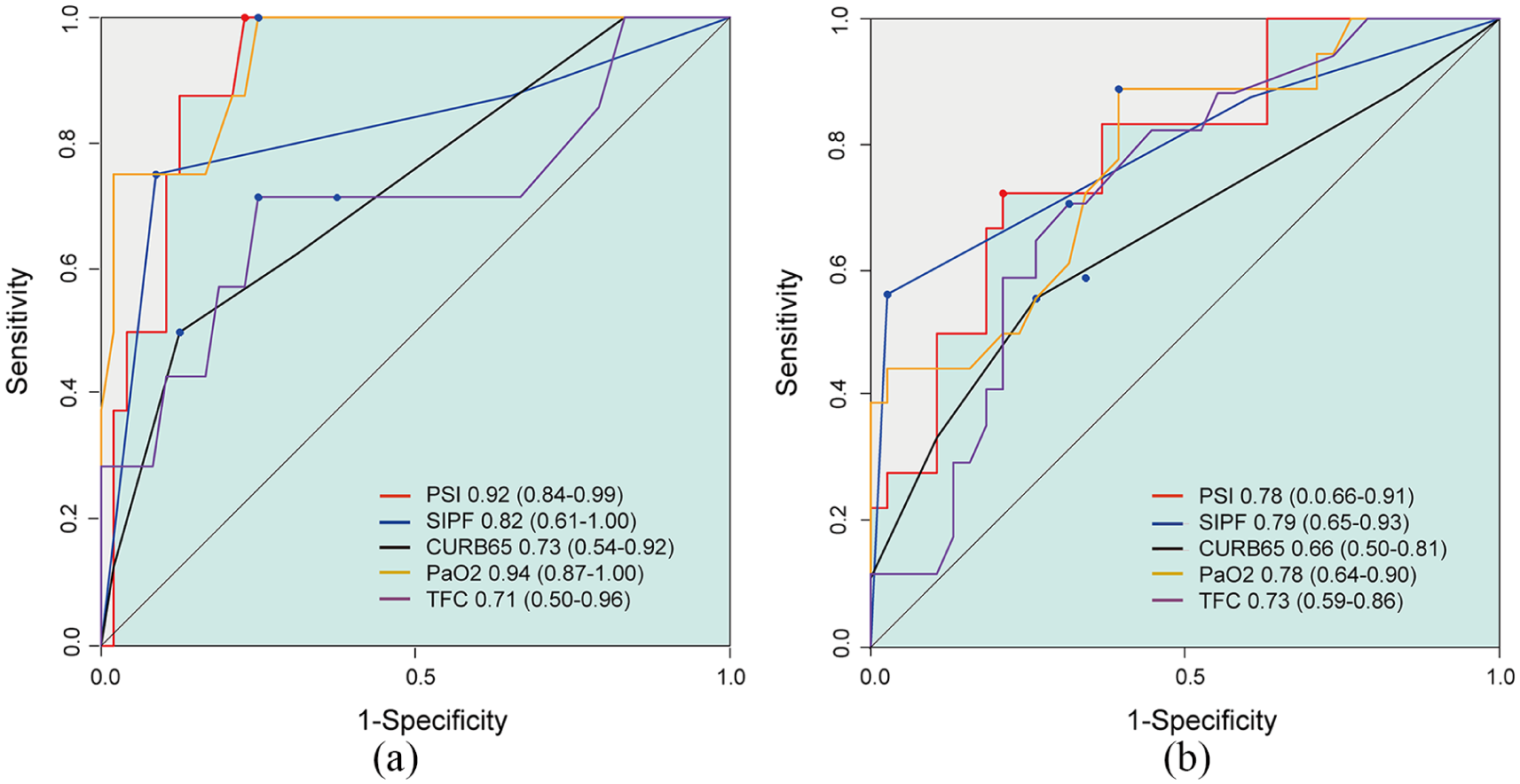
(a) Receiver operating characteristic (ROC) curve for the 28-day mortality is presented on left panel. (b) Right panel disclosed ROC curve for intensive care unit (ICU) admission. The values correspond to the area under the ROC curve (95% confidence interval).
