
Abstract
Objectives and Background
Pelvic fracture causes significant mortality and morbidities. The purpose of this study is to identify the characteristics of patients with pelvic fracture in Hong Kong and to determine the factors predicting mortality. The result could help to identify high-risk patients who might benefit from more intensive evaluation and intervention.
Method:
Five hundred and eight patients (age > 12 years old) with pelvic fractures were identified from the trauma registries of four designated trauma centres in Hong Kong from 1 January 2005 to 31 December 2012. Patient baseline characteristics and outcomes were analysed. Stepwise logistic regression was performed to identify independent clinical predictors for mortality.
Result:
Mean age was 45.4 ± 19.2 years, 43.3% were female, mean length of hospital stay was 27.9 ± 42.4 days and mean length of intensive care unit stay was 4.8 ± 6.8 days. Injury severity score was 28.9 ± 18.7, revised trauma score was 7.2 ± 2 and 30-day mortality was 20.9%. Stepwise logistic regression identified patient’s age, presenting systolic blood pressure, initial Glasgow Coma Scale, injuries to the thoracic and abdominal regions, first base excess and the volume of red blood cell transfusion required within the first 6 h to be independent risk factors predicting mortality.
Conclusion:
Pelvic fracture is associated with significant risk of mortality in major trauma patients. Clinical characteristics obtained during emergency department resuscitation can help in selecting patients for timely aggressive interventions.
Introduction
Background
Major pelvic fractures are caused by high-energy trauma such as motor vehicle accident or fall from height. In the elderly population, pelvic fractures can also be caused by low-energy impact because of underlying osteoporosis.1,2 The primary cause of mortality in pelvic fracture is exsanguination.3,4 The bleeding sources are the bony fragment surface or injury to the adjacent veins and arteries. 5 Control of haemorrhage is the priority to save lives. Pelvic stabilisation with external fixation, preperitoneal pelvic packing 6 and arterial embolisation are the ways to tackle each of these bleeding sources. These procedures can improve the mortality of haemodynamically unstable pelvic fracture patients.7–9 The objectives of this study were to identify the characteristics of patients with fractured pelvis in Hong Kong and to determine predictors of mortality. There is limited information on the early clinical predictors of mortality among trauma patients with pelvic fractures. The results of this study helped to alert clinicians to initiate early intensive evaluation and more aggressive intervention for such patients.
Objective
The objective of this study is to report on the epidemiology of major pelvic fractures in Hong Kong and to identify predictors of mortality among trauma patients with pelvic fractures during early resuscitation period.
Methods
Study design
This was an unmatched case-control study on patients with pelvic fractures identified in the trauma registries of four designated trauma centres in Hong Kong, including Tuen Mun Hospital (TMH), Princess Margaret Hospital (PMH), Queen Elizabeth Hospital (QEH) and Queen Mary Hospital (QMH), from 1 January 2005 to 31 December 2012.
Hong Kong trauma registry
There are five designated trauma centres in Hong Kong, namely, TMH, PMH, QEH, QMH and Prince of Wales Hospital (PWH), under the management of the Hospital Authority (HA). Patients with major trauma would be diverted to one of these trauma centres dictated by ambulance protocols. Throughout the years since 2005, trauma patients who meet trauma team activation criteria, trauma cases transferred from other hospitals, trauma patients who are triaged as critical and emergency 10 in emergency department (ED), trauma death (however, death before arrival to ED is excluded) and trauma patients admitted to intensive care units (ICU)/high dependency units are captured in the trauma registry of the respective hospitals. The data collected include patient’s demographics, clinical parameters during ED resuscitation, mechanism of injuries and injury descriptors, namely, Abbreviated Injury Scale score (AIS), injury severity score (ISS) and revised trauma score (RTS). The total length of stay (LOS), outcomes (mortality/survival) and interventions given during pre-hospital, ED resuscitation and inpatient period are also recorded.
Patients
Patients were recruited from the dataset obtained for the ‘Dynamic MBT score’ study. 11 Secondary analysis of those patients with pelvic fracture was performed. Inclusion criteria included age > 12 years and ISS ⩾ 9. Pelvic fractures were diagnosed based on pelvic X-ray and computed tomography (CT) scan results. Patients with burn injury, drowning chronic renal failure, known chronic anaemia with haemoglobin ⩽ 8 g/dL or traumatic cardiac arrest were excluded. The primary outcome is all-cause mortality at 30 days with survivors being the control.