DeLong’s paired comparison of the area under receiver operating characteristics curves for predicting 28-day mortality and ICU admission.
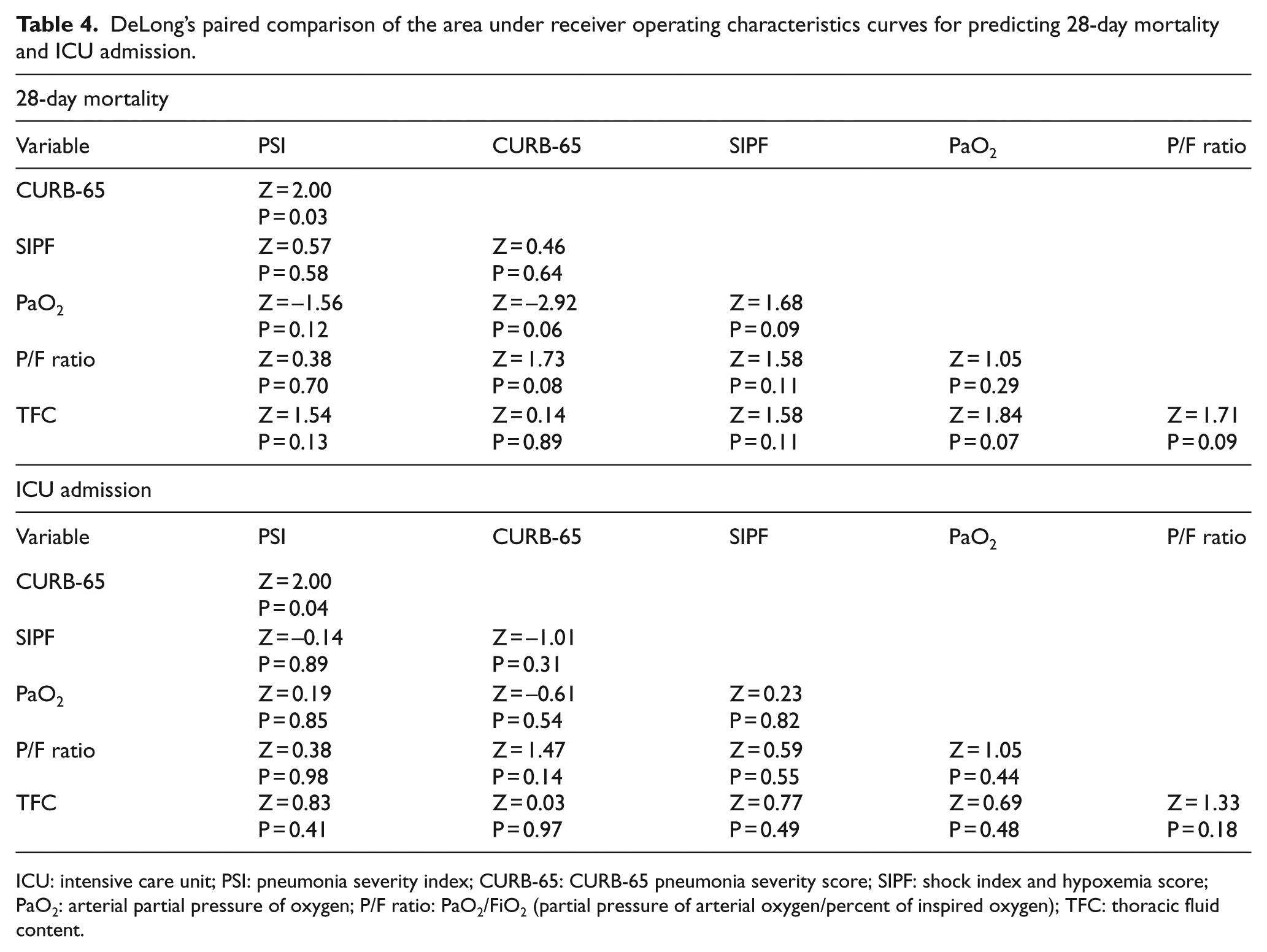
ICU: intensive care unit; PSI: pneumonia severity index; CURB-65: CURB-65 pneumonia severity score; SIPF: shock index and hypoxemia score; PaO2: arterial partial pressure of oxygen; P/F ratio: PaO2/FiO2 (partial pressure of arterial oxygen/percent of inspired oxygen); TFC: thoracic fluid content.
The values of the cut-off levels, the confidence interval, the sensitivity and the specificity of thoracic fluid content for prediction of 28-day mortality and ICU admission.
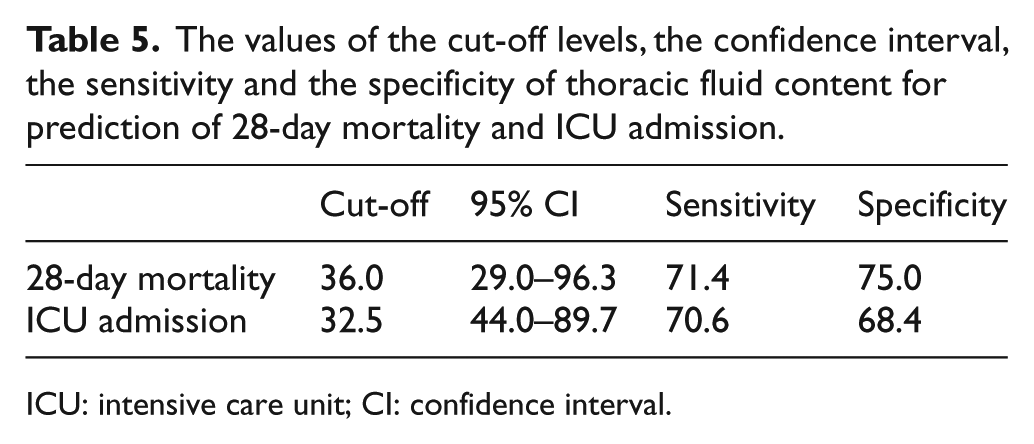
ICU: intensive care unit; CI: confidence interval.
Discussion
There is still no outstanding tool to predict the prognosis of pneumonia continuously at the bedside. Results from this study suggest that the EC monitoring may help in assessing prognosis of CAP patients in terms of length of hospital and ICU stay and 28-day mortality. Increased TFC is the single most useful parameter related to worse outcomes of CAP patients. EC monitoring allows additional benefits such as real-time measurements without inconveniencing the patient with invasive catheters.
Age is an important risk factor of CAP and plays an important role in the prognosis and disease severity of CAP. 13 Male sex is also associated with increased mortality and development of acute respiratory failure and sepsis/septic shock in CAP patients. 2 These reports are in accordance with this study, which showed significantly higher mortality rates in older patients and more number of ICU admissions in men.
A previous paper reported that procalcitonin level provides prognostic information regarding the severity of CAP, but measured CRP (c-reactive protein) level was not associated with the severity in accordance with this study. 14 Ito et al. 15 conducted a multivariate logistic regression analysis for prognostic factors in hospitalized CAP patients and reported that body P/F ratio, albumin level and BUN level were significantly associated with in-patient death. Ioanas et al. 16 also reported that no improvement in the P/F ratio after treatment in patients with severe pneumonia was an independent predictor of mortality. Both PaO2 and P/F ratio were significant predictive factors for 28-day mortality and ICU admission in this study. However, in contrast to past studies, this study found that BUN is not related to the prognosis of CAP patients.