Clinical variables
Collected data included age, gender, mechanism of injury, types of pelvic fractures, vital signs (systolic blood pressure (SBP), heart rate, respiratory rate, Glasgow Coma Scale (GCS)) and investigation results (first haemoglobin level, haemoglobin drop, initial and subsequent base excess, initial and subsequent international normalised ratio (INR), initial and subsequent platelet counts). X-rays and CT scans were read independently by two emergency medicine specialists with disagreement adjudicated by a third senior physician to determine fracture types. These data were extracted from the trauma registries and also from the Clinical Data Analysis and Reporting System of the HA.
Statistical method
Patient baseline characteristics were reported as mean or median that where appropriate with standard deviations and interquartile range (IQR). Normality of continuous variables was tested using the Shapiro–Wilk test. Inter-group differences were analysed using Student’s t tests for parametric variables and Mann–Whitney’s U test for non-parametric variables. Chi-square/Fisher’s exact test is used for discrete variables. Stepwise logistic regression was performed to identify independent risk factors of 30-day mortality. Results were presented as odds ratio (OR) with the corresponding 95% confidence intervals (CI). A p value of <0.05 was regarded as statistically significant. Statistical analysis was handled by IBM SPSS Statistics version 25 and Microsoft Excel version 16.23.
Results
Pelvic fracture patients in Hong Kong
Patient characteristics
Between January 2005 and December 2012, 5151 trauma patients who met the inclusion criteria were identified from the four trauma registries of participating hospitals. In all, 4991 trauma patients were included for analysis after exclusion (Figure 1 and Table 1). Among them, 508 (10.2%) patients suffered from pelvic fracture. Their mean age was 45.4 ± 19.2 years with non-survivors being significantly older (mean difference = +11.7, p < 0.0005) and predominantly male (56.7%, p = 0.14).

Case eligibility and selection.
Patient characteristics and injury patterns.

PMH: Princess Margaret Hospital; QEH: Queen Elizabeth Hospital; QMH: Queen Mary Hospital; TMH: Tuen Mun Hospital; RTS: revised trauma score; ISS: injury severity score (1998); AIS: Abbreviated Injury Scale; SBP: systolic blood pressure; HR: heart rate; RR: respiratory rate; GCS: Glasgow Coma Scale; Hb: haemoglobin; INR: international normalised ratio; PT: prothrombin time; APTT: activated partial thromboplastin time; Plt: platelet; BE: base excess; Ext-Fix: external fixation; PPP: pre-peritoneal packing; FAST: focused assessment with sonography in trauma; MTP: massive transfusion protocol; MBT: massive blood transfusion; RBC: red blood cell; FFP: fresh frozen plasma; Cryo: cryoprecipitate; IQR: interquartile range; CT: computed tomography.
Mechanism of injury
The mechanism for pelvic fracture was mostly fall from height (fall more than 2 m, 37.4%) and pedestrians involved in a road traffic accident (33.5%). Vehicle drivers, passengers and motorcyclists contribute around 13%.
Injury severity and injury pattern
The mean ISS was 28.9 ± 18.7 and mean RTS was 7.2 ± 2. In all, 27% of our cohort suffers from unstable pelvic fractures (defined as Youngs and Burgess Classification anteroposterior compression type II and III, lateral compression type II and III, vertical shear and combined mechanism). Pelvic fracture was commonly associated with severe injuries of other organs (AIS > 2). Among our patients, 66% had injury to extremities, 48% had thoracic injury, 40.9% had head and neck injury and 17% had abdominal injury.
Morbidity and mortality
The overall 30-day mortality was 20.9%. Among survivors, the mean hospital LOS was 27.9 ± 42.4 days and the mean ICU LOS was 4.8 ± 6.8 days.
Factors associated with mortality in pelvic fracture patients
Univariate analysis was performed for potential early clinical predictors of mortality. Stepwise logistic regression was then done to identify independent predictors. It was noted that age, presenting SBP, presenting GCS, injuries to the thoracic and abdominal regions, first base excess and the volume of red blood cell transfusion within the first 6 h were significant independent risk factors predicting mortality in major pelvic fracture patients (Table 2).
Univariate analysis and multiple logistic regression analysis.

Logistic Model R2 = 0.687, SBP: systolic blood pressure, Hb: hemoglobin, RBC: red blood cell, PLT: platelet, INR: international normalised ratio, FFP: fresh frozen plasma, BE: base excess, GCS: Glasglow coma scale, Ext-Fix: external fixation, FAST: focus assessment with sonography for trauma, MTP: massive trasfusion protocol
Among these factors, GCS has the best predicting power, with an area under the receiver operating characteristic (ROC) curve of 0.832, with the best cut-off at 13 with sensitivity of 0.84 and specificity of 0.78. A GCS of less than 9 has a specificity of 90% for mortality while a GCS of 3 is 96% specific (Figure 2, Table 3).