Several severity scores have been proposed to predict outcomes of CAP patients and to support clinical decisions. First, the PSI was originally developed as part of the Pneumonia Patient Outcomes Research Team (PORT) project to come up with a clinically applicable prediction rule for evaluating short-term mortality among adult CAP patients. 4 The PSI score is frequently used to predict the need for hospitalization in patients with CAP. Patients in class I to III with a very low cumulative mortality rate of 0.1%, 0.6% and 0.9%, respectively, could be discharged with oral antibiotics; however, the patients with scores of 4 and 5 showed mortality rates of 9.3% and 27%, respectively. 17 The PSI score was also a good predictor for 28-day mortality in this study (class IV patients, 5.3%, and class V, 100%). The overall mortality rate for patients in this study was 14.2%, which is relatively higher than that usually reported for CAP patients. 4 This may be because the patients included were older than previous studies, and we only included patients who complained of dyspnoea on ED arrival.
It is difficult to identify 19 variables to calculate PSI in a busy ED where there are many patients. The SIPF score is the combination of shock index (HR/systolic blood pressure) >0.7 (=1 point) and P/F ratio <250 (=1 point). SIPF was reported as a good predictor of ICU admission than CURB-65 and PSI. 5 Results from this study also confirmed SIPF is a good predictor for ICU admission and mortality but discrimination ability of SIPF was not significantly excellent over PSI or CURB-65. CURB-65 is a simple pneumonia severity score that uses the five criteria which were mentioned at the ‘Introduction’ section, proposed by the British Thoracic Society. 2 Previous studies reported a high CURB-65 score was significantly associated with mortality, the need for mechanical ventilation and hospital admission in CAP patients. 18 The results from this study showed interim finding that CURB-65 has low power of mortality prediction and length of ICU stay but it has reasonable power of prediction for the length of hospital stay. Basically, CURB-65 was developed for adults under the age of 65 with less severe symptoms. 19 Low power of prediction of CURB-65 in this study might be associated with the high proportion of elderly patients. Findings from this study also confirmed that CURB-65 was only associated with length of hospital stay than mortality and ICU stay suggesting that CURB-65 may be more suitable for patients with less severity. 20
Despite the scoring system’s prognosis predicting power, it can be difficult to calculate using multiple parameters from clinical and laboratory results. In addition, it takes more than an hour to get laboratory results that are needed to obtain the PSI and SIPF, and we need an invasive procedure like arterial blood gas analysis. Pulse oximetry may be very helpful in evaluating pneumonia patients; a decrease in oxygen saturation of >3% from baseline or with random oxygen saturation of <94% was suggestive of pneumonia; 21 however, pulse oximetry only shows only oxygen bound to haemoglobin, not hemodynamic changes.
An EC is an advanced form of noninvasive thoracic impedance for hemodynamic monitoring. The electric current from the chest wall was able to easily run through the blood in the aorta. Dynamic blood flow aligns the red blood cells in the aorta during systole parallel to the blood stream from random orientation during diastole. The change from random orientation to uniform alignment of red blood cells generates a characteristic steep increase in conductivity or dZ(t). EC is likely to provide more accurate information on CO with only four electrodes on the body surface and is independent of the volume of the surrounding tissue than thoracic electrical bioimpedance. 22 In a previous meta-analysis, EC monitoring demonstrated acceptable reliability for measurement of CO in critically ill patients. 23 Another study showed EC provides accurate CO comparable to invasive methods using pulmonary artery catheters. 22 In addition to accuracy, these authors suggested that TFC from EC can be an indicator of CAP prognosis. This can be a noninvasive real-time bedside approach to assessing pneumonia patients and for making informed decisions.
Baseline thoracic electrical bioimpedance is inversely proportional to the baseline thoracic fluid level. When the fluid in the chest is increased, the bioimpedance is expected to decrease; on the contrary, bioimpedance is respectively expected to increase when the chest fluid volume is reduced. We can hypothesize that the reduction of thoracic impedance that resulted from the fluid filling in the airway could be associated with the outcome of acute CAP patients. Recently, a study reported that a separate peak of thoracic impedance during continuous measurement with implantable devices can detect evolving pneumonic infiltration very early prior to distinct clinical symptom development. 24 In this study, we reported decreased thoracic impedance, and therefore increased TFC could be explained by pneumonia with air space infiltration. The increased TFC could be indicative of outcomes of pneumonia even though pathogens were not identified.
TFC measured by noninvasive EC represents the amount of water in the interstitial and alveolar spaces of lungs including the pulmonary vasculature. EC measures full thoracic impedance and lung impedance is a small component of thoracic impedance and skin-to-electrode contact resistance is high. Therefore, the TFC from EC is considered to have low sensitivity for small changes in alveolar fluid at the area of pneumonic infiltration and congestion; however, a study by Hammad et al. 25 indicated that TFC from EC was excellent for detecting pulmonary oedema in eclampsia patients (AUC = 0.94) with good agreement with the EVLW (extra vascular lung water) measured by lung ultrasound (AUC = 0.96). From this study, AUC values were 0.71 for mortality prediction and 0.72 for prediction of ICU admission, which were lower than AUC values in the study of Hammad et al. 25 for eclampsia patients. This may be because pneumonic infiltration usually involves a focal area of lung while pulmonary oedema in eclampsia patients usually involves both lungs. Lower sensitivity and specificity for pneumonia may due to focal involvement of pneumonia and collection of exudative fluid.
On the other hand, we should consider the effects of pleural effusion, which is frequently observed in cases of severe pneumonia. Pleural effusion is a predictor of severe pneumonia and prognostic implications on mortality. 26 Zink et al. 27 demonstrate that changes in TFC due to thoracentesis in pleural effusion resulted in an increase in bioelectrical impedance. Thoracic bioelectrical impedance values before and after thoracentesis correlated with the volume of pleural effusion. These findings suggest that as the pleural effusion increases in severe CAP, the TFC also increases to reflect the outcomes.
We observed that the P/F ratio was an independent prognostic factor with the highest AUC value for 28-day mortality and ICU admission which is in accordance with some studies.28,29 TFC and P/F ratio disclosed good correlation and found to be associated with 28-day mortality in an independent manner. This finding suggests that the impairment in oxygenation during CAP is mainly contributed by the accumulation of lung water, as measured by TFC.
Limitations
There were several limitations to this research; it was a single-centre study with a small sample size and retrospective in nature. The EC measures resistance across the thorax, and resistance of pneumonic infiltration is a very small part of the total resistance. Thoracic impedance is more likely to be affected by other factors than pneumonic infiltration; however, we targeted more severe CAP patients with dyspnoea to reduce bias. There is a possibility of increasing the TFC due to the accumulation of blood volume in heart and major vessels in chest by sepsis and circulatory failure accompanying with dyspnoeic pneumonia patients. However, the possibility was very low because we excluded patients with underlying congestive heart failure (CHF) and heart disease, and there was no difference in comparison of CO, SV and FTC as an useful measure of preload (Table 1). EC monitoring was done only once at admission; however, EC variables may continue to change as patient conditions change.
Conclusion
EC monitoring demonstrated a new approach for assessing the prognosis of CAP patients. Increased TFC values may be related to worse patient outcomes including mortality and ICU admission. EC monitoring allows for real-time measurements of TFC without inconveniencing the patient with invasive catheters.
Footnotes
Acknowledgements
The authors confirm that the paper is original, is not under consideration by another journal, has not been previously published and has been prepared.
Author Contributions
The authors of this article contributed as follows: K.G., S.H.W. and S.H. designed the study. K.G., S.H.W., S.M.L., K.C.P., G.N.P., J.K. and S.H. collected data. S.H.W., G.N.P., J.K. and S.H. analysed data. K.G., K.C.P., G.N.P., J.K. and S.H. wrote paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data supporting the conclusions of this article are included within the article.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
This study was approved by the Institutional Review Board of Daejeon St. Mary’s Hospital (DC18RESI0109).
Human rights
The authors state that the study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.