ROC curves.
ROC curve analysis.
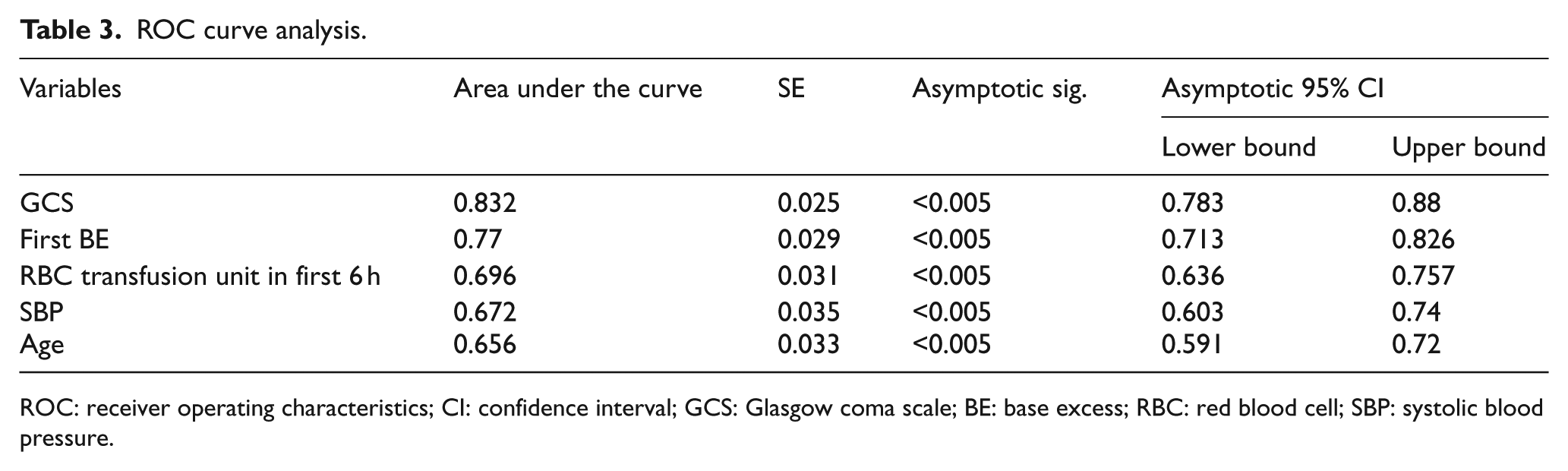
ROC: receiver operating characteristics; CI: confidence interval; GCS: Glasgow coma scale; BE: base excess; RBC: red blood cell; SBP: systolic blood pressure.
Discussion
Key results
Reported mortality rate of pelvic fracture in trauma patients from previous studies ranged from 5% to 20%.1,2,12–19 In this study, the 30-day mortality rate was 20.9%. With such high mortality risk, strategies8,9,20 were developed to tackle pelvic fracture. For example, concurrent preperitoneal packing, external fixation and pelvic arteries embolisation (3-in-1 pelvic damage control procedure) have been shown to improve survival.8,9 This study was conducted to determine useful early predictive factors to identify patients with more severe injury and higher mortality. This group of patients could benefit from immediate aggressive early intervention.
Many countries and trauma systems have examined predictors of mortality for pelvic fracture patients.18,19,21–24 Age, the presence of shock, a high ISS, blood products requirement, multiple injuries, traumatic brain injury or depressed GCS was consistently found to be predictive of mortality. However, many of the above parameters, for example, ISS, are not available during the initial resuscitation, making it less useful during initial trauma resuscitation in the ED.
Studies using only early predictors of mortality in patients suffering from pelvic fractures are scarce. Starr et al. reported the relationship between survival with age, SBP on arrival, base deficit, fracture pattern and RTS in 325 patients with mean ISS around 18. 12 Giannoudis et al. reported, in a cohort of 11,149 patients with median ISS of 9, that age, physiologic derangement, and associated head, chest, and abdominal injuries abdominal injuries predict their mortality. And liver injury was found to carry the most significant impact on survival. 19
In our study, we identified that age, presenting SBP, initial GCS, injuries to the thoracic and abdominal regions, first base excess and the volume of red blood cell transfusion required within the first 6 h were independent risk factors predicting mortality. Most of the above parameters could be obtained at the bedside during resuscitation in the ED and initial observation, with the advent of point-of-care testing, base excess and haemoglobin level are easily obtainable at the bedside.
GCS is a significant predictive factor for mortality. Its association with mortality persisted after multiple logistic regression suggesting that death associated with decreased consciousness was concomitant direct trauma brain injury rather than physiological derangement. From our statistical result, each point of GCS < 15 decreased the odds of survival by 28%. A GCS of <9 was 90% specific for mortality. In trauma patients with unstable haemodynamics, permissive hypotension was advocated to decrease bleeding and transfusion requirement. However, permissive hypotension was contraindicated in the patients with severe trauma brain injury. The struggle to maintain adequate cerebral perfusion could result in increased bleeding and blood product requirement. Apart from more difficult resuscitation, patients with severe traumatic brain injury might be deemed as having poor neurological outcome despite resuscitation. So, many of them would be offered conservative or palliative treatment. In this way, it is important to identify patients with severe brain damage in the early phase of resuscitation and treatment.
Major pelvic fractures were resulted from high energy trauma, which was frequently associated with significant injuries to the thorax and abdomen. The mortality for major thoracic injury, for example, massive haemothorax, and uncontrolled intra-abdominal bleeding was extremely high which explained the concomitant thoracic or abdominal injury to be two of the major predictors of mortality for patients with major pelvic fractures. In our analysis, the presence of significant (AIS > 2) thorax and abdominal injuries increases the OR for mortality by >300%.
Previous studies found that specific fracture pattern was not predictive of patient’s outcome.4,24 Fracture stability was shown to be a predictive factor of mortality in our study during univariate analysis. However, it was found to be insignificant after multivariate logistic regression analysis; this suggested fracture stability was confounded by the trauma severity; its significance vanished when more direct indicators of trauma severity were analysed together.
Limitation
This study was a retrospective analysis of data from four trauma centres in Hong Kong, and it was subjected to the same limitations of all retrospective studies. When determining the independent predictors of mortality, patient comorbidities and functional status were not considered. As the population ages with more people suffering from chronic medical conditions, a large proportion of trauma patients are suffering from comorbid conditions. Furthermore, we only measured mortality; yet, patient’s functional outcomes and quality of life were not examined. Functional recovery in a trauma patient is an important outcome. Since the study included data over an 8-year period from 2005 to 2012, the management of unstable pelvic fracture has gradually changed, with more trauma centres adopting the 3-in-1 pelvic damage control protocol which is a multidisciplinary approach and was shown to significantly reduce the mortality of major pelvic fracture patients in recent local studies.8,9 In all, 9.6% of our current study cohort has undergone the 3-in-1 procedure. Cheng et al. 8 reported that 46% of patients received the 3-in-1 procedure in a cohort of patients with haemodynamic instability and unstable pelvic fractures. Therefore, the predictive factors of mortality may be different after more widespread use of the 3-in-1 procedure.
Conclusion
Mortality related to major pelvic fracture remains high despite the multidisciplinary management in major trauma centre. Therefore, we recommend that aggressive monitoring and treatment should be instituted promptly for patients with pelvic fracture presenting with hypotension, elevated base excess and depressed GCS; associated with thoracic or abdominal injuries or requiring early transfusions. Point-of-care test is useful as an adjunct in the management of trauma patients.
Footnotes
Acknowledgements
We would like to acknowledge Dr Mina Cheng, Dr Chak Wah Kam, Dr Gilberto Leung and Dr Siu Man Li who worked on the original dataset.
Author contributions
W.Y.K., M.Y. and O.F.W. conceived the study. W.Y.K. and M.Y. did literature search, statistical analysis, and first draft of the manuscript. W.O.F., C.T.L. and K.L.T. were responsible for reading the X-ray films, ethical approval, and synthesis of the original dataset and revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data
The datasets generated and/or analysed during the current study are available. It has been uploaded to the publisher’s website.
Informed consent
Informed consent was not sought for the present study because this is a retrospective study.
Ethical approval
Ethical approval was not sought for the current study because it is a subgroup analysis of prior data. Ethical approval was obtained from the ethical review board of the four trauma centres for the prior dataset (approval reference: KC/KE-13-0243/ER-1, KW/EX-14-089(75-01), UW 15-550, NTWC/CREC/1161/13).
Human right
Human right is protected. This is a retrospective analysis of clinical data. No information identifiable to individuals has been collected and stored